J Clin Aesthet Dermatol. 2026;19(7):33–37.
by Sandi Assaf, BS, and Peter Lio, MD
Ms. Assaf is with Sam Houston State University College of Osteopathic Medicine, Huntsville, Texas. Dr. Lio is with Medical Dermatology Associates of Chicago and Northwestern University Feinberg School of Medicine, Chicago, Illinois.
FUNDING: No funding was provided for this article.
DISCLOSURES: Dr. Lio reports being on the speaker’s bureau for AbbVie, Arcutis, Galderma, Incyte, La Roche-Posay/L’Oréal, Lilly, Pfizer, Pierre-Fabre Dermatologie, Regeneron/Sanofi Genzyme, and Verrica; reports consulting/advisory boards for Alphyn Biologics, AbbVie, Almirall, Amyris, Apogee, Arcutis, Astria Therapeutics, Castle Biosciences, Codex Labs, Concerto Biosci, Dermavant, Galderma, Kenvue, LEO Pharma, Lilly, Lipidor, L’Oréal, Merck, Micreos, MyOR Diagnostics, Nektar Therapeutics, Nia Health, Pelthos Therapeutics, Phyla, Regeneron/Sanofi Genzyme, Sibel Health, Skinfix, Song Lab Skincare, Soteri Skin, Stratum Biosciences, Sun Pharma, Theraplex, Thimble Health, Topaz Biosciences, Unilever, Verdant Scientific, Verrica, and Yobee Care; and reports stock options with Akeyna, Inc., Alphyn Labs, Codex Labs, Concerto Biosci, Song Lab Skincare, Soteri Skin, Stratum Biosciences, Thimble, Topaz Biosciences, Yobee Care, and Verdant Scientific. In addition, Dr. Lio has a patent pending for a Theraplex product with royalties paid and is a Scientific Advisory Committee Member emeritus of the National Eczema Association. Ms. Assaf has no relevant conflicts of interest.
Abstract: Key therapeutic options for dermatologic care frequently extend beyond prescription medications to include evidence-based, over-the-counter (OTC) topicals that meaningfully influence disease pathophysiology. We introduce the concept of active dermatologic care (ADC), which encompasses nonprescription topical products with biologically active compounds that support and modulate key skin disease processes and can be routinely incorporated into comprehensive dermatologic care plans. We expand upon the recent concept of categorizing OTC active ingredients for acne based on their mechanisms of action and apply it to atopic dermatitis. The pathophysiologic pillars of itch, barrier dysfunction, acid mantle disruption, dysbiosis, and inflammation are each considered as potential therapeutic targets for ADC. Keywords: Atopic dermatitis, disease management, skin barrier dysfunction, type 2 inflammation, integrative dermatology, pruritus, cutaneous microbiome
Introduction
Dermatology is unique among medical specialties in that a substantial proportion of therapies are delivered topically, as alternatives or adjuncts to systemic treatments. Many of these topical agents are available over the counter (OTC) under United States Food and Drug Administration (FDA) monographs, permitting biologically active ingredients to be incorporated into nonprescription products. As a result, key therapeutic options for dermatologic care frequently extend beyond prescription medications to include evidence-based, nonprescription interventions that meaningfully influence disease pathophysiology. In this paper, we introduce the concept of active dermatologic care (ADC), which encompasses nonprescription topical products with biologically active compounds that support and modulate key skin disease processes and can be routinely incorporated into comprehensive dermatologic care plans. These compounds may include FDA OTC monograph agents as well as dietary bioactives and botanical extracts. This expands upon a concept recently introduced by Baldwin et al,1 which categorizes OTC active ingredients for acne based on their mechanisms of action. A second paper with a similar theme by Baldwin et al2 coined the more acne-specific term for these dermocosmetic products as “acneceuticals.” Baldwin et al1 used expert consensus to select active ingredients that address 5 principal therapeutic goals in acne management: keratolysis, antimicrobial activity, anti-inflammatory effects, sebum reduction, and barrier repair.
