J Clin Aesthet Dermatol. 2019;12(12):E58–E63
 by Yohei Tanaka, MD, PhD
by Yohei Tanaka, MD, PhD
Dr. Tanaka is with the Clinica Tanaka Plastic and Reconstructive Surgery and Antiaging Center in Matsumoto, Japan.
FUNDING: No funding was provided for this study.
DISCLOSURES: The authors have no conflicts of interest relevant to the content of this article.
ABSTRACT: Background: Radiofrequency energy has been shown to penetrate deeper into the skin, independent of skin color, and to be beneficial for skin tightening. It was previously reported that multisource, phase-controlled radiofrequency treatments provide safe and effective skin tightening and rejuvenation. The present study evaluated the effectiveness of multisource, phase-controlled radiofrequency treatments with a unique concentric electrode configuration for skin tightening.
Methods: Twenty-five Japanese patients were treated with the novel multisource phase-controlled radiofrequency system. Digital photographs and three-dimensional imaging were used to evaluate the results. The patients also provided subjective assessments.
Results: Objective assessments with digital photographs and superimposed three-dimensional color images showed significant volumetric reduction in the treated areas. Ninety-six percent of patients reported satisfaction with the results, and all patients reported satisfaction with the convenience of the procedure. Complications were minor and transitory, consisting of a slight burning sensation and mild erythema, which resolved within one hour of treatment. No side effects were observed.
Conclusions: The multisource phase-controlled radiofrequency treatments evaluated in this study showed efficacy with minimal discomfort and side effects. Repeated treatments using this method can provide an alternative to more invasive tightening treatments.
KEYWORDS: Multisource, phase-controlled radiofrequency, skin tightening, volumetric reduction
Demand for a noninvasive and long-lasting treatment to reduce undesirable fat tissue and to induce skin tightening has grown dramatically over the past few decades as new aesthetic technologies have been introduced into practice.1 A major cause of wrinkles, laxity, and cellulite is the reduction in the quantity and quality of collagen in the dermis and hypodermis.1 The author has previously reported that near-infrared can penetrate deep into human tissue to achieve skin tightening2–7 and that multisource, phase-controlled radiofrequency (RF) treatments provide safe and effective long-term stimulation of elastin, which is beneficial for skin rejuvenation by improving skin laxity and wrinkles.8–14
RF devices have also been widely used for skin tightening, and are thought to heat the dermis and subcutaneous tissues, thereby stimulating dermal collagen remodeling.8–14 One of the effects of dermal heating is an immediate change in collagen structure, followed by long-term stimulation of neocollagenesis beginning 4 to 6 weeks after treatment.15 These thermal effects can help reduce the appearance of wrinkles and laxity and improve contours on both the face and body.1
The thermal effects of monopolar and bipolar RF have demonstrated efficacy in skin tightening.1 Nevertheless, these effects are often partial or unpredictable, due to the uncontrolled nature and possible pain produced during monopolar or unipolar RF treatments and the superficial nature of energy flow for bipolar or tripolar configurations.1 In addition, these first-generation RF therapy systems lack the ability to adjust the delivered power based on differences in individual skin impedance.
In the author’s previous research, multisource, phase-controlled RF systems with six independent RF generators were used.8–14 Each of these generators are phase-controlled, allowing for a complex three-dimensional (3D) interaction to occur between the electromagnetic fields produced in the tissue. Since adjacent electrodes, on each side of the handpiece, posses identical polarities, no current is created between these electrodes on the skin’s surface, and most of the energy is driven deeper into the skin with minimal epidermal flow.8–14 In addition to the RF delivery technology, the tested system facilitates continuous real-time measurement of skin impedance and delivers constant energy to the patient’s skin, independent of changes in its impedance.
In this study, a novel, multisource, phase-controlled RF system with four concentric electrodes specially designed to deliver focused energy was used (Figure 1) and provided both patient-reported and objective, clinical evidence of skin tightening.

Methods
Patients. Twenty-five Japanese patients (20 women and five men) aged 27 to 72 years (mean age: 52.80±13.89 years) with Fitzpatrick Skin Types III and V were enrolled in this study. All of the patients had visited the Clinica Tanaka Anti-aging Center to reduce undesirable fat tissue and to seek skin tightening of the face and body. Twenty-five patients received treatment on the face, and 3 out of 25 patients were also treated on the abdomen and legs. None of the patients had a history of any type of skin disease or cosmetic procedure that affected the treatment areas. The patients did not use any specific skincare products and had no specific diet. Patients who exhibited weight loss during the study period were excluded from volumetric measurement analyses, because changes in diet and/or exercise might affect volumetric changes. After reading the experimental protocol and being advised of the treatment risks, all patients gave written informed consent for participation in the study. Informed consent to participate in the study and consent for the use of photos were received from all patients. The study followed ethical principles described in the current revision of the Declaration of Helsinki.
