J Clin Aesthet Dermatol. 2026;19(6):52–67.
by Scott Stratman, MD, MPH, and Helen He, MD
Drs. Stratman and He are with the Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
BACKGROUND: Atrophic scars have a significant psychosocial and functional impact on quality of life. Chemical reconstruction of skin scars (CROSS) using trichloroacetic acid (TCA) has emerged as an effective procedure for targeted treatment of atrophic scars, yet application methods and efficacy vary across scar types and patient populations. OBJECTIVE: To evaluate the methodology, indications, efficacy, and safety profile of the TCA CROSS technique in atrophic scarring and to compare TCA CROSS outcomes to other therapeutic modalities and assesses its adjunctive use. METHODS: A PubMed literature search was performed for clinical studies evaluating TCA application in scar management; inclusion criteria focused on studies using the CROSS technique published after 2002. Two reviewers independently screened 133 results: 34 publications (20 clinical trials, 4 comparative/cohort studies, 4 case series, 2 case reports, and 4 expert opinions) met eligibility criteria. RESULTS: In total, 937 patients (predominantly female, aged 4–65 years, Fitzpatrick skin types I–V) were included. TCA CROSS was primarily used for ice pick and boxcar acne scars, but it was also used for varicella and leishmaniasis scars. Application techniques varied, with fine-gauge needles and paintbrushes enabling more precise delivery. Multiple sessions yielded greater improvement, and higher TCA concentrations increased the risk of complications. Patient satisfaction was generally high, with improvement rates of 50% to 80%. The most common adverse events were transient postinflammatory pigmentary changes. CONCLUSION: TCA CROSS is a safe, effective option for treating atrophic scars. Methodical application and multimodality approaches optimize patient outcomes; further research should address technique standardization and efficacy across diverse skin types. Keywords: Trichloroacetic acid, TCA, CROSS, atrophic, scar, cosmetic dermatology, adjunct therapy
Introduction
Atrophic scarring can be a sequela of multiple different dermatologic conditions, most commonly acne vulgaris, and can cause significant impacts on quality of life.1 The pathogenesis of atrophic scarring is driven by dysregulated wound healing, persistent inflammation, and aberrant fibroblast activity, leading to flawed collagen synthesis and tissue contraction.2 This pathogenic process results in dermal depressions from insufficient collagen deposition.2 Atrophic scars can be categorized based on their appearance through the Jacob et al3 classification system for atrophic acne scars. There are 3 types of atrophic acne scars: ice pick, rolling, and boxcar scars. Atrophic scars are associated with substantial psychosocial distress, diminished quality of life, and functional impairment, necessitating effective and individualized treatment strategies.4,5
The therapeutic landscape for atrophic scarring has evolved considerably, with evidence supporting the efficacy of ablative and nonablative fractional laser, microneedling, platelet-rich plasma (PRP), dermal fillers, subcision, and chemical peels, either as monotherapies or in combination.5 Among these modalities, the trichloroacetic acid (TCA) chemical reconstruction of skin scars (CROSS) technique has emerged as an effective treatment option for ice pick and boxcar scars. TCA CROSS causes focal chemical injury to the dermal tissue at the base and walls of scars, which stimulates new collagen synthesis and dermal remodeling through fibroblast activation.6 This subsequently results in gradual elevation of the scar base, reducing scar depth with improvement in texture and appearance over multiple sessions.
In recent years, the TCA CROSS technique has been used to treat nonacne atrophic scarring such as varicella and leishmaniasis atrophic scars.6–10 Furthermore, TCA CROSS can be combined with other treatment modalities for patients who often have a spectrum of different atrophic scars. Since the comprehensive review by Chung et al,11 additional studies have provided new insights into this technique, such as optimal application instruments, comparative efficacy of different TCA concentrations, and outcomes in a larger population of Fitzpatrick skin types (FST). The objective of this review is to update the current literature about the methodology, indications, efficacy, and safety profile of TCA CROSS in atrophic scars. Moreover, this review aims to compare the outcomes of TCA CROSS to other treatment modalities or as an adjunct for atrophic scarring.