While this approach was developed in the context of acne, it underscores the principle that nonprescription topical agents can be strategically selected, either alone or in combination, to target discrete pathogenic pathways in inflammatory skin disease. Many of these therapeutic goals, particularly inflammation control and barrier support, are shared across a range of dermatologic conditions. However, atopic dermatitis (AD) represents a distinct inflammatory disorder with unique pathophysiologic drivers, including epidermal barrier dysfunction, neuroimmune dysregulation, and microbiome alteration. Accordingly, the application of ADC to eczema requires condition-specific goals that prioritize related mechanisms and thus its own set of active compounds.
Indeed, while much of the attention in journals, conferences, and continuing medical education is devoted to advances in prescription therapies, the OTC space has experienced a parallel period of substantial growth and innovation that are often underappreciated. Nearly all clinical guidelines for AD emphasize the foundational role of gentle skin care, including regular use of moisturizers and nonirritating cleansers, across disease severities. However, relatively little is written about how to operationalize these recommendations. In practice, clinicians may offer broad guidance while patients and families are left to navigate aisle after aisle of products that differ substantially in composition, biologic activity, and clinical relevance.
In this review, we extend the ADC model to eczema, defining disease-specific therapeutic goals and reviewing nonprescription active compounds in the literature that may support barrier restoration, immune modulation, microbiome balance, and itch relief.
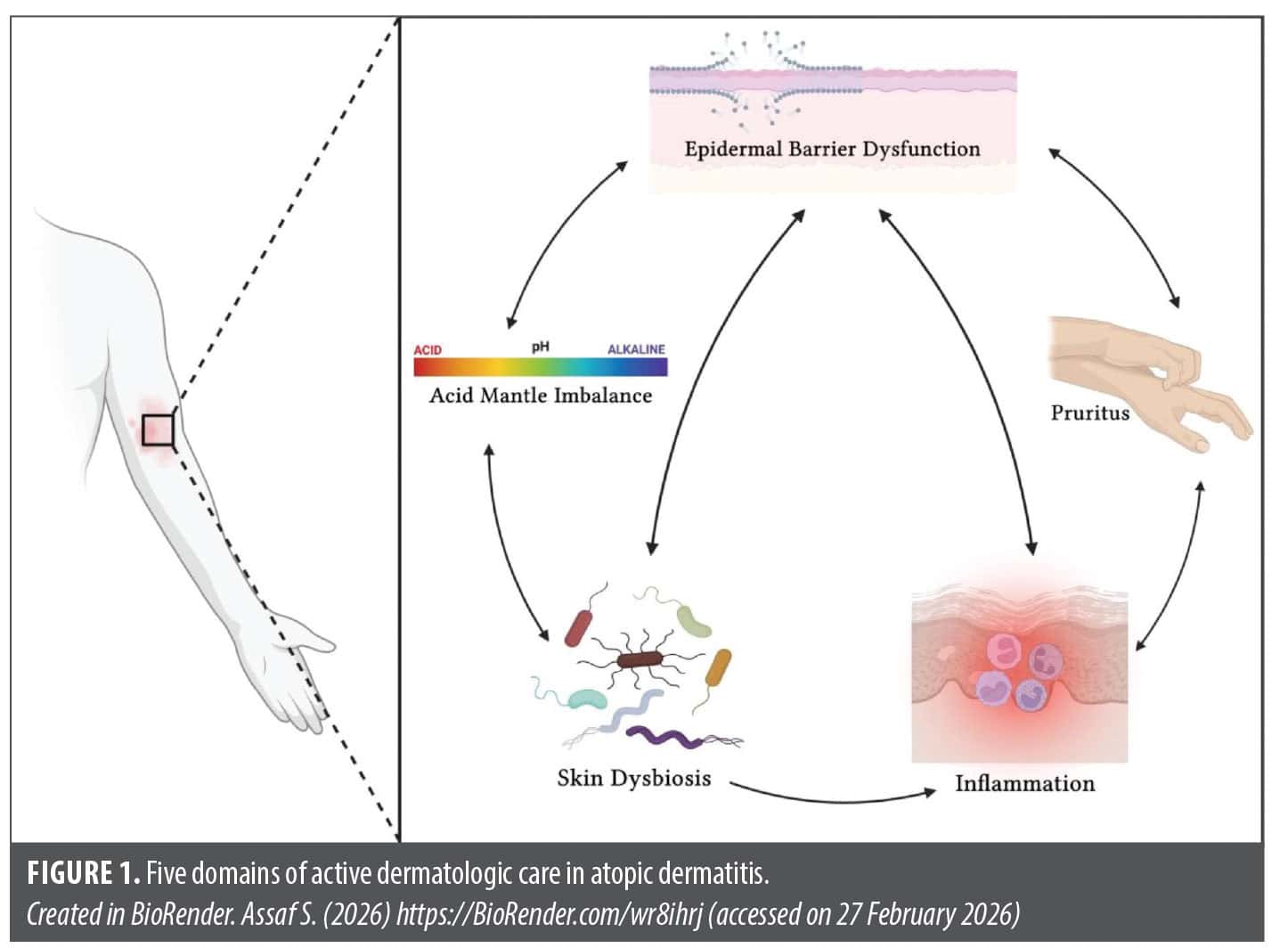
AD is a chronic immune-mediated condition characterized by helper T cell (Th) type 2 lymphocyte–mediated inflammation of the skin.3 This creates epidermal barrier dysfunction with resulting transepidermal water loss (TEWL) that clinically manifests as skin that is pruritic, prone to infection, dry, and hypersensitive.3 The barrier dysfunction in AD can alter the acid mantle and lead to a more alkaline pH of the skin, which can further compromise skin integrity and increase TEWL.4 Given this broad overview of the complex pathophysiology of AD, 5 key target domains for ADC can be used to classify nonprescription topical options: pruritus, epidermal barrier dysfunction, acid mantle imbalance, skin dysbiosis, and inflammation. These target domains are illustrated in Figure 1, which expands on existing diagrams by Dainichi et al.5
