J Clin Aesthet Dermatol. 2026;19(6):22–26.
by Suneel Chilukuri, MD; Isabel Diaz, BA; Bianca GonzaleZ, BS; and Lia Arvanitidou, PhD
Dr. Chilukuri is with Refresh Dermatology, Houston, Texas. Ms. Diaz, Ms. Gonzalez, and Dr. Arvanitidou are with Colgate-Palmolive Company, Piscataway, New Jersey.
FUNDING: This study was sponsored by Colgate-Palmolive Company/CP Skin Health Group/PCA Skin.
DISCLOSURES: Dr. Chilukuri is a consultant and researcher for Colgate-Palmolive Company and PCA Skin. Ms. Diaz, Ms. Gonzalez, and Dr. Arvanitidou are employees of Colgate-Palmolive Company.
OBJECTIVE: To demonstrate the safety and enhanced cosmetic outcomes of the combination of microneedling with a pigment-correcting peel when treating hyperpigmented skin across diverse Fitzpatrick skin types. METHODS: A total of 31 patients (Fitzpatrick skin types I–V) with facial hyperpigmentation were enrolled in the study. Each participant received 2 different treatments on the face: 1 side was treated with a pigment-correcting peel combined with microneedling, while the other side received microneedling alone (3 sessions, 4 weeks apart). Assessments included Mexameter measurements, dermatologist grading, and standardized clinical imaging. Self-assessment questionnaires were completed by participants at different timepoints. RESULTS: The 31 participants completed the study; both microneedling alone and the combination treatment were well tolerated. The combined approach yielded significantly better results according to dermatologist efficacy assessment for clarity/brightness, evenness of skin tone (pigmentation and redness), overall appearance and texture (P<0.05), and patient perception, with 94% reporting a significant or noticeable improvement on skin discoloration/hyperpigmentation on the side treated with combination therapy and 90% reporting they prefer the results of the combination therapy vs microneedling alone (P<0.0001). LIMITATIONS: A primary limitation of this study was the restricted assessment window, which proved to be insufficient to achieve significant clinical improvement for parameters such as fine lines, wrinkles, and pore size. CONCLUSION: This research showed that combining a pigment-correcting peel with microneedling can be significantly more effective at improving overall skin appearance than microneedling alone. This combined therapy was safe, well tolerated, and preferred by participants across a diverse population. KEYWORDS: Chemical peel, peel, microneedling, skin rejuvenation, hyperpigmentation, photoaging
Introduction
Facial aging presents a prevalent aesthetic concern, primarily manifesting as cutaneous rhytidosis, laxity, and dyspigmentation. These collectively contribute to a departure from a perceived youthful appearance. The cellular aging process of the skin can be attributed to intrinsic factors, such as genetics, and extrinsic factors, such as sun exposure and lifestyle. These factors influence the visible manifestations of skin aging such as wrinkles and melanosis.1
Hyperpigmentation is a common condition affecting all skin types that can have a significant effect on self-esteem and confidence.2,3 It is most often caused by sun exposure that triggers an increase in melanin synthesis but can also be caused by dermatologic conditions such as acne, hormones, genetics, or trauma to the skin.4 Many options are available for the treatment of hyperpigmentation, including oral medications, topical formulations, laser therapy, and chemical peels.
Chemical peels are one of the most popular noninvasive cosmetic procedures. Chemical peeling works by delivering caustic actives that denature the proteins and coagulate keratin on the skin surface, triggering a healing response.5 This leads to epidermal growth that improves the skin texture and appearance. Different types and combinations of peeling agents offer different degrees of penetration into the skin, allowing for treatment for a wide range of skin concerns.6
Microneedling is considered to be an effective, noninvasive treatment technique. During the microneedling treatment, fine needles create controlled injuries to the skin to stimulate an increased production of extracellular proteins such as collagen and elastin.7 Microneedling originated as a treatment for skin rejuvenation, but it has been successfully used to treat a variety of skin concerns including hyperpigmentation, acne, scarring, and primary hyperhidrosis.8
By combining a pigment-correcting peel with microneedling, we were able to offer a synergistic treatment for facial signs of aging. While chemical peels effectively improve skin texture and tone through controlled exfoliation and microneedling stimulates collagen and elastin production by inducing a healing response, their combined use can provide a comprehensive treatment of textural and pigmentary concerns, leading to enhanced efficacy in correcting hyperpigmentation and improving overall skin rejuvenation, ultimately restoring a more youthful appearance.