Methods
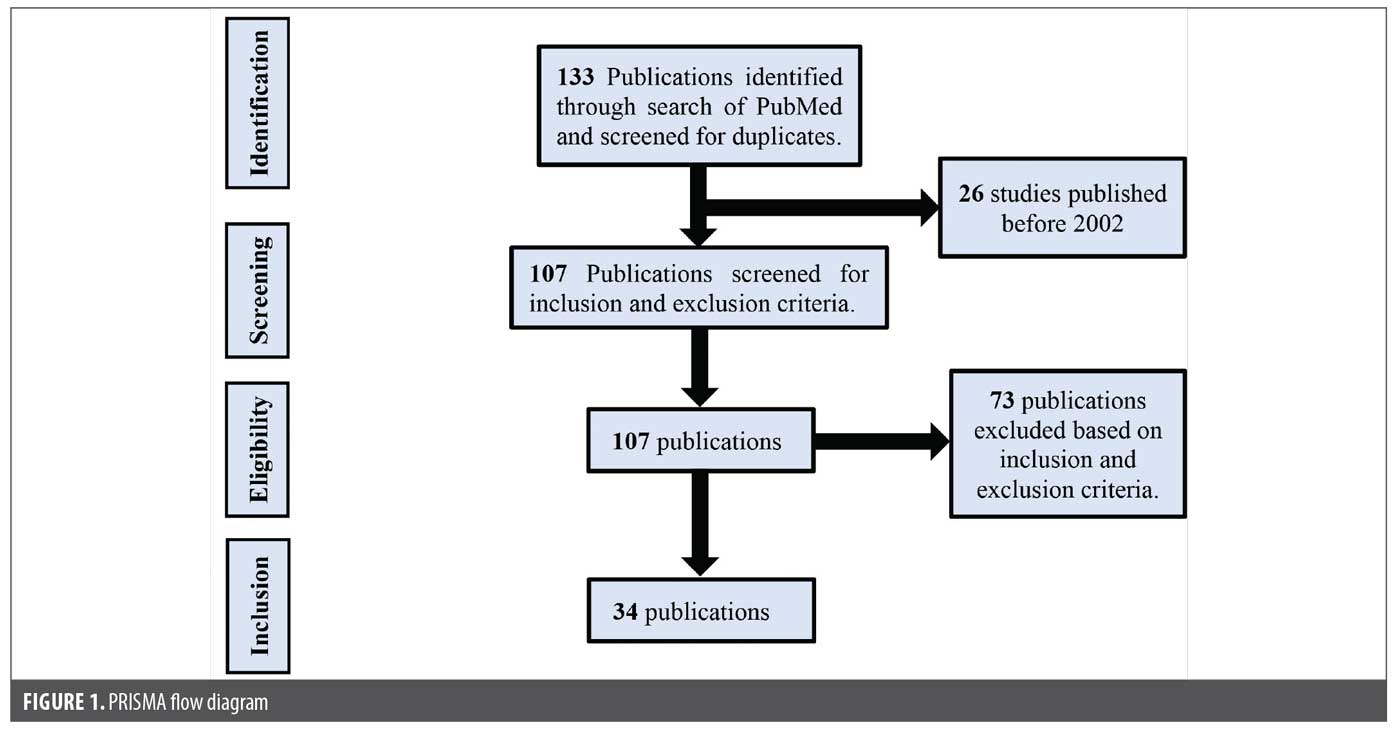
A systematic literature search was conducted using the PubMed database to identify studies evaluating the use of TCA in the management of scars, with a particular focus on acne scars. The search strategy employed the following terms: (“scar” OR “acne”) AND “trichloroacetic acid.” The search retrieved 133 results that were subsequently restricted to 107 publications by limiting the time frame to studies published after 2002, the year in which the CROSS technique was first described. Two independent reviewers (S.S. and H.H.) screened each article for eligibility criteria. Publications were excluded if they were animal studies or review articles, not written in English, lacked available full text, or represented duplication publications or if they did not utilize the CROSS methodology. Procedural pearls and opinion pieces from experts were included. After reviwing for exclusion criteria, 34 publications (20 clinical trials, 4 comparative/cohort studies, 4 case series, 2 case reports, 4 expert opinions) were included in this review (Figure 1).
Results
Patient demographics. A total of 937 patients were included in the selected 34 publications (Table 1), and most were female. The age range for patients was 4 to 65 years. The most common FST range was IV to V. Nine publications included FST II,8,9,12–18 and 2 publications included FST I.15,19
Clinical indications. The types of scars evaluated in these publications were predominantly atrophic acne scars (ice pick, rolling, and boxcar). Fourteen publications specifically mentioned evaluating ice pick acne scars.13,14,16,19–29 In addition to atrophic acne scars, the CROSS method was employed in varicella6,7,9 and leishmaniasis scars8,10 as well as enlarged pores.30
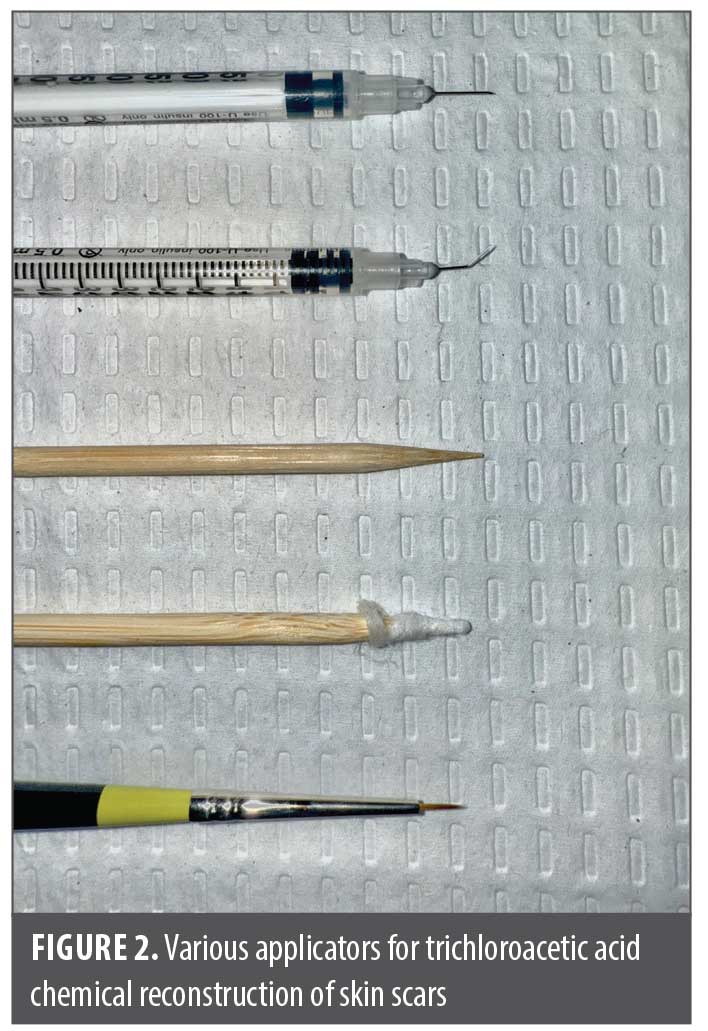
Techniques. Types of applicators. There were several types of applicators used (Figure 2). Sharpened wooden applicators, toothpicks, and cotton-wrapped applicators were commonly used. However, this reportedly led to longer treatment times as the wooden applicator or toothpick required repeated dipping into TCA. Whang et al30 proposed the use of either a 30-, 31-, or 33-gauge needle and syringe for acne scars or enlarged pores, eliminating the need to repeatedly dip back into TCA solution. Cho et al31 suggested bending the needle on a syringe, which increases the resistance of flow and, therefore, slows the flow rate of TCA from the needle, allowing for more precise application. More recently, Rullan29 commented on the use of a cosmetic paint brush for TCA CROSS, a technique that was also implemented by Sun and Lim.19 Use of a cosmetic paintbrush allows for painting TCA on the raised borders of boxcar and polymorphic scars, which would not normally be possible with a toothpick or wooden applicator. Currently, there are no studies comparing these different applicators, and selection of a preferred applicator is provider dependent.
Concentration of TCA. There were varying concentrations of TCA used, ranging from 50% to 100%. The most used TCA concentration was 100%. Several studies investigated the differences in TCA CROSS concentration and patient outcomes.16,18,32 While there was no significant difference in efficacy between lower and higher concentrations of TCA, there were more complications in higher TCA concentrations.18,32
Method of application. The CROSS technique involves pinpoint application of a high concentration acid to an atrophic scar using an applicator. The clinical endpoint is white frosting of each scar, which usually occurs within seconds of application (Figure 3 and Figure 4). This results in a controlled injury, prompting the skin to heal and rebuild through neocollagenesis.


