J Clin Aesthet Dermatol. 2026;19(6):46–48.
by Fahad Siddiqui, DO; Ann Church, MD; and Rajiv Nathoo, MD
Dr. Siddiqui is with the Kansas City University GME Consortium/Advanced Dermatology and Cosmetic Surgery, Maitland, Florida. Dr. Church is with Dermpath Diagnostics, Pompano Beach, Florida. Dr. Nathoo is with Sun State Dermatology, Maitland, Florida.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
Confluent and reticulated papillomatosis (CARP) is a rare keratinization disorder typically presenting as hyperpigmented, scaly papules that coalesce into reticulated plaques on the trunk of adolescents and young adults. Hypopigmented variants have only rarely been reported and are frequently misdiagnosed as tinea versicolor, resulting in delayed diagnosis and unnecessary antifungal therapy. We describe 2 young adults with biopsy-confirmed hypopigmented CARP who initially received multiple courses of oral and topical antifungal agents with minimal to no benefit. Both patients demonstrated widespread hypopigmented, scaly, coalescing plaques. Following histopathologic confirmation, antifungal treatments were discontinued, and oral minocycline was initiated, leading to clinical improvement. These cases add to the limited literature describing hypopigmented CARP and underscore that the disease’s defining features are distribution and morphology rather than pigmentation. Recognition of this rarely reported variant is essential for timely diagnosis and initiation of appropriate treatment. Keywords: Confluent and reticulated papillomatosis, CARP, hypopigmentation, tinea versicolor, minocycline, keratinization disorder, skin of color
Introduction
Confluent and reticulated papillomatosis (CARP), first described by Gougerot and Carteaud in 1927, is an uncommon dermatosis characterized by scaly papules that coalesce into confluent plaques with peripheral reticulation, most often affecting the upper trunk and neck of adolescents and young adults.1–3 Its pathogenesis remains incompletely understood, with proposed mechanisms including disordered keratinization, colonization by Dietzia papillomatosis, metabolic associations such as diabetes and obesity, and overexpression of keratin 16.2 Familial clustering and concurrent cases with tinea versicolor also suggest a possible genetic or microbial component.4
Classically, CARP is described as hyperpigmented.1,2 However, the clinical spectrum is broader: reports document hypopigmented CARP in darker skin types,1 nonpigmented erythematous CARP in fair-skinned individuals,5 and coexistence with fungal elements that complicate diagnosis.4 These variants are frequently mistaken for tinea versicolor, eczema, or ichthyosis, leading to prolonged mismanagement with antifungals.1,4,5
While oral minocycline remains the mainstay of treatment, responses to other systemic antibiotics and topical keratinization-modulating therapies, including retinoids and vitamin D analogs, support a pathophysiologic basis in abnormal epidermal maturation.1–3,6 Recognition of unusual morphologic variants is essential for timely diagnosis and effective therapy. We present 2 cases of hypopigmented CARP, underscoring the diagnostic challenge in skin of color and the importance of including CARP in the differential diagnosis of persistent, scaly hypopigmented plaques.
Case 1
An 18-year-old female patient with a history of diabetes presented with an asymptomatic rash on her back and upper extremities. She denied pruritus, pain, or tenderness. She was not taking any medications, denied alcohol or drug use, and had no known allergies. On physical examination, annular scaly hypopigmented plaques were observed on the back, chest, and bilateral upper arms (Figure 1). Based on morphology, a clinical diagnosis of tinea versicolor was made. The patient was prescribed ketoconazole 2% shampoo to be used as a body wash 3 times weekly and fluconazole 300 mg weekly for 2 weeks.

At the 2-week follow-up, the patient did not see improvement. Examination showed persistent hypopigmentation with minimal clinical improvement. Antifungal therapy was continued for another 2 weeks. On subsequent follow-up, lesions remained active with increased body surface area. A geometric hypopigmented patch was also noted on the right posterior shoulder, prompting a 4-mm punch biopsy.