Pruritus. Itch is a major source of distress for patients and thus a central target for AD management. Corticosteroids have been central to the management of itch and inflammation for decades; hydrocortisone 0.51% is an OTC option.3,6,7 Topical anesthetics such as lidocaine, benzocaine, and pramoxime function via interference with nerve transmission to provide rapid itch relief.6,7 Strontium is proposed to suppress sensory irritation such as itch without the adverse effects of traditional anesthetics.6,8 Topical capsaicin in concentrations of 0.025% to 0.1% can reduce itch by depleting substance P from sensory nerves and causing an initial burning sensation to counteract itch; however, this mechanism may impact long-term adherence.6 Cooling topicals such as menthol, menthoxypropanediol, and camphor work as antipruritics by depressing sensory receptors and stimulating nerve endings.3,6,7 H1 antihistamine antagonists (topical diphenhydramine) may provide symptomatic relief but are often recommended against due to contact dermatitis concerns.6 Aloe vera (Aloe barbadensis) is known for its soothing properties and can help relieve itch as it is high in magnesium, which inhibits production of histamine.6,9 Witch hazel (Hamamelis virginiana) is another plant that provides itch relief by reducing the release of thymic stromal lymphopoietin and C-C motif chemokine ligand 26 (CCL26), which are involved in eosinophil recruitment.6,10
Colloidal oatmeal is also an effective antipruritic emollient used for eczema that functions by soothing irritation and itch.7 Paraffin and mineral oil are both derived from petroleum and also act as emollients that trap moisture to soften and relieve itch.6,11 Borage oil, a major source of γ-linolenic acid, has also been shown to be effective at reducing itch by its metabolism into anti-inflammatory eicosanoids like prostaglandin E1.12,13 Aluminum acetate is a topical that reduces itch through its astringent properties.6 Black tea has also demonstrated efficacy in a small set of patients with AD, and although its mechanism as an antipruritic is not fully understood, its tannins have astringent properties.14 Lastly, another emerging topical is resveratrol, which is thought to influence itch partially by its anti-inflammatory nature due to its inhibition of cyclooxygenase.15
A recent publication sought to more fully catalog the wide array of OTC antipruritic products, highlighting the diversity of mechanisms available outside of prescription therapies.6
Epidermal barrier dysfunction. At the center of AD pathophysiology is the dysfunctional epidermal barrier. Underscoring this is the fact that nearly all guidelines recommend daily moisturizers as a mainstay treatment.3 Moisturizers decrease TEWL and can potentially increase natural moisturizing factors that increase hydration of the epidermis and allow for increased water retention.3 Petroleum derivatives such as paraffin and mineral oil, along with colloidal oatmeal, improve skin barrier function.1,3,6,11 Ceramides contribute barrier lipids that help prevent TEWL.1,6,7,16 Certain bioactives such as niacinamide (nicotinamide) and urea increase ceramide production also benefiting the hydrolipid barrier.1,6,7,17