Multiple methods of application have been previously described (Figure 2). The proceduralist may stretch the skin surrounding the atrophic scar and use an applicator to touch the base of the scar.6–10,13–15,18,20–23,25,32–39 A needle attached to a syringe can be used to form microdroplets of acid, which subsequently fills the atrophic scar.16,17,24,26,27,30,31,40 Controlled application of TCA in atrophic scars is recommended, as spillage outside of the scar can result in worsening of the scar or other adverse events. Kang et al40 performed the CROSS technique in a different way by using a 29-gauge needle with a syringe to prick atrophic scars, facilitating deeper penetration of 100% TCA.
Precare instructions. Various topical agents were reportedly used either together or separately in the weeks leading up to TCA application. Sunscreen, both SPF 30 or SPF 50+, was typically combined with hydroquinone (HQ) or a topical retinoid (tretinoin or adapalene). Some publications reported using HQ and/or topical retinoids at least 2 to 4 weeks prior.12,14–16,22,23,35
On the day of the procedure, several authors reported using topical lidocaine for anesthesia prior to procedure. Before the procedure, acetone or alcohol were used frequently to degrease the patient’s skin. There were no reports of patients needing oral prophylaxis with antibiotics or antivirals prior to CROSS procedure.
Postcare instructions. Most publications reported using general wound care through petrolatum-based ointments and moisturizers or emollients. Topical antibiotics such as mupirocin, polysporin, or other antibiotic creams were used for a few days after TCA CROSS until focal crust formation. As with the precare instructions, some patients were advised to use sunscreen for photoprotection or HQ and/or retinoids to mitigate postinflammatory hyperpigmentation (PIH).
Other adjunctive medications for mitigating PIH included topical desonide and 20% azelaic acid daily. Sun and Lim19 were the only ones to report using oral doxycycline and oral valacyclovir. They reported using doxycycline 50 mg daily for 7 days postprocedure and valacyclovir 500 mg twice daily for 5 days, but only if the patient reported a history of herpes simplex virus infection.
Number and frequency of treatments. Across the included studies, 4 treatment sessions was the most common number of treatments for most studies; 3 treatment sessions were also typically seen. The number of treatments increased based on the severity and chronicity of the target scar type. For instance, 5 treatments were reported by Nilforoushzadeh et al8 when treating leishmaniasis scars with 50% TCA. Barikbin et al9 reported using 6 treatments for atrophic facial varicella scars with 70% TCA.
Regarding frequency of treatment, a 2- to 4-week interval between treatments was most common. However, some studies personalized their treatment intervals based on the healing and PIH risk of their patients.
Adjunct and compared therapies. Laser therapy. Fractional laser techniques were either used as adjunct therapies or as comparators to TCA CROSS in several studies.8,10,14,16,21,40 Kim et al21 and Kang et al40 both employed a 1,550-nm Erbium glass (Er:Glass) fractional photothermolysis device for management of atrophic acne scars. Kim et al21 conducted a split-face randomized trial directly comparing Er:Glass fractional laser with TCA CROSS, finding no statistically significant difference in mean scar improvement between the 2 modalities. However, both physician and patient assessments indicated significantly greater improvement for rolling scars with the fractional laser than with TCA CROSS, whereas no significant difference was observed for ice pick scars.