RF treatment. The RF device used in this study was a Mini-Shaper treatment handpiece and an EndyMed PRO™ treatment system (EndyMed Medical; Caesarea, Israel), which is a multisource, phase-controlled RF system that emits at a 1-MHz frequency at 1 to 50W. The patients’ faces were treated at 25 to 30W, while the abdomen and legs were treated at 50W. If the patient reported a strong sensation of heat, scanning was performed slightly faster and/or the treatment head was moved slightly away from the point of heat sensation. The patients were treated until they experienced a burning sensation and mild erythema. No oral analgesics were administered before, during, or after the treatment. In addition, no skin cooling was required. Three to five treatment sessions with one-month intervals between treatments were performed.
The electrode surface area is 9cm2, prompting approximately a 250-percent increase in the effective treatment area compared to the handpiece for face and neck treatments used in the author’s prior studies (Figure 1). Thermal images of the Mini-Shaper RF device used in the present study showed deeper penetration and a higher temperature of 2.9 degrees at 4mm in depth compared to the handpiece used in the author’s prior studies (Figure 2). A representative thermal image (Figure 3) of the RF device used in the study shows a high therapeutic temperature in the patient’s jawline and knees. The unique concentric electrodes provide superior volumetric heating, with deeper average heating depth.


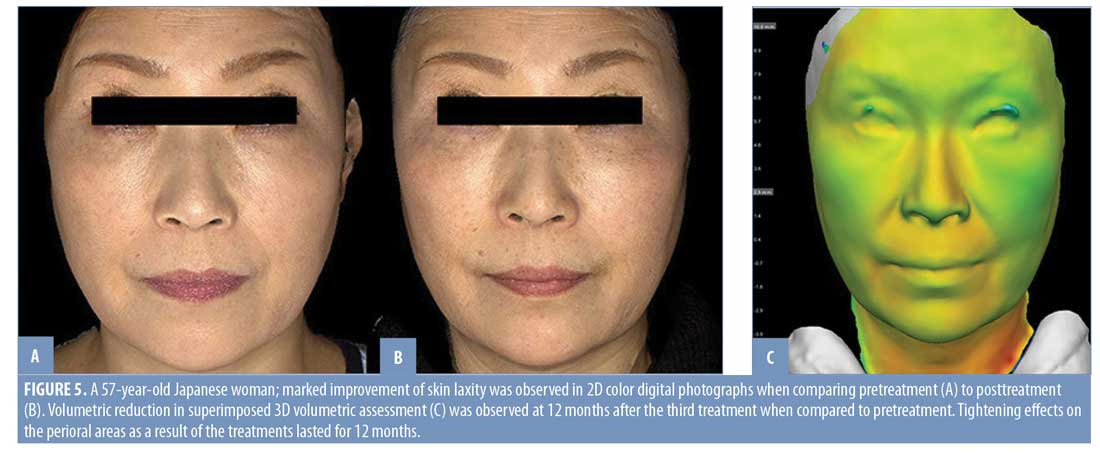
Objective assessments. Digital photographs and 3D imaging were used as objective assessments and acquired with a Canfield Scientific Vectra Handy camera and software (Canfield Scientific Inc., Fairfield, New Jersey). This system is designed to accurately capture the surface shape and two-dimensional (2D) color information of the human body. The superimposed 3D color schematic representations were used to indicate the volumetric changes between pretreatment and posttreatment, and shows the varying degrees of tightening in colors that range from yellow to red (red: -5mm change). Green areas indicated no changes to the face, while gray areas indicated changes of more than 5mm. Three-dimensional volumetric assessments were performed up to 12 months after the treatment.
Subjective assessments. Subjective assessments were performed using questionnaire data collected 12 months posttreatment. Patients rated their degree of satisfaction with improvement of the treated area and convenience of the procedure. Scores were based on a five-point scale, ranging from 0 to 4 points (0=worse; 1=little satisfaction or not satisfied; 2=fairly satisfied; 3=satisfied; 4=very satisfied).