In clinical studies, the following topical botanicals have been found to benefit epidermal barrier dysfunction by decreasing TEWL: comfrey root (Symphyti radix), chicory (Cichorium intybus), chamomile (Chamomilla recutita), glycerin/glycerol, canola oil, sunflower oil, Cannabis sativa L., Aloe vera, sea-buckthorn (Hippophae rhamnoides), Indian gooseberry (Emblica officinalis), gotu kola (Centella asiatica), ashwagandha, rosmarinic acid, Stizolophus balsamita, coffee bean, kombucha berry leaf, fig (Ficus carica), and topical beeswax.16,18,19
Epidermal barrier dysfunction may best be repaired using a combination of humectants such as hyaluronic acid, emollients such as shea butter, and occlusives such as dimethicone; each of these has an anti-inflammatory effect that encourages repair.1,6,18 Some water-soluble acids such as alpha hydroxy acids (AHAs) and beta hydroxy acids (BHAs) repair the epidermis through acidification, allowing for exfoliation and increased cellular turnover.1,4 In contrast, coal tar is a bioactive topical that increases filaggrin expression, thus improving skin barrier function as well as helping to normalize the interleukin (IL)-4 pathway. One study described coal tar as having comparable efficacy to hydrocortisone 1%.3 Panthenol functions as a humectant and barrier-supporting agent, improving stratum corneum hydration.1,19 Zinc oxide and calamine protect the epidermis by different mechanisms but both also exert astringent properties.6 Lastly, cocoa butter can function as an occlusive for the skin barrier as it contains fatty acids and a high amount of triglycerides.6,20
Another publication outlined many botanicals and unconventional approaches supported by varying levels of evidence in greater detail.21
Acid mantle imbalance. One therapeutic domain that is less represented in the recent literature is the acid mantle. Normal skin maintains an acidic pH of approximately 4.5 to 5.5, whereas inflammatory skin diseases such as AD are associated with a shift toward a more alkaline pH. This pH disruption impairs multiple enzymatic and metabolic processes, contributing to increased TEWL and dysregulated skin microbiota.4
Skin surface pH (pHSS) is essential in regulating the metabolism of different ceramides, and in AD, there is a disproportionate increase in short-chain ceramides and a decrease in long-chain ceramides.22 Topical moisturizers and cleansers that are balanced with ceramides may regulate the pHSS and improve the acid mantle.22 Citric acid is another bioactive in OTC topicals that can regulate pHSS as a pH buffer.7 AHAs and BHAs are also available in OTC topicals and work to acidify the skin pH to facilitate cellular function.4 The concept of the acid mantle and pHSS is not yet fully explored in the literature and more research is needed into bioactives, particularly OTC formulations that can regulate skin acidity in patients with inflammatory skin disorders such as AD.
