J Clin Aesthet Dermatol. 2026;19(6):44–45.
by Margaret G. Mercante, BA; Emily G. Tocco, BS; and Diego R. Dasilva, MD
Mses. Mercante and Tocco are with the University of Virginia School of Medicine, Charlottesville, Virginia. Dr. Dasilva is with Forefront Dermatology and Eastern Virginia Medical School, Virginia Beach, Virginia.
FUNDING: No funding was provided for this article.
DISCLOSURES: Dr. Dasilva reports AbbVie, Arcutis, Dermavant, Galderma, Janssen, LEO Pharma, Lilly, Pfizer, Sanofi & Regeneron, UCB, and Verrica. Mses. Mercante and Tocco have no relevant conflicts of interest.
Sarcoidosis and atopic dermatitis (AD) are chronic inflammatory conditions with distinct immunologic profiles but overlapping disparities in prevalence and severity among Black Americans populations. We report a rare case of a 58-year-old Black woman with refractory cutaneous sarcoidosis and AD overlap, who presented with severely pruritic, erythematous, scaly lesions primarily on the face, scalp, and neck. Histopathologic examination revealed granulomatous inflammation. Standard topical and systemic therapies were ineffective. Initiation of upadacitinib, a selective Janus kinase (JAK) inhibitor, resulted in dramatic symptom improvement within 1 month, with a pruritus reduction from a peak pruritus Numeric Rating Scale score of 9/10 to 1/10. This case underscores the therapeutic potential of JAK inhibition in addressing convergent inflammatory pathways across traditionally distinct dermatoses, particularly in patients from populations at increased risk for treatment-refractory disease. Keywords: Sarcoidosis, atopic dermatitis, JAK inhibitors, case report, racial disparities
Introduction
Sarcoidosis is a multisystem chronic inflammatory disorder with a predilection for the skin and lungs. It is characterized by granulomatous inflammation and carries a significantly higher prevalence and severity among Black Americans in the United States. This disparity manifests as more extensive multi-organ involvement, increased hospitalization rates, and worse overall prognosis compared to other racial and ethnic groups.1,2 Similarly, atopic dermatitis (AD) is a chronic inflammatory skin disease marked by intensely pruritic and often painful lesions. AD disproportionately impacts Black and Latinx populations, which tend to experience more severe disease presentations and an increased burden of associated comorbidities.3
Here, we report a unique and noteworthy case of a Black woman presenting with an overlap of cutaneous sarcoidosis and AD. The patient provided informed consent and photo consent. Despite significant disease burden and failure of standard treatments, this patient achieved remarkable clinical improvement with upadacitinib, a selective Janus kinase (JAK) inhibitor. This case provides insights into the intersection of immune dysregulation in sarcoidosis and AD and emphasizes the potential for JAK inhibition to address overlapping inflammatory pathways in complex, refractory conditions.
Case Description
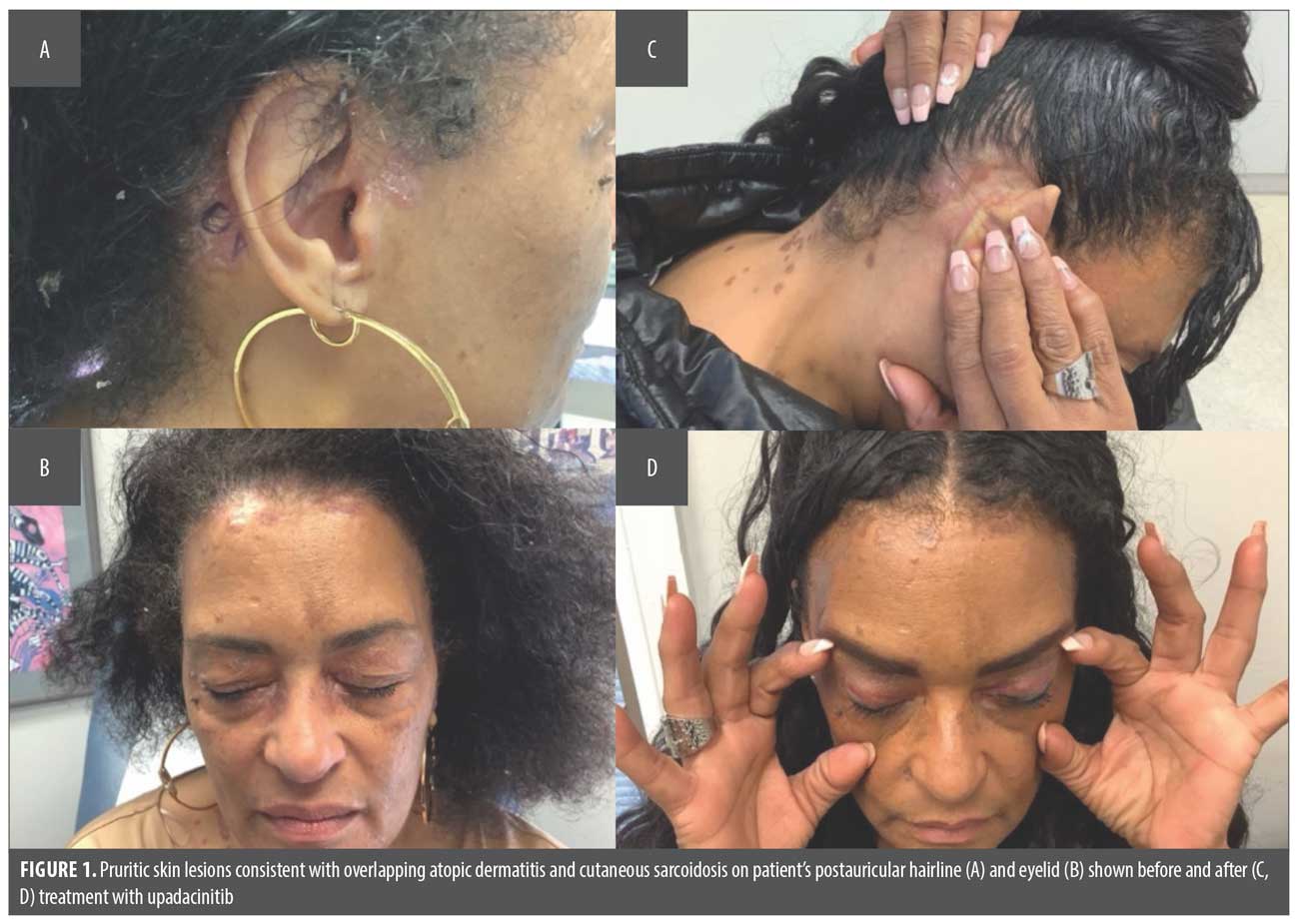
A 58-year-old Black female patient with a history of childhood-onset AD, pulmonary sarcoidosis, and hypertension presented with a 6-month history of progressive and severely pruritic skin lesions. These erythematous, scaly patches, papules, and plaques were predominantly distributed on her face, neck, scalp, hairline, and eyelids, with a peak pruritus Numerical Rating Scale (PP-NRS) score of 9/10.