This study was designed to evaluate the efficacy of microneedling combined with a pigment-correcting peel containing a mixture of lactic, mandelic, pyruvic, and tranexamic acids (PCA Skin Pigment Correct Peel; Colgate-Palmolive Co.) compared to microneedling alone on hyperpigmented skin after a series of 3 treatments.
Methods
This prospective, split-face, dermatologist-investigator blinded, single-arm study conducted at a single center was approved by the U.S. Investigational Review Board, Inc. All participants signed informed consent and the study was conducted according to Good Clinical Practice guidelines.
A total of 31 patients with Fitzpatrick skin types I to V, aged 33 to 65 years, with facial hyperpigmentation (18 with melasma, 13 with overall hyperpigmentation) were enrolled. Participants in the study panel included patients of White, Hispanic or Latino, Black or African American, and Asian descent. Patients were eligible for study inclusion if they were men or nonpregnant, nonlactating women with Fitzpatrick skin types I to VI with mild to moderate signs of photoaging (balanced on both sides of the face, as assessed by the investigator). Exclusion criteria included history of keloid formation or hypertrophic scarring, or excessive sun exposure and use of tanning beds or tanning creams in the 30 days prior to treatment.
Participants underwent a total of 4 study visits over 12 weeks. A series of 3 treatments (peel + microneedling on 1 side of the face; microneedling alone on the opposite side as per randomization) were performed every 4 weeks. On the side treated with the peel and microneedling, a total of 2 layers of the peel were applied with an interval of 5 minutes between layers; the peel was administered prior to microneedling. Microneedling was performed on both sides of the face with 3 passes (horizontal, vertical, and circular) at a depth of 0.5 mm each pass using the SkinPen Microneedling System (Crown Aesthetics). The peel was applied before the microneedling in every treatment, allowing for it to self-neutralize before the skin barrier was breached by the microneedling procedure, significantly decreasing the risk of unpredictable systemic absorption and potential adverse reactions that could arise if the acid seeped too deeply into the open channels. Applying the peel first also allowed the dermatologist to monitor the skin’s reaction before administering the microneedling treatment.
Participants were instructed to use a post-treatment regimen consisting of a gentle cleanser, 1% hydrocortisone healing cream, moisturizer, sunscreen, and an ointment for 5 to 7 days after each treatment. For the rest of the study duration, patients were instructed to continue their usual personal skincare regimen from prior to study entry, except for any products intended to treat pigmentation or discoloration, and to not introduce new products into their regimen during the course of the study.
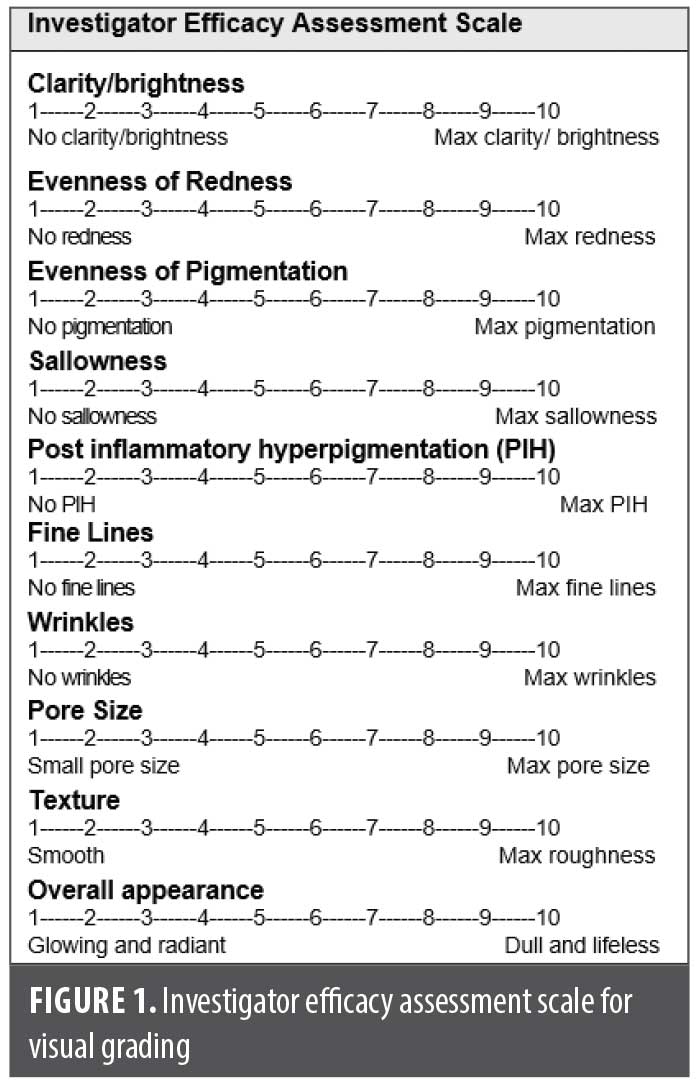