Skin dysbiosis. The skin acts as a physical and immunologic barrier to infection. In AD, abnormalities of the epidermal barrier, immune responses, and skin microbiota are tightly interconnected and influence one another.23 Resident microbes of the epidermis such as Staphylococcus epidermidis decrease while detrimental microbes such as Staphylococcus aureus and Candida albicans may colonize excessively.22 Several topical therapies target skin dysbiosis in AD. OTC probiotic formulations containing Streptococcus thermophilus, Vitreoscilla filiformis, Lactobacillus sakei, Lactococcus lactis, or Roseomonas mucosa have been shown to reduce bacterial burden.24 Indigo naturalis (lindioil ointment) is another OTC option and has demonstrated reductions in S. aureus comparable to topical tacrolimus.25
Antiseptics are a category of OTC topicals that can also help with skin dysbiosis, primarily by inhibition of bacteria on the surface. Chlorhexidine is a cationic bisbiguanide antiseptic that disrupts bacterial cell membranes.23 Povidone-iodine is yet another antiseptic that acts as an antimicrobial by releasing iodine, which oxidizes cellular components in a way that can decrease antibiotic resistance.23
There are also natural topicals available OTC to positively influence the skin microbiome. Medical-grade honey such as manuka contains the enzyme glucose oxidase, which produces hydrogen peroxide, as well as other antibacterial factors such as methylglyoxal and bee defensin-1.23 Virgin coconut oil (VCO) has antibacterial properties due to its lauric acid content and its derivative monolaurin. In one study, VCO was more effective than mineral oil in reducing S. aureus colonization in patients with AD.23 Similarly, small clinical studies found that essential oils such as tea tree, thyme, and oregano have antimicrobial properties primarily due to terpenes that disrupt bacterial cellular membranes.1,23
Zinc is a mainstay of mineral sunscreens and, beyond UV protection, modulates innate immune cells, including macrophages, neutrophils, natural killer cells, and phagocytes, thereby contributing to antimicrobial activity.1,26 Sandalwood album oil (SAO) has also been shown to be antimicrobial to several bacteria, fungi, and viruses implicated in skin infections.21 Antibacterial enzymes are also an area of interest in AD for improving skin dysbiosis, particularly endolysins, bacteriophage-encoded enzymes that have shown efficacy in small trials.23
Several papers dive more deeply into the complex and rapidly evolving ways to manipulate the microbiome more effectively.23,27,28
Inflammation. Several of the bioactives previously discussed have demonstrated anti-inflammatory activity: colloidal oatmeal, resveratrol, hydrocortisone, and coal tar.3,7,15 Additionally, licochalcone A is a flavonoid that decreases inflammation via multiple signaling pathways such as NOD-like receptor protein 3 inflammasome, nuclear factor κ-light-chain-enhancer of activated B cells, phospholipase C/extracellular signal-regulated kinase/signal transducer and activator of transcription 3, activator protein 1, and nuclear factor erythroid 2-related factor 2/heme oxygenase-1.3,7,29 There are others that have been shown to be effective in relieving inflammation associated with AD. Soybean is a legume that contains isoflavones, such as genistein, that inhibit inflammatory cytokines.1,30 Similarly, bakuchiol also acts as an anti-inflammatory and has shown to be well tolerated by patients with AD.1,31 Silymarin is a botanical that has been shown to be therapeutic against several inflammatory symptoms of AD via immunomodulation of inflammatory cytokines.1,32
Cannabidiol, which is a nonpsychoactive compound of Cannabis sativa, has been shown to be anti-inflammatory via immunomodulation of Th2 pathways; a 2% topical application was found to improve inflammation in patients with AD.1,33 Echinacea purpura has also shown relief in patients with AD via a similar pathway: immunomodulation of the cannabinoid 2 receptor.21 SAO has also been implicated as a potential option for AD, particularly due to its inhibition of pro-inflammatory cytokines and symptom relief in a small set of pediatric patients.21
Additional natural agents described in the literature have shown clinical promise in small patient cohorts, including black tea, topical vitamin B12, and indigo naturalis. Other topical therapies are discussed in greater detail elsewhere.21,34
Conclusion
AD is a chronic, relapsing condition that often requires multiple therapeutic approaches tailored to disease severity and patient tolerance. While pharmacologic treatments remain central to care, nonpharmacologic strategies, including OTC topical therapies, textiles, and balneotherapy, play an important supportive role.35 Regulatory constraints limit the claims that OTC products may make for AD, despite the inclusion of active ingredients under FDA monographs. This review summarizes available OTC options that have demonstrated benefit across key therapeutic domains of AD in clinical studies (Table 1). Several bioactives appear to act across multiple domains, underscoring the need for further mechanistic studies and larger, well-designed clinical trials.