In contrast, Kang et al40 implemented the 1,550 nanometer Er:Glass fractional laser as an adjunct to dot peeling and subcision, reporting marked reductions in scar severity scores. The authors concluded that a multimodal therapeutic strategy for scar treatment is needed to address solitary atrophic acne scars, improve skin texture, and treat broad depressed boxcar or rolling scars. Bahl et al16 also used nonablative fractional laser therapy in combination with TCA CROSS to treat ice pick and boxcar acne scars. After 3 to 6 sessions, all patients achieved moderate-to-significant improvement in their scarring. All patients were either satisfied (76%) or very satisfied (24%) after their last treatment.
Ahmed et al14 compared carbon dioxide (CO2) ablative therapy to 100% TCA CROSS in ice pick acne scars. Both groups (CO2 and TCA CROSS) had 4 treatments every 3 weeks with 3 months of follow-up. The authors reported a significant reduction in the severity of scar appearance in the CO2 group compared to the TCA group. Patients were also significantly more satisfied in the CO2 group with no major complications. Nilforoushzadeh et al8 also compared 1-time CO2 ablative therapy against focal 50% TCA peeling for leishmaniasis scars. They reported significant improvement post-treatment in both groups, but there was no significant difference between the 2 methods. While there were more cases of hyperpigmentation in the TCA group, there was more resistant erythema in the CO2 group. Iraji et al10 used CO2 ablative therapy as an adjunct therapy to focal peeling with 50% TCA for leishmaniasis scars. They compared TCA and CO2 ablative therapy to laser therapy alone and found that none of the cases in the laser monotherapy group responded completely. All leishmaniasis lesions in the TCA and CO2 laser group showed either good or excellent response.10
Subcision. Subcision is a minor surgical procedure in which a needle, cannula, or specialized blade is inserted under the surface of the skin to directly disrupt fibrous septae that anchor the scar to deeper structures, allowing the overlying skin to elevate. Kang et al40 implemented this technique alongside dot peeling and laser with significant improvement in acne scars. Kaur and Kalsy35 also used subcision as an adjunct to TCA dot peeling but did not use laser in their sample. Based on their assessments, 6 patients had an excellent response, 3 had a good response, and 1 had a fair response. Transient PIH occurred in 3 patients, while there were no “significant complications” reported by Kang et al.40
Ramadan et al34 compared subcision against 100% TCA for rolling acne scars and found a statistically significant improvement in the average size of scars for both TCA and subcision groups. However, there was a more significant reduction on the subcision side, suggesting that other modalities may be more suitable for rolling scars (eg, subcision or ablative laser) than TCA CROSS. Moreover, there was more pigmentary alteration from baseline on the TCA side compared to the subcision side.
Platelet-rich plasma. Platelet-rich plasma (PRP) is a blood product with a high concentration of platelets and growth factors, such as platelet-derived growth factor, transforming growth factor beta, and epidermal growth factor, that are critical for tissue regeneration and wound healing. Intradermal injection of PRP into atrophic acne scars can promote collagen synthesis and remodel the extracellular matrix.41 Mumtaz et al38 compared intradermal PRP against 50% TCA in patients with atrophic acne scarring. After 12 and 24 weeks of therapy, they reported a significant difference in scar scores for both intradermal PRP and TCA; however, intradermal PRP was significantly superior with a greater reduction in scar scores when compared to 50% TCA.
Nofal at el36 compared intradermal PRP to 100% TCA and microneedling with topical PRP. Each group had 3 treatment sessions with 2-week intervals. By the end of the study period, each group demonstrated significant improvement in scar severity.36 There was also no significant difference in the degree of improvement between groups. Kamel et al25 used intradermal PRP but as an adjunct therapy to 50% TCA CROSS along with subcision. The authors used a global scarring grading system and compared subcision with PRP to subcision with PRP and TCA CROSS. Both groups demonstrated significant improvement in their scar severity, and patients’ satisfaction was reported as excellent by 60% of patients and good by 40%.25 There was no statistically significant difference between the 2 treated sides. The authors reported that while the CROSS technique is beneficial for ice pick acne scars, combing TCA CROSS with PRP and subcision may provide added improvement to skin texture and/or other scars.
Microneedling. Percutaneous collagen induction (PCI), or microneedling, is a minimally invasive procedure that uses fine needles to create controlled micro-injuries in the skin. These controlled injuries stimulate the wound healing cascade, leading to increased production of collagen and elastin and remodeling of the extracellular matrix. Leheta et al12 compared PCI against TCA CROSS in 30 participants with atrophic acne scars. All the participants had an objective improvement in their acne scars, and the authors reported statistically significant improvement when using CROSS technique for ice pick scars and PCI for rolling scars. There was no statistically significant difference between either group regarding overall scar severity improvement. However, post-treatment erythema and overall downtime was longer in participants who received TCA than those who received PCI.