Clinical grading for efficacy, safety/tolerability assessments, and instrumental measurements were conducted at baseline, Weeks 4 and 8 before treatment, and at Week 12 (4 weeks after the last treatment). Facial clinical images were also acquired at these visits. Clinically graded efficacy parameters, including clarity/brightness, evenness of skin tone (redness and pigmentation), sallowness, postinflammatory hyperpigmentation (PIH), fine lines, wrinkles, pore size, texture, and overall appearance, were evaluated on a 10-point scale (Figure 1). Safety/tolerability was evaluated by the investigator by assessing the presence of erythema, scaling, crusting, peel-induced hyperpigmentation, peel-induced hypopigmentation, and scarring. If any of the assessed safety/tolerability parameters was present during follow-up visits, patients would be excluded from further treatments. The Reflectance-Based Pigmentation Meter was used to measure changes in pigmentation of the skin. A total of 11 measurements were taken from both sides of the forehead, both sides mid-cheek 4 cm medial to the tragus, both sides of the chin, and both sides of the nose. The findings were recorded and then averaged separately for each side. Clinical photography of the front, right, and left face was acquired using a standardized clinical imaging booth.
Self-assessment questionnaires were completed by patientes immediately after the first treatment, 1 week after the initial treatment, and 4 weeks after the last treatment at Week 12. Immediately after the first peel and microneedling treatment, prior to receiving microneedling alone on the opposite side of the face, participants were asked to respond to an open-ended self-perception question on the state of their skin. One week after the treatment and 4 weeks after the last treatment, patients completed self-assessment questionnaires where they rated statements regarding the condition of their skin on a 5-point scale for level of agreement.
Descriptive statistics were calculated for clinical grading and instrumental measurements. Changes from baseline and between-treatment comparisons for clinical grading were evaluated using a signed rank test. For instrumental measurements obtained via the Reflectance-Based Pigmentation Meter, changes from baseline were assessed using a t test, while between-treatment differences were analyzed using analysis of covariance. The self-perception questionnaire responses were summarized by frequency of responses for each question, with within-treatment analyses conducted via top box analysis. All statistical tests of hypothesis were conducted at a significance level of α=0.05.
Results
All 31 patients completed the study. Enrolled participants were aged 33 to 65 years and had Fitzpatrick skin types ranging from I to V. All participants presented hyperpigmentation: 18 with melasma, 13 with overall hyperpigmentation.