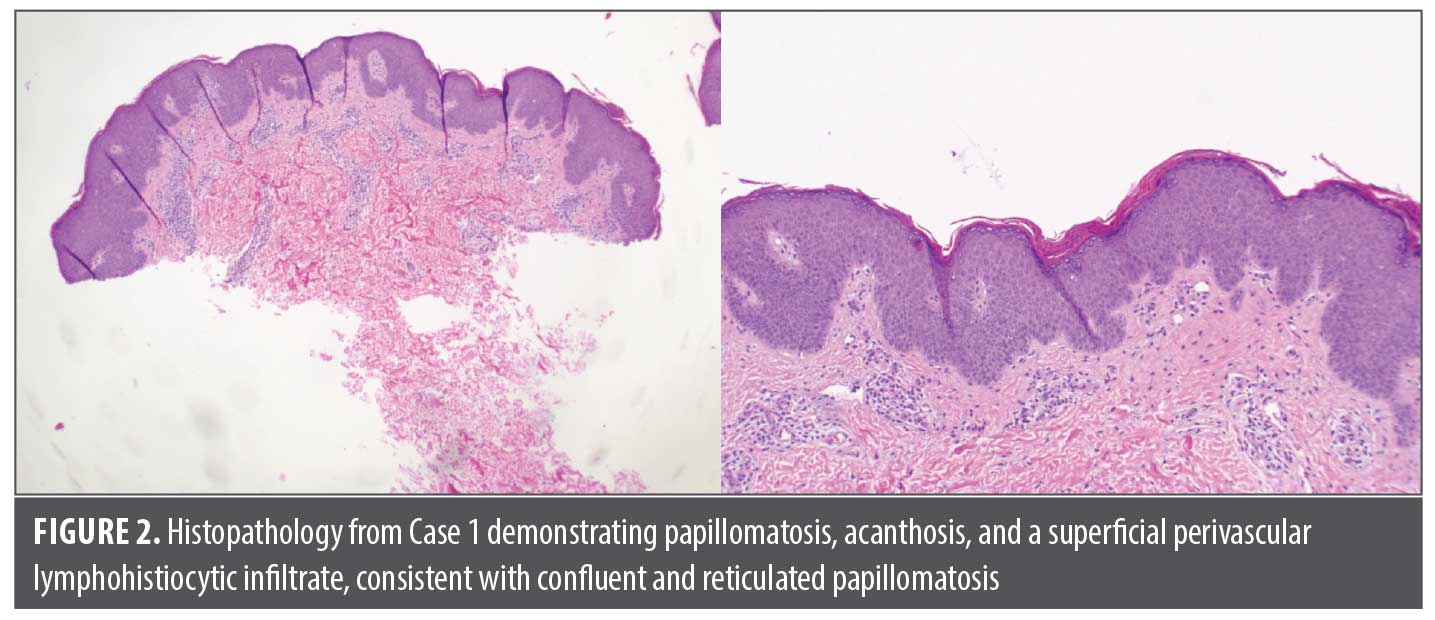
Histopathologic examination revealed papillomatosis, acanthosis, and a superficial perivascular lymphohistiocytic infiltrate, leading to a diagnosis of CARP (Figure 2). At this stage, the eruption had progressed with scaly hypopigmented macules coalescing into reticulated patches across the chest, abdomen, back, and upper extremities. Given the lack of response to antifungal therapy and the biopsy findings, antifungal therapy was discontinued, and the patient was started on oral minocycline 100 mg twice daily for 6 weeks.
Case 2
A 22-year-old male patient with no significant past medical history presented with a several-year history of a pruritic rash on the trunk. He denied pain or tenderness. On physical examination, annular scaly hypopigmented plaques were observed on the chest, abdomen, and back (Figure 3). Based on morphology, a clinical diagnosis of tinea versicolor was made. The patient was started on fluconazole 200 mg orally once weekly for 4 weeks in combination with ketoconazole 2% shampoo applied as a body wash 3 times weekly.

At the 4-week follow-up, the patient reported only minimal improvement. Examination revealed persistent hypopigmented scaly plaques on the trunk. The fluconazole dose was subsequently increased to 400 mg weekly for 4 weeks. Despite this escalation, the patient continued to experience no improvement and complained of worsening pruritus.