Acid peels. While the CROSS technique has been extensively studied using TCA, it has also been studied in other chemical agents such as phenol.15 Phenol is used for deep chemical peels and penetrates into the mid-reticular dermis. It is used to treat deep wrinkles and scars but has a higher risk of complications, most notably cardiac arrhythmias. Dalpizzol et al15 used phenol with the CROSS technique and compared this to 90% TCA. Post-treatment assessment scores were significantly lower compared to pretreatment assessment among physicians and patients. While there was no significant difference between TCA and phenol sides, treatment discomfort was significantly higher with phenol, while complications such as hypochromia and scar enlargement were only reported on the TCA side.15
Glycolic acid is another chemical agent used for superficial peels, and its effects are limited to the epidermis and superficial papillary dermis. Glycolic acid peels are effective in improving skin texture, hyperpigmentation, mild photodamage, and acne, but they are less effective for deep wrinkles or scars, although improvement with 70% glycolic acid peel has been reported for acne scars.42 Roy et al39 investigated 50% glycolic acid peel against 65% TCA CROSS for atrophic acne scars. Patients who received TCA CROSS had statistically significant improvement in visual results than those who received glycolic acid peel. However, adverse events were more prevalent in the TCA CROSS group compared to the glycolic acid group.
Timolol. Timolol is a beta-adrenergic receptor blocker that has been shown to improve and accelerate healing.43 Ghassemi et al28 used topical timolol as an adjunct therapy to TCA CROSS to reduce scar complications and accelerate the wound healing process. In addition to timolol, they also performed normal saline injections as an adjunct therapy, which has been shown to stimulate fibroblasts, collagen production, and rearrangement of the extracellular matrix.44 This results in accelerated healing of atrophic scars caused by acne. Forty-five participants with atrophic acne scars were randomly divided into 3 groups of 15 people. The new treatment was performed on 1 side of their face, and the other side was considered the control (TCA alone). Group 1 received TCA and normal saline, Group 2 received TCA and timolol, and Group 3 received TCA, normal saline, and timolol.
Through intragroup comparisons and evaluation of the efficacy of the new treatment, there was no significant effect on the number of scars in the participants when compared to the control group. However, patients who had received timolol (TCA and timolol; or TCA, normal saline, and timolol) experienced a significantly shorter period of postprocedure hyperpigmentation compared to patients who received saline and TCA. The results of the study showed that PIH after TCA CROSS may be significantly reduced if paired with topical timolol and/or saline.28
Clinical efficacy. Acne scars. Variable methods were used for physician assessment of scar improvement, with a quantile grading scale being the most common (Table 2). In studies using the quantile grading scale, 60% to 100% of patients experienced a >25% to 30% improvement in their atrophic acne scarring with participants in Nofal et al36 experiencing the least amount of improvement.7,12,14,19,22,23,33,35,37 For the other 9 studies, 66% to 100% of patients experienced a >50% improvement in their atrophic acne scarring. Yug et al20 and Fabbrocini et al6 did not use a specific assessment scale but did report an improvement in appearance and depth of scars. Horovitz et al17 measured scar volume deficit with a validated high-resolution 3-dimensional imaging system and found a 26.3% decrease in the volume of the scars after just 1 treatment.
The Échelle d’Évaluation Clinique des Cicatrices d’Acne (ECCA) grading scale associates each kind of acne scar with a quantitative score and a weighting factor.45 Dalpizzol et al15 used this grading scale to assess their participants’ atrophic acne scar improvement and reported significant improvement from pre- (130.7±73.7) and post-treatment (91.0±72.0) with TCA CROSS. Other studies used a global acne grading system, the Goodman-Baron scale, to determine acne scar improvement.18,25,38,39 The Goodman-Baron scale evaluates the degree of scarring after acne has resolved, with higher numbers for numerous lesions and severe atrophic or hypertrophic scars.46 Each author group that used this scale demonstrated a significant improvement in atrophic acne scarring for their participants by the end of the treatment protocol.25,38,39
Patient satisfaction with TCA CROSS for acne scars was rated generally high across multiple studies and clinical trials. Studies typically used a quantile scale to assess patient satisfaction, and most patients reported subjective improvement in their appearance. 9,12,14,16,25,33,34,36,37,39 Satisfaction rates commonly ranged from moderate to high, usually 50% to 80% improvement. Patient-reported outcomes consistently reflected favorable perceptions about TCA CROSS efficacy, especially when treatment was repeated for several sessions and tailored to scar type and skin phototype.
Kim et al21 and Leheta et al12 were the only groups to stratify improvement based on scar type. Kim et al21 concluded that 1,550-nm fractional laser had significantly higher improvement rates of rolling scars compared to TCA CROSS. However, there was no statistically significant difference in ice pick scar improvement when compared to this laser therapy and TCA CROSS.21 For Leheta et al,12 their physicians reported TCA CROSS performed better than PCI for ice pick scars but that PCI performed better than TCA CROSS for rolling scars. However, there was no statistically significant difference between the groups (TCA CROSS vs PCI) regarding overall scar severity improvement. Based on the results of our comprehensive review, TCA CROSS appears more suitable for ice pick scars rather than rolling scars, but this conclusion is limited by the few publications that stratified improvement based on scar type. Generally, acne scarring improves as the total number of treatment sessions increases.
While Lee at al33 suggested that higher TCA concentrations yield a higher therapeutic effect, other authors found no significant differences with TCA concentrations; instead, higher TCA concentrations come with more risk of complications, such as erythema, PIH, or postinflammatory hypopigmentation (PIHO). While the frequency between treatment remains ambiguous, the authors suggest that TCA be applied every 4 to 6 weeks to mitigate possible complications. Furthermore, we suggest an extension to 6 to 9 weeks for higher TCA concentrations (≥80%) or in patients with darker FSTs (IV–VI).