There were no serious adverse events reported during the study. While all the patients tolerated the procedures well, 2 patients noted erythema lasting up to 3 days on both the microneedling-treated and combination-treated sides of the face. Discomfort with the microneedling was reported by 7 of patients at the first visit but not at subsequent visits. No other tolerability issues or adverse events related to the peel were noted by the participants or the investigator for the duration of the study.
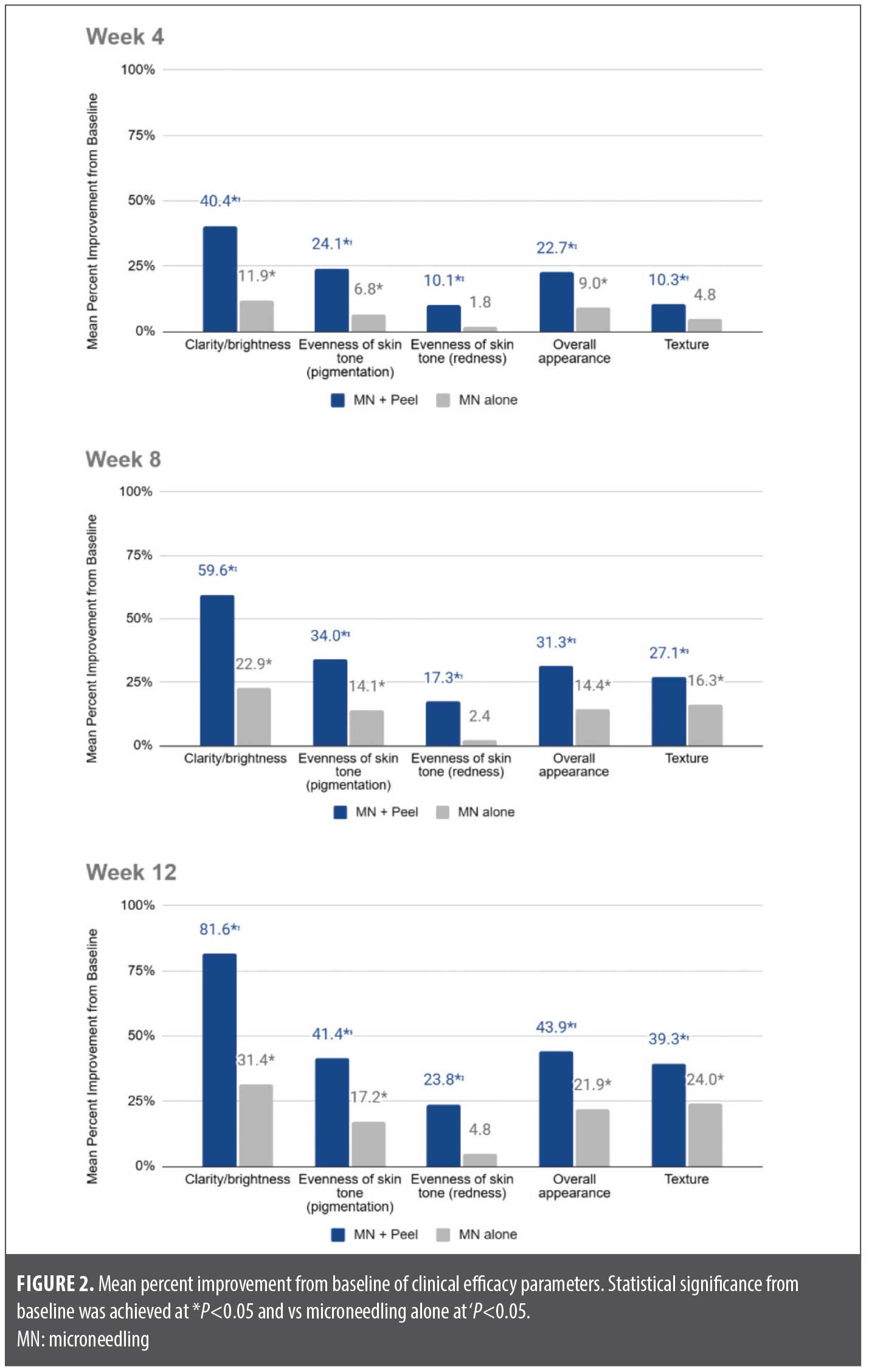
Visual evaluation for clarity/ brightness, evenness of skin tone (pigmentation), and overall appearance by the investigator showed a statistically significant improvement from baseline for both microneedling plus peel and microneedling alone at Weeks 4, 8, and 12 (all P<0.05). Visual assessment of evenness of skin tone (redness) showed a significant improvement (P<0.05) at all visits for the combined treatment but no significant improvement was observed on the side treated with microneedling alone. Visual evaluation of texture showed a significant improvement at all vists (P<0.01) for the combined treatment, while improvement was only significant at Weeks 8 and 12 for microneedling alone (P<0.01). For all of the above-mentioned parameters,; a greater significant improvement was seen on the side treated with the peel and microneedling (all significant vs microneedling alone; P<0.05; Figure 2). Some improvement from baseline was seen for other visually graded parameters such as sallowness, PIH, fine lines, wrinkles, and pore size for both treatments, but not all of them were significant vs baseline and no significant differences between treatments were noted.
Reflectance-Based Pigmentation Meter measurements, which objectively measure skin pigmentation, indicated an overall improvement with both treatments. However, these improvements were not statistically significant when compared to the initial baseline for either treatment at any point. Furthermore, no statistically significant difference was observed between the 2 treatments.
One week after the treatment and 4 weeks after the last treatment, participants completed self-assessment questionnaires to rate statements regarding the condition of their skin on a 5-point scale for level of agreement. Responses to the questionnaire indicate that, overall, patients felt the combined treatment of peel and microneedling was more effective than microneedling alone. A majority (94%) saw a significant or noticeable improvement on skin discoloration/hyperpigmentation on the side treated with microneedling plus peel, and 90% reported prefering the results of the combined treatment vs microneedling alone (P<0.0001).
The improvement of facial skin conditions was well captured in clinical digital imaging. Photographs of representative patients clearly show enhanced improvement in fine lines, evenness of skin tone, and overall facial appearance on the side treated with the combination treatment vs microneedling alone in Figure 3.