References
- Baldwin H, Bui H, Callender V, et al. The use of acneceuticals to improve acne care: introduction of a new term and review of the literature. J Drugs Dermatol. 2025;24(3):281–288.
- Baldwin H, Frey C, Hebert A, et al. Real-world clinical case series utilizing acneceuticals as monotherapy, adjunctive, or maintenance therapy for acne vulgaris. J Drugs Dermatol. 2025;24(6):8421s3–8421s14.
- Fleischer DM, Udkoff J, Borok J, et al. Atopic dermatitis: skin care and topical therapies. Semin Cutan Med Surg. 2017;36(3):104–110.
- Tan IJ, Lio PA. From discovery to modern understanding: the acid mantle in dermatology. J Integr Dermatol. Published online 27 Jan 2025
- Dainichi T, Kitoh A, Otsuka A, et al. The epithelial immune microenvironment (EIME) in atopic dermatitis and psoriasis. Nat Immunol. 2018;19(12):1286–1298.
- MacIntyre D, Lio P. Beyond the prescription pad: a guide to over-the-counter itch management. J Integr Dermatol. Published online 15 Jan 2026.
- Hebert AA, Rippke F, Weber TM, Nicol HN. Efficacy of nonprescription moisturizers for atopic dermatitis: an updated review of clinical evidence. Am J Clin Dermatol. 2020;21(5):641–655.
- Hahn GS. Strontium is a potent and selective inhibitor of sensory irritation. Dermatol Surg. 1999;25(9):689–694.
- Hekmatpou D, Mehrabi F, Rahzani K, Aminiyan A. The effect of aloe vera clinical trials on prevention and healing of skin wound: a systematic review. Iran J Med Sci. 2019;44(1):1–9.
- Piazza S, Martinelli G, Magnavacca A, et al. Unveiling the ability of witch hazel (Hamamelis virginiana L.) bark extract to impair keratinocyte inflammatory cascade typical of atopic eczema. Int J Mol Sci. 2022;23(16):9279.
- Maher S, Lio PA. Non-pharmacologic and lifestyle-based approaches to managing chronic hand eczema: a narrative review. Dermatol Digest. 2025;17–21.
- Wang X, Jia Y, He H. The role of linoleic acid in skin and hair health: a review. Int J Mol Sci. 2024;26(1):246.
- Kanehara S, Ohtani T, Uede K, Furukawa F. Clinical effects of undershirts coated with borage oil on children with atopic dermatitis: a double-blind, placebo-controlled clinical trial. J Dermatol. 2007;34(12):811–815.
- Witte M, Krause L, Zillikens D, Shimanovich I. Black tea dressings – a rapidly effective treatment for facial dermatitis. J Dermatolog Treat. 2019;30(8):785–789.
- Gugleva V, Zasheva S, Hristova M, Andonova V. Topical use of resveratrol: technological aspects. Pharmacia. 2020;67(2):89–94.