Varicella scars. Three publications investigated the use of TCA CROSS in atrophic varicella scars through clinical trials.6,7,9 Barikbin et al9 used 70% TCA, and 83% of patients had >25% improvement in their varicella scars. Agarwal et al,7 however, used 100% TCA, and 100% of patients had >25% improvement. Although their sample size was small (n=5), Fabbrocini et al6 reported improvement in scar appearance and depth with 50% TCA.
Leishmaniasis scars. Through a 2-arm randomized clinical trial, Nilforoushzadeh et al8 used 50% TCA CROSS to treat atrophic leishmaniasis scars. They reported that 57% of their participants experienced >20% improvement in their atrophic leishmaniasis scars. These results were also statistically insignificant when compared to 1-time carbon dioxide (CO2) ablative laser therapy. Iraji et al10 also investigated TCA CROSS in the treatment of leishmaniasis scars but used CO2 ablative laser therapy as an adjunct in a small case series. They found that all lesions in the CO2 and TCA group showed good or excellent response.10
Complications. TCA CROSS is generally a well-tolerated procedure with few serious adverse effects. Of the publications that were included in our study, patients with FST I through VI were all evaluated. PIH was the most frequent adverse event, with incidence rates varying from mild, transient cases (weeks) to more prolonged episodes (months). Several studies reported rates of PIH ranging from 6.7% to over 60%.14 The current literature suggests that PIH from TCA CROSS is a transient adverse event and can also be treated with hydroquinone and tretinoin to expedite resolution. Every patient, regardless of FST, should be counseled on this possible adverse event, and proceduralists should be informed about possible treatments to help expedite PIH resolution.
Postinflammatory erythema (PIE) and PIHO were the more common adverse events after PIH. While most cases of PIE were transient, some studies reported PIE that was more persistent.15,34 PIHO was less common than PIE, and only transient cases that were documented.9,22,23,34 Mild crusting was nearly universal after procedure, but it generally resolves without significant sequelae. Burning sensation and pain were infrequently reported; some authors used topical lidocaine before the procedure.16,25 Finally, infection was uncommon and reported in only 1 study.14
One significant adverse event that was documented from TCA CROSS was scar enlargement or worsening atrophy.13,15,27,37 Three of these 4 publications used a sharpened wooden applicator or toothpick.13,15,37 This could have resulted in poorly controlled application of TCA, with spillage onto perilesional skin and subsequent worsened atrophy. Veenstra et al27 used an electronic micropipette device to perform TCA CROSS; however, they presumed this resulted in less precise application of TCA, resulting in worsening scar atrophy for 1 of their patients. Based on the current literature, proceduralists recommend using a fine-gauge needle or a fine paintbrush for controlled application of TCA.15,18,19,26,28
Not every study included in our review stratified complication by FST. Therefore, the proceduralist performing TCA CROSS should counsel their patients on each of the previously mentioned complications regardless of the patient’s FST. Future directions for research should focus on assessing complication rates based on patient FSTs.
Discussion
TCA CROSS is well-tolerated in patients with atrophic acne scars with minimal complications. Specifically, TCA CROSS is best used for ice pick scars, followed by boxcar scars, then rolling scars. While TCA CROSS demonstrated improvement in patients with atrophic scars from varicella and leishmaniasis, additional research through clinical trials is warranted to determine its efficacy in this population. Regarding FST, types I through V were the most studied, and this technique appears relatively safe in this patient population. Only 1 participant with FST VI was included in our review, and they subsequently developed PIH. Additional research is needed about the efficacy and safety profile of TCA CROSS in patients with FST VI.
Multiple treatment sessions increase the overall success rate of TCA CROSS. While higher TCA concentrations can also increase success rate, the risk of complications (eg, PIH, PIE, and PIHO) is higher. Regarding method of application, fine-gauge needles with syringes offer more precise control compared to toothpicks or other wooden applicators. A fine paintbrush can also be used to apply TCA at the base and sides of an atrophic scar. Complications such as PIH, PIE, and PIHO are generally transient and topical agents such as hydroquinone and tretinoin can be used to prevent and/or hasten resolution of these adverse effects.
Conclusion
While TCA CROSS is a useful tool, it is important to recognize that no one treatment may be most suitable for a patient. Instead, the authors recommend a multimodality approach to address each patient’s unique scar concerns and provide synergistic therapeutic effects on different scar types, which commonly co-occur in the same individual. Therefore, when approaching scar treatment, combination therapy should always be considered. The published literature continues to have several limitations, such as small sample sizes, inconsistent follow-up between patients, differing TCA concentrations and frequency of application, and variations in assessment scores. Future research in randomized controlled trials should focus on defining the optimal application frequency, concentration, and number of sessions. These studies should also aim to include participants with a broad spectrum of FST and stratify analysis by patient demographics, including skin type and scar classification.
Ethics statement
Consent for the publication of all patient photographs and medical information was provided by the authors at the time of article submission to the journal, stating that all patients gave consent for their photographs and medical information to be published in print and online with the understanding that this information may be publicly available.
Author contributions
Both authors contributed substantially to the conception, design, acquisition of data, analysis and interpretation of the data included in this manuscript. They were both involving in draft production and revision of intellectual content.