Discussion
By combining a pigment-correcting peel with microneedling, we offered a synergistic approach to address the multifaceted concerns of facial aging, including textural and pigmentary concerns. Facial aging, driven by both intrinsic and extrinsic factors, often manifests as hyperpigmentation due to increased melanin synthesis. While chemical peels effectively improve skin texture and tone through controlled exfoliation and microneedling stimulates collagen and elastin production by inducing a healing response, their combined use can provide a more comprehensive treatment. This dual approach targets both pigmentary and textural irregularities, leading to enhanced efficacy in correcting hyperpigmentation and improving overall skin rejuvenation, ultimately restoring a more youthful appearance.
This study successfully established the safety of combining a pigment-correcting peel and microneedling treatment across a diverse population, allowing for enhanced cosmetic outcomes that are safe for all Fitzpatrick skin types, including skin of color. No serious adverse events were reported, and the main discomfort reported by patients was transient and related to the microneedling procedure itself. Post-treatment erythema, dryness, and irritation were minimal, even on the areas that received the combined treatment.
When compared to microneedling alone, the combination treatment led to a quicker and more significant improvement across most of the clinically graded parameters. By Week 12, there was greater improvement in skin clarity/ brightness by 50%, evenness of skin tone (pigmentation) by 24%, evenness of skin tone (redness) by 19%, overall appearance by 22%, and skin texture by 15% for the combination treatment compared to microneedling alone. The self-reported findings regarding improvement as early as Week 1 further reinforce the clinical findings.
While both treatments showed mild improvements in fine lines, wrinkles, and pore size assessments by the dermatologist, the observed progress after 3 sessions suggests that further enhancement could be achieved with additional treatments. Future research could explore the efficacy of pairing this peel formula with other aesthetic treatments, such as fractional laser resurfacing, to potentially enhance the reduction of rhytids. The lack of statistically significant improvement in skin pigmentation measurements may be attributed to the melanin measurement being confined to a small area that may not fully capture the overall improvement clinically observed by the dermatologist and evident in standardized clinical photographs. While the Reflectance-Based Pigmentation Meter provides highly specific, localized data, the subsurface melanin image analysis technology available in the standardized clinical macroscopic imaging system can be used to analyze the whole face or a large region simultaneously. If used in this study, the results might have aligned better with the observed improvement in pigmentation.
The study’s duration showed to be a methodological constraint, as the assessment period ended before the peak therapeutic effect could be seen for structural concerns such as fine lines, wrinkles, and pore size.
Conclusion
The combination of a pigment-correcting peel and microneedling targets both pigmentary and textural irregularities, leading to enhanced efficacy in correcting hyperpigmentation and improving overall skin appearance and self-confidence. The combined therapy proved safe and effective across a diverse population. No serious adverse events were reported or observed, and the investigator identified no safety issues.
References
- Goodman GJ, Bagatin E. Photoaging and cosmeceutical solutions in sun-overexposed countries: the experience of Australia and Brazil. J Eur Acad Dermatol Venereol. 2024;38(Suppl. 4):36–44.
- França K, Keri J. Psychosocial impact of acne and postinflammatory hyperpigmentation. An Bras Dermatol. 2017;92(4):505–509.
- Platsidaki E, Efstathiou V, Markantoni V, et al. Self-esteem, depression, anxiety and quality of life in patients with melasma living in a sunny Mediterranean area: results from a prospective cross-sectional study. Dermatol Ther (Heidelb). 2023;13(5):1127–1136.
- Thawabteh AM, Jibreen A, Karaman D, Thawabteh A, Karaman R. Skin pigmentation types, causes, and treatment–a review. Molecules. 2023;28(12):4839.
- Soleymani T, Lanoue J, Rahman Z. A practical approach to chemical peels: a review of fundamentals and step-by-step algorithmic protocol for treatment. J Clin Aesthet Dermatol. 2018;11(8):21–28.
- Rendon MI, Berson DS, Cohen JL, Roberts W, Starker I, Wang B. Evidence and considerations in the application of chemical peels in skin disorders and aesthetic resurfacing. J Clin Aesthet Dermatol. 2010;3(7):32–43.
- Jaiswal S, Jawade S. Microneedling in dermatology: a comprehensive review of applications, techniques, and outcomes. Cureus. 2024;16(9):e70033.
- Cohen BE, Elbuluk N. Microneedling in skin of color: a review of uses and efficacy. J Am Acad Dermatol. 2016;74(2):348–355.