Results
All twenty-five patients completed a treatment course of more than three treatments using the novel multisource phase-controlled RF system. Objective assessments with digital photographs and superimposed 3D color images showed marked volumetric reductions in the treated faces. Representative 2D color images and superimposed 3D color images are presented in Figures 4, 5, and 6. Marked volumetric reduction in the treated body area can be observed in 2D color digital photographs compared to pretreatment in Figures 7 and 8. Ninety-six percent of patients reported satisfaction with the results, and all patients reported satisfaction with the convenience of the procedure (Figure 9). The mean degrees of satisfaction with the results and convenience of the procedure based on a five-point scale from 0 to 4 points were 3.12±0.83 and 3.28±0.84, respectively. Complications were minor and transitory, consisting of a slight burning sensation and mild erythema, which resolved within one hour posttreatment. Most of the patients did not report feeling pain during the RF treatment, even though therapy was performed without anesthesia and contact cooling. Side effects, such as epidermal burns, adipose tissue atrophy, and contraction were not observed, and the patients felt comfortable throughout the study.





Discussion
In our clincal experience, skin tightening procedures to improve skin laxity and contours of the face and body, regardless of age or skin type, are among the most common requests from patients. Although invasive procedures, such as liposuction or surgeries, are effective in improving contours and reducing undesirable fat tissue, the postprocedure downtime and scar formation are not desirable. Ablative procedures, such as laser resurfacing, are effective in skin tightening; however, the downtime and potential adverse effects, such as hyper- and hypopigmentation, are also not desirable. Noninvasive skin tightening procedures can be particularly applicable to skin of color, such as that of Asian patients, because such procedures are independent of skin type.16 Whereas nonablative skin rejuvenation heats up the superficial dermis, deep tissue heating that involves RF, laser, or near-infrared sources aims to induce thermal injury in the deep tissue.17 The aim of deep tissue heating is to stimulate new collagen formation, which can achieve skin tightening. RF treatment is capable of volumetric heating of the mid-to-deep dermis, as well as selective heating of the fibrous septa strands and fascia layer.18 Specifically, RF energy heats hydrodermal collagen, promoting both collagen remodeling and skin tightening.19 Clinically, these effects promote dermal collagen production and the tightening of these deep subcutaneous structures.18 RF devices have been used in thermal delivery systems to provide the beneficial effects of heat while avoiding some of the downfalls of more standard lasers.20
In this study, the novel multisource phase-controlled RF system was used, which allows for continuous, real-time measurement of skin impedance and the delivery of constant energy to the patient’s skin, independent of changes in its impedance. Using the multisource phase-controlled RF system, less thermal damage of the dermis and subcutaneous tissues occurs compared to during monopolar or unipolar RF treatments. The author evaluated the efficacy of the multisource, phase-controlled RF treatments both subjectively and objectively and found that the treatments provide satisfactory results without notable side effects. Furthermore, most of the patients reported being satisfied with the improvements in skin laxity and did not report feeling pain during the treatment, even though therapy was performed without anesthesia and contact cooling.
Although the volumetric measurement was performed 12 months after the final treatment, marked volumetric reduction and skin tightening were observed compared to the pretreatment volume in all of the patients. Since the effects of this RF treatments are clinically observed for at least 12 months after the treatment, further studies of volumetric assessments with a longer follow-up time periods are needed.
Side effects, such as epidermal burns, adipose tissue atrophy, and contraction were not observed, and the patients felt comfortable throughout the study. Further research is necessary to determine if a higher output, increased frequency of treatments, or longer periods of treatment can be even more effective.
Limitations. It should be noted that this was a preliminary study that included a fairly small number of patients. Moreover, we cannot exclude the possibility that lifestyle habits, such as food, alcohol, and salt intake might impact the changes observed in this study. Therefore, larger studies with longer posttreatment periods are warranted in order to evaluate variations in treatment parameters and correlations with patients’ environmental factors. In addition, the lack of a control group and the lack of a comparison between dosage strengths and frequencies limit the significance of our findings.
Conclusion
Using multisource, phase-controlled radiofrequency treatments with a unique concentric electrode configuration, the author found significant improvements in contours and skin laxity through objective assessments, and most patients reported being satisfied with the results. The major advantage of the multisource phase-controlled RF system is its long-lasting efficacy. Moreover, this technique produced minimal complications and downtime, as well as few side effects. Overall, this noninvasive, multisource, phase-controlled RF approach provides safe, long-lasting, and effective treatment of skin tightening.