References
- Tan J, Beissert S, Cook-Bolden F, et al. Impact of facial atrophic acne scars on quality of life: a multi-country population-based survey. Am J Clin Dermatol. 2022;23(1):115–123.
- Kohlhauser M, Mayrhofer M, Kamolz LP, Smolle C. An update on molecular mechanisms of scarring-a narrative review. Int J Mol Sci. 2024;25(21):11578.
- Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45(1):109–117.
- Basson R, Bayat A. Skin scarring: latest update on objective assessment and optimal management. Front Med (Lausanne). 2022;9:942756.
- Chilicka K, Rusztowicz M, Szygula R, Nowicka D. Methods for the improvement of acne scars used in dermatology and cosmetology: a review. J Clin Med. 2022;11(10):2744.
- Fabbrocini G, Cacciapuoti S, Fardella N, Pastore F, Monfrecola G. CROSS technique: chemical reconstruction of skin scars method. Dermatol Ther. 2008;21 Suppl 3:S29–S32.
- Agarwal N, Mittal A, Kuldeep C, Gupta LK, Khare AK, Mehta S. Chemical reconstruction of skin scars therapy using 100% trichloroacetic acid in the treatment of atrophic facial post varicella scars: a pilot study. J Cutan Aesthet Surg. 2013;6(3):144–147.
- Nilforoushzadeh MA, Jaffary F, Ansari N, Moradi S, Siadat AH. The comparison between trichloroacetic acid 50% and CO2 laser in the treatment of cutaneous leishmaniasis scar. Indian J Dermatol. 2011;56(2):171–173.
- Barikbin B, Saadat N, Akbari Z, Yousefi M, Toossi P. Focal high-concentration trichloroacetic acid peeling for treatment of atrophic facial chickenpox scar: an open-label study. Dermatol Surg. 2012;38(10):1662–1667.
- Iraji F, Asilian A, Heidari A, Shariat S, Jazi SB, Siadat AH. Combination of continuous wave CO2 laser and topical application of trichloroacetic acid 50% vs CO2 laser alone the treatment of cutaneous leishmaniasis (a case series of 6 patients). J Cosmet Dermatol. 2020;19(6):1367–1370.
- Chung HJ, Al Janahi S, Cho SB, Chang YC. Chemical reconstruction of skin scars (CROSS) method for atrophic scars: a comprehensive review. J Cosmet Dermatol. 2021;20(1):18–27.
- Leheta T, El Tawdy A, Abdel Hay R, Farid S. Percutaneous collagen induction versus full-concentration trichloroacetic acid in the treatment of atrophic acne scars. Dermatol Surg. 2011;37(2):207–216.
- Weber MB, Machado RB, Hoefel IR, Manzoni AP, Da Silva Bastos Geler A. Complication of CROSS-technique on boxcar acne scars: atrophy. Dermatol Surg. 2011;37(1):93–95.
- Ahmed R, Mohammed G, Ismail N, Elakhras A. Randomized clinical trial of CO2 LASER pinpoint irradiation technique versus chemical reconstruction of skin scars (CROSS) in treating ice pick acne scars. J Cosmet Laser Ther. 2014;16(1):8–13.
- Dalpizzol M, Weber MB, Mattiazzi APF, Manzoni APD. Comparative study of the use of trichloroacetic acid and phenolic acid in the treatment of atrophic-type acne scars. Dermatol Surg. 2016;42(3):377–383.
- Bahl A, O’Connor K, Chung HJ. Treatment of atrophic acne scars with combination therapy of chemical reconstruction of skin scars method and fractionated nonablative laser: a retrospective analysis. J Cosmet Dermatol. 2020;19(10):2591–2595.
- Horovitz T, Salameh F, Shehadeh W, Koren A, Artzi O. Painting CROSS TCA technique: modification of the CROSS method for the treatment of atrophic acne scars-case series. J Cosmet Dermatol. 2022;21(1):327–330.
- Soysal MC, Akçalı C. Comparison of 70% and 100% concentration of trichloroacetic acid peeling efficacy with chemical reconstruction of skin scars technique in atrophic acne scar treatment. Arch Dermatol Res. 2025;317(1):547.
- Sun C, Lim D. Trichloroacetic acid paint for boxcar and polymorphic acne scars. Dermatol Surg. 2022;48(2):214–218.
- Yug A, Lane JE, Howard MS, Kent DE. Histologic study of depressed acne scars treated with serial high-concentration (95%) trichloroacetic acid. Dermatol Surg. 2006;32(8):985–990.
- Kim HJ, Kim TG, Kwon YS, Park JM, Lee JH. Comparison of a 1,550 nm Erbium: glass fractional laser and a chemical reconstruction of skin scars (CROSS) method in the treatment of acne scars: a simultaneous split-face trial. Lasers Surg Med. 2009;41(8):545–549.
- Bhardwaj D, Khunger N. An assessment of the efficacy and safety of CROSS technique with 100% TCA in the management of ice pick acne scars. J Cutan Aesthet Surg. 2010;3(2):93–96.
- Khunger N, Bhardwaj D, Khunger M. Evaluation of CROSS technique with 100% TCA in the management of ice pick acne scars in darker skin types. J Cosmet Dermatol. 2011;10(1):51–57.