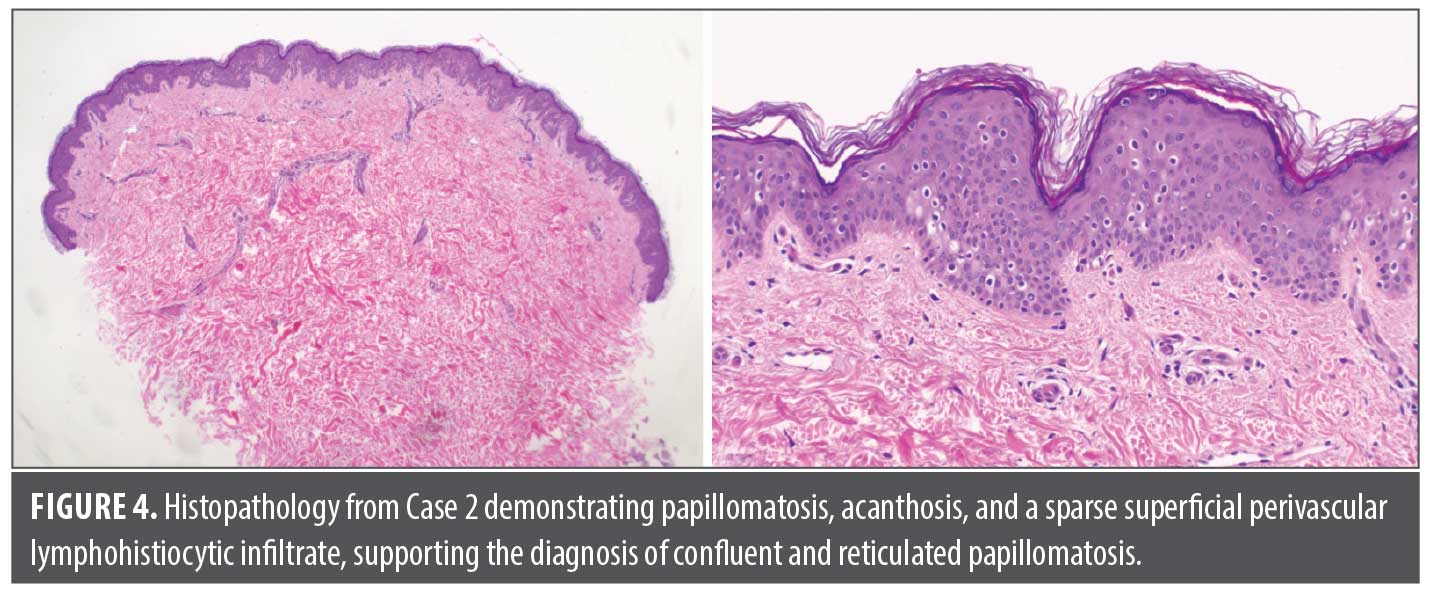
At the next visit, the eruption remained active, and hypopigmented nonscaly patches were noted on the right scapular back. Given the refractory nature of the eruption and the broadened differential diagnosis, a punch biopsy was performed. Histopathology showed papillomatosis, acanthosis, and a sparse perivascular lymphohistiocytic infiltrate, confirming a diagnosis of CARP (Figure 4). At this point, the eruption had progressed with hypopigmented scaly macules coalescing into reticulated patches across the chest, back, and upper extremities. Antifungal therapy was discontinued, and the patient was started on oral minocycline 100 mg twice daily.
At follow-up 3 weeks later, the patient reported improvement. Examination showed partial resolution of hypopigmented scaly plaques. Minocycline was continued to complete a 6-week course.
Discussion
These 2 cases expand upon the growing recognition that CARP can deviate significantly from its “classic” hyperpigmented presentation. Hypopigmented CARP, as in our patients, was documented in prior series of dark-skinned individuals, where decreased melanin synthesis with preserved melanocyte density was observed on histology.1 This suggested that pigmentary change is not intrinsic to CARP itself but may reflect variable melanogenic activity across skin types. Similarly, Treat et al5 described nonpigmented CARP manifesting as pink, scaly plaques without hyperpigmentation, further reinforcing that color should not be considered a defining criterion for diagnosis. Cases of hypopigmented and nonpigmented CARP, including both previously reported cases and the patients described here, are summarized in Table 1 with respect to age, sex, race/ethnicity, and treatment response.