References
- Elman M, Harth Y. Novel multi-source phase-controlled radiofrequency technology for non-ablative and micro-ablative treatment of wrinkles, lax skin and acne scars. Laser Therapy. 2011;20(2):139–144.
- Tanaka Y, Matsuo K. Non-thermal effects of near-infrared irradiation on melanoma. Tanaka Y, ed., Breakthroughs in Melanoma Research. London, UK: IntechOpen; 2011: 597–628.
- Tanaka Y, Gale L. Beneficial applications and deleterious effects of near-infrared from biological and medical perspectives. Optics and Photonics Journal. 2013;3(4A):31–39.
- Tanaka Y, Tsunemi Y, Kawashima M, et al. Objective assessment of skin tightening using water-filtered near-infrared (1000–1800 nm) device with a contact cooling and freezer stored gel. Clin Cosmet Investig Dermatol. 2013;6: 167–176.
- Calderhead G, Tanaka Y. Photobiological basics and clinical indications of phototherapy for skin rejuvenation. In: Tanaka Y. Photomedicine: Advances in Clinical Practice. London, UK: IntechOpen; 2017: 215–252.
- Tanaka Y. Beneficial applications of near-infrared irradiation in laser treatment field. In Japanese. The Journal of Japan Laser Therapy Association. 2018;17:24–27.
- Tanaka Y. Nakayama J. Up-regulated expression of La ribonucleoprotein domain family member 6 and collagen type I gene following water-filtered broad-spectrum near-infrared irradiation in a 3-dimensional human epidermal tissue culture model as revealed by microarray analysis. Australas J Dermatol. 2018;59(2):e87–92.6.
- Tanaka Y. Objective assessment of skin tightening using multisource, phase-controlled radiofrequency in Asians. J Cosmet Dermatol Sci Applications. 2013;3:110–116.
- Tanaka Y, Tsunemi Y, Kawashima M, et al. Treatment of skin laxity using multisource, phase-controlled radiofrequency in Asians: – Visualized three-dimensional skin tightening results and increase in elastin density shown through histological investigation. Dermatol Surg. 2014;40(7):756–762.
- Tanaka Y. Long-term three-dimensional volumetric assessment of skin tightening using a sharply tapered non-insulated microneedle radiofrequency applicator with novel fractionated pulse mode in Asians. Lasers Surg Med. 2015;47(8):626–633.
- Tanaka Y. Long-term skin tightening effects of a sharply tapered non-insulated microneedle radiofrequency applicator with novel fractionated pulse mode shown through three-dimensional volumetric assessment. Australas J Dermatol. 2016;57(1):78.
- Gold M, Taylor M, Rothaus K, Tanaka Y. Non-insulated smooth motion, micro-needles RF fractional treatment for wrinkle reduction and lifting of the lower face: International study. Lasers Surg Med. 2016;48(8):727–733.
- Tanaka Y. Long-term nasal and peri-oral tightening by a single fractional non-insulated microneedle radiofrequency treatment. J Clin Aesthet Dermatol. 2017;10(2):45–51.
- Tanaka Y. Treatment of skin laxity using multisource, phase-controlled radiofrequency. In: Vereecken P. Dermatologic Surgery and Procedures. London, UK: IntechOpen; 2018;175–192.
- Sadick N, Sorhaindo L. The radiofrequency frontier: a review of radiofrequency and combined radiofrequency pulsed light technology in aesthetic medicine. Facial Plastic Surg. 2005;21(2):131–138.
- Chan HH, Yu CS, Shek S, et al. A prospective, split face, single-blinded study looking at the use of an infrared device with contact cooling in the treatment of skin laxity in Asians. Lasers Surg Med. 2008;40(2):146–152.
- Dierickx CC. The role of deep heating for noninvasive skin rejuvenation. Lasers Surg Med. 2006;38(9):799–807.
- Kist D, Burns AJ, Sanner R, et al. Ultrastructural evaluation of multiple pass low energy versus single pass high energy radio-frequency treatment. Lasers Surg Med. 2006;38(2): 150–154.
- Zelickson BD, Kist D, Bernstein E, et al. Histological and ultrastructural evaluation of the effects of a radiofrequency based nonablative dermal remodeling device: a pilot study. Arch Dermatol. 2004;140(2):204–209.
- Owens BD, Stickles BJ, Busconi BD. Radiofrequency energy: applications and basic science. Am J Orthop. 2003;32(3):117–120.