- Vishwanath T, Barve A, Farande P, Ghate S, Shinde G, Nagpal A. Use of blunted needle of insulin syringe as a simple method for precise delivery of drug during chemical reconstruction of skin scars (CROSS). J Am Acad Dermatol. 2020;83(3):e177–e178.
- Kamel MM, Hegazy RA, Hegazy AA, Fotoh OMAE, Amer MA. Combined subcision, autologous platelet-rich plasma, and CROSS technique in the treatment of atrophic acne scars: prospective split face study. Clin Dermatol. 2021;39(6):1018–1024.
- Mitra D, Singh GK, Singh T, Mitra B. Use of 27-gauge tuberculin syringe for trichloroacetic acid chemical reconstruction of skin scars (TCA-CROSS). J Cutan Aesthet Surg. 2021;14(3):357–358.
- Veenstra JJ, Fakhoury JW, Ozog D. Worsening of acne scars from trichloroacetic acid CROSS delivered via micropipette: a case report. J Clin Aesthet Dermatol. 2021;14(4):41–42.
- Ghassemi M, Shahverdi MH, Behrangi E, Hosseini-Baharanchi FS, Goodarzi A. Efficacy and safety of topical timolol 0.5% plus saline 0.9% versus each one alone in acne scar trichloroacetic acid-CROSS therapy: a blinded randomized controlled trial. Dermatol Ther. 2022;35(4):e15341.
- Rullan P. Commentary on trichloroacetic acid paint. Dermatol Surg. 2022;48(2):219.
- Whang SW, Lee KH, Lee JB, Chung KY. Chemical reconstruction of skin scars (CROSS) method using a syringe technique. Dermatol Surg. 2007;33(12):1539–1540.
- Cho SB, Lee SJ, Kang JM, Kim YK, Kim DH. Chemical reconstruction of skin scars method using a syringe bent-needle technique. Dermatol Surg. 2009;35(7):1134–1135.
- Dac Thuy LN, Thuy Trang VT, Tran NN, Phuong Thao DT. Comparing the use of 80% trichloroacetic acid and 50% trichloroacetic acid for the treatment of ice pick acne scars. Dermatol Surg. 2024;50(9):847–850.
- Lee JB, Chung WG, Kwahck H, Lee KH. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatol Surg. 2002;28(11):1017–1021.
- Ramadan SAE, El-Komy MHM, Bassiouny DA, El-Tobshy SA. Subcision versus 100% trichloroacetic acid in the treatment of rolling acne scars. Dermatol Surg. 2011;37(5):626–633.
- Kaur J, Kalsy J. Subcision plus 50% trichloroacetic acid chemical reconstruction of skin scars in the management of atrophic acne scars: a cost-effective therapy. Indian Dermatol Online J. 2014;5(1):95–97.
- Nofal E, Helmy A, Nofal A, Alakad R, Nasr M. Platelet-rich plasma versus CROSS technique with 100% trichloroacetic acid versus combined skin needling and platelet rich plasma in the treatment of atrophic acne scars: a comparative study. Dermatol Surg. 2014;40(8):864–873.
- Agarwal N, Gupta LK, Khare AK, Kuldeep CM, Mittal A. Therapeutic response of 70% trichloroacetic acid CROSS in atrophic acne scars. Dermatol Surg. 2015;41(5):597–604.
- Mumtaz M, Hassan T, Shahzad MK, Hanif N, Anwar S, Anjum R. Comparing the efficacy of intra-dermal platelet rich plasma (PRP) versus 50% trichloracetic acid (TCA) using cross technique for atrophic acne scars. J Coll Physicians Surg Pak. 2021;31(1):55–59.
- Roy G, Gayen T, Sen S, Rudra O. Study to compare the efficacy of 50% glycolic acid with 65% trichloroacetic acid in the treatment of atrophic acne scar by CROSS technique. J Cutan Aesthet Surg. 2024;17(3):198–204.
- Kang WH, Kim YJ, Pyo WS, Park SJ, Kim JH. Atrophic acne scar treatment using triple combination therapy: dot peeling, subcision and fractional laser. J Cosmet Laser Ther. 2009;11(4):212–215.
- Hausauer AK, Humphrey S. The physician’s guide to platelet-rich plasma in dermatologic surgery part II: clinical evidence. Dermatol Surg. 2020;46(4):447–456.
- Erbağci Z, Akcali C. Biweekly serial glycolic acid peels vs. long-term daily use of topical low-strength glycolic acid in the treatment of atrophic acne scars. Int J Dermatol. 2000;39(10):789–794.
- Goodarzi A, Mozafarpoor S, Dodangeh M, Seirafianpour F, Shahverdi MH. The role of topical timolol in wound healing and the treatment of vascular lesions: a narrative review. Dermatol Ther. 2021;34(2):e14847.
- Pravangsuk J, Udompataikul M, Cheyasak N, Kamanamool N. Comparison of normal saline injection with pneumatic injector to subcision for the treatment of atrophic acne scars. J Clin Aesthet Dermatol. 2021;14(5):50–55.
- Dreno B, Khammari A, Orain N, et al. ECCA grading scale: an original validated acne scar grading scale for clinical practice in dermatology. Dermatology. 2007;214(1):46–51.
- Goodman GJ, Baron JA. Postacne scarring: a qualitative global scarring grading system. Dermatol Surg. 2006;32(12):1458–1466.