The patient was previously treated with topical corticosteroids and calcineurin inhibitors (eg, tacrolimus), which yielded minimal improvement. Systemic corticosteroids (prednisone) provided temporary symptom relief but were not a sustainable solution due to mood lability and disease recurrence.
A saucerization biopsy of 0.1-cm depth was obtained from the postauricular hairline and demonstrated noncaseating granulomatous inflammation within the dermis. In the appropriate clinical context, these findings were compatible with AD and cutaneous sarcoidosis. Special stains for microorganisms were negative. Laboratory workup, including complete blood count, comprehensive metabolic panel, infectious studies, and inflammatory markers, was unremarkable.
Given the recalcitrance of her symptoms to initial therapies and the clinical overlap of her conditions, upadacitinib 15 mg daily was initiated. The patient tolerated the treatment well, and at her 1-month follow-up, she reported dramatic symptom improvement. The erythema, scaling, and pruritus had almost completely resolved, with a reduction in PP-NRS from 9/10 to 1/10. (Figure 1)
Discussion
The coexistence of cutaneous sarcoidosis and AD is rare but raises important questions regarding the potential interplay between distinct inflammatory conditions. While it remains unclear whether they are connected by shared immune dysregulation pathways or represent entirely independent disease processes, their simultaneous occurrence in this patient underscores the need for further research into overlapping mechanisms. It also highlights how JAK inhibition can be harnessed as a targeted yet comprehensive method of blocking distinct immune pathways.
Both sarcoidosis and AD impose a higher disease burden on Black patients, likely reflecting a combination of genetic, immunologic, and socio-environmental factors. Sarcoidosis is characterized by granulomatous inflammation driven predominantly by a helper T-cell (Th) type 1 immune response.4 Conversely, AD involves a Th2-dominated inflammatory pathway, which results in increased production of cytokines such as interleukin (IL) 4, IL-13, and IL-31.5 Despite these differing immunologic profiles, both diseases share cytokine signaling mediated via the JAK-signal transducer and activator of transcription pathway.6,7
Upadacitinib, a selective JAK inhibitor, targets multiple immune pathways, offering a novel therapeutic option for managing immune-mediated inflammatory diseases. In this case, the inhibition of overlapping cytokine pathways via JAK inhibition provided significant clinical benefit, reducing both Th1-driven granulomatous inflammation in sarcoidosis and Th2-mediated inflammation in AD.
This case also highlights the importance of considering JAK inhibitors as a versatile treatment option for complex, overlapping inflammatory conditions, particularly in patients from minority populations who are disproportionately affected. As JAK inhibitors become increasingly integrated into the therapeutic landscape for inflammatory skin diseases, further studies are needed to elucidate their long-term efficacy and safety in managing coexisting conditions like sarcoidosis and AD.
References
- Mirsaeidi M, Machado RF, Schraufnagel D, Sweiss NJ, Baughman RP. Racial difference in sarcoidosis mortality in the United States. Chest. 2015;147(2):438–449.
- Sitaru S, Zink A, Biedermann T, Steimle-Grauer SA. Concomitant sarcoidosis, psoriasis, and eczema – immune patterns on the skin. Orphanet J Rare Dis. 2024;19(1):404.
- Croce EA, Levy ML, Adamson AS, Matsui EC. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol. 2021;148(5):1104–1111.
- Miyagaki T, Asano Y, Shibata S, et al. The development of Th1-mediated sarcoidosis improves the clinical course of Th2-mediated atopic dermatitis. Mod Rheumatol. 2011;21(4):406–409.
- Mohamed MF, Bhatnagar S, Parmentier JM, Nakasato P, Wung P. Upadacitinib: mechanism of action, clinical, and translational science. Clin Transl Sci. 2024;17(1):e13688.
- Guttman-Yassky E, Irvine AD, Brunner PM, et al. The role of Janus kinase signaling in the pathology of atopic dermatitis. J Allergy Clin Immunol. 2023;152(6):1394–1404.
- Miedema J, Cinetto F, Smed-Sörensen A, Spagnolo P. The immunopathogenesis of sarcoidosis. J Autoimmun. 2024;149:103247.