- Lei D, Liu D, Zhang J, Zhang L, Man MQ. Benefits of topical natural ingredients in epidermal permeability barrier. Front Physiol. 2024;14:1275506.
- Załęcki P, Jezusek J, Nowicka D. Topical niacinamide in daily skincare: a 3-week real-world cosmetic study. Appl Sci. 2025;15(17):9729.
- Prakoeswa CRS, Damayanti, Anggraeni S, et al. The role of moisturizer containing antiinflammatory on skin hydration in mild-moderate atopic dermatitis patients. Dermatol Res Pract. 2024;2024:3586393.
- Madnani N, Deo J, Dalal K, et al. Revitalizing the skin: exploring the role of barrier repair moisturizers. J Cosmet Dermatol. 2024;23(5):1533–1540.
- Purushothaman VK, Wen TJ, Anne M, et al. Cocoa butter as an effective moisturizer for topical cream. J Nat Remedies. 2025;25(2):391–401.
- Shi K, Lio PA. Alternative treatments for atopic dermatitis: an update. Am J Clin Dermatol. 2019;20(2):251–266.
- Mijaljica D, Townley JP, Klionsky DJ, Spada F, Lai Ml. The origin, intricate nature, and role of the skin surface pH (pHSS) in barrier integrity, eczema, and psoriasis. Cosmetics. 2025;12(1):24.
- Marzouk S, Khan S, Syed S, Lio P. Topical antibacterials in dermatology: novel approaches and emerging therapies. J Integr Dermatol. Published online 6 Nov 2024.
- Frankel D, Lio P. The role of topical probiotics for atopic dermatitis: a systematic review. J Integr Dermatol. Published online 27 Mar 2023.
- Yang CY, Chen CB, Lu CW, et al. Efficacy and safety of indigo naturalis oil extract (lindioil ointment) for the treatment of atopic dermatitis: a randomized, crossover, evaluator-blinded, controlled trial. Front Pharmacol. 2025;16:1546589.
- Gupta M, Mahajan VK, Mehta KS, Chauhan PS. Zinc therapy in dermatology: a review. Dermatol Res Pract. 2014;2014:709152.
- Pintas S, Lio P. Manipulating the microbiome: what is known, what is unknown? J Integr Dermatol. Published online 25 Feb 2022.
- Yu SY, Lio P. External factors and the cutaneous microbiome. J Integr Dermatol. Published online 8 Oct 2024.
- Liu D, Jiang X, Yang F, Zhou J, Li Y, Yang H. Therapeutic potential of licochalcone A in dermatological diseases: from basic to clinical research. Front Pharmacol. 2025;16:1632006.
- Natarelli N, Gahoonia N, Maloh J, Sivamani RK. Clinical efficacy of topical or oral soy supplementation in dermatology: a systematic review. J Clin Med. 2023;12(12):4171.
- Draelos ZD, Gunt H, Zeichner J, Levy S. Clinical evaluation of a nature-based bakuchiol anti-aging moisturizer for sensitive skin. J Drugs Dermatol. 2020;19(12):1181–1183.
- Mady FM, Essa H, El-Ammawi T, Abdelkader H, Hussein AK. Formulation and clinical evaluation of silymarin pluronic-lecithin organogels for treatment of atopic dermatitis. Drug Des Devel Ther. 2016;10:1101–1110.
- Hakim S, Goel S, Papastergiou J, Goldberg DJ. Improvement in atopic dermatitis using a novel topical 2% cannabidiol (CBD) application. Dermatol Rev. 2025;6:e70024.
- Ahuja K, Sunkara M, Lio P. An integrative algorithm for atopic dermatitis. J Integr Dermatol. Published online 25 Mar 2025.
- Lio PA. Non-pharmacologic therapies for atopic dermatitis. Curr Allergy Asthma Rep. 2013;13(5):528–538.