The diagnostic challenge stems from clinical overlap with tinea versicolor. Both conditions produce scaly, reticulated plaques on the trunk, and hypopigmented variants are particularly difficult to distinguish in skin of color.1,4 Key differentiators include a lack of hyphae on a potassium hydroxide test or biopsy preparation and failure to respond to antifungal therapy.1,2,4 In our patients, extensive antifungal therapy did not produce improvement, prompting biopsy and eventual recognition of CARP.
Pathogenesis remains debated. Earlier associations with Malassezia raised the possibility of an inflammatory response to yeast,4 but inconsistent fungal isolation and responsiveness to tetracyclines point toward a keratinization disorder with possible microbial triggers.2 Familial clustering, as documented in siblings with both CARP and tinea versicolor, suggests a genetic predisposition that may influence host response.4 More recently, disordered keratinization has been supported by therapeutic successes with topical retinoids, vitamin D analogs, and combination regimens such as calcipotriene plus tretinoin.3 These interventions normalize keratinocyte differentiation and turnover, targeting the underlying epidermal dysregulation rather than microbial colonization.
Therapeutically, oral minocycline remains the most reliable agent, producing rapid clearance in most reported cases regardless of pigmentation.1,2,4,5 However, adverse effects, relapses, and patient preference for systemic-sparing options highlight the need for alternatives.3 Adjunctive or standalone topical regimens, particularly keratinization-directed therapies, have shown promise in recent case reports.3 In hypopigmented or nonpigmented CARP, where misdiagnosis is common, the therapeutic trial of an antibiotic can serve both diagnostic and curative functions.
Our cases add to the literature by confirming that CARP in skin of color may present exclusively as hypopigmented plaques, reinforcing that the disease’s defining features are distribution and morphology rather than pigmentary change. These findings underscore the need for clinicians to broaden diagnostic suspicion, especially when confronted with persistent hypopigmented eruptions unresponsive to antifungals.
Conclusion
CARP is a heterogeneous disorder of keratinization with morphologic variants that challenge traditional descriptions. Hypopigmented CARP in darker skin and nonpigmented CARP in lighter skin expand the clinical spectrum beyond its classic hyperpigmented form. When hypopigmented or erythematous, CARP can closely mimic tinea versicolor or other dermatoses, delaying diagnosis and treatment. Recognition of these variants, along with careful consideration of distribution, histology, and treatment response, is essential. Oral minocycline remains the most effective first-line therapy, but emerging topical regimens such as calcipotriene and tretinoin demonstrate promise. Our cases highlight the importance of considering CARP in the differential diagnosis of persistent hypopigmented plaques and add to the evolving recognition of color-independent variants of this rare dermatosis.
References
- Hudacek KD, Haque MS, Hochberg AL, Cusack CA, Chung CL. An unusual variant of confluent and reticulated papillomatosis masquerading as tinea versicolor. Arch Dermatol. 2012;148(4):505–508.
- Le C, Bedocs PM. Confluent and reticulated papillomatosis. In: StatPearls [Internet]. StatPearls Publishing; 2026–. Updated 7 Aug 2023. Accessed 2 Feb 2026. https://www.ncbi.nlm.nih.gov/books/NBK459130/
- Nathoo R, Siddiqui F. Successful treatment of confluent and reticulated papillomatosis with calcipotriene and tretinoin: a novel topical regimen. J Clin Aesthet Dermatol. 2025;18(9):55–57.
- Stein JA, Shin HT, Chang MW. Confluent and reticulated papillomatosis associated with tinea versicolor in three siblings. Pediatr Dermatol. 2005;22(4):331–333.
- Treat JR, Barak OG, James WD. Nonpigmenting confluent and reticulated papillomatosis. Pediatr Dermatol. 2006;23(5):497–499.
- Mufti A, Sachdeva M, Maliyar K, et al. Treatment outcomes in confluent and reticulated papillomatosis: a systematic review. J Am Acad Dermatol. 2021;84(3):825–829.