J Clin Aesthet Dermatol. 2026;19(7):28–32.
by Rania Nabil Abd-Elbaky, MBBCh; Ramadan M. Eldahshan, MD; Osama Elshabory, MD; and Mohamed L. Elsaie, MD
Dr. Abd-Elbaky is with the Medical Administration at Al-Azhar University, Cairo, Egypt. Drs. Eldahshan and Elshabory are with the Department of Dermatology, Venereology, and Andrology, Damietta Faculty of Medicine, Al-Azhar University, Damietta, Egypt. Dr. Elsaie is with the Department of Dermatology, Medical Research and Clinical Studies Institute, National Research Centre, Giza, Egypt.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
Abstract: Background: Alopecia areata (AA) is a frequent nonscarring alopecia affecting the body or scalp, distinguished by hair loss without clinical inflammatory indicators. Objective: To compare the efficiency and safety of trichloroacetic acid (TCA), 35%, vs superficial cryotherapy in the treatment of resistant AA. Methods: In a double-armed, single-blinded, randomized clinical trial, 32 patients with resistant AA were randomized into 2 groups of 16 patients each: superficial cryotherapy group and topical TCA group. The first group was treated with superficial cryotherapy administered by spraying liquid nitrogen for 15 seconds, followed by thawing, and repeated for 2 further cycles, every 2 weeks for 3 months (6 sessions). The second group was treated with topical TCA performed once monthly for 3 months (3 sessions). Results: No statistically significant variance was discovered among the examined groups according to Severity of Alopecia Tool (SALT) score before treatment (P=0.93). Following treatment, a SALT score reduction from 10.93±3.90 to 7.28±3.27 was demonstrated among the cryotherapy group and from 10.81±4.91 to 4.46±2.88 in the TCA group. A more significant reduction in alopecia severity (P<0.01) was discovered after treatment among the TCA group. Conclusion: We have demonstrated the efficacy of both treatments with a more significant result favoring TCA. Considering that it is less painful and easier to perform, superficial cryotherapy is especially worthy of application to patients with mild AA and with stable course who have difficulty with conventional treatments. Keywords: Alopecia areata, trichloroacetic acid, cryotherapy
Introduction
Alopecia areata (AA) is a prevalent nonscarring alopecia that affects the body and/or scalp, distinguished by loss of hair without any clinical inflammatory indicators. It is one of the most prevalent forms of hair loss observed by dermatologists, constituting 25% of all alopecia cases.1 AA is classified as resistant only if it has not responded to a minimum of 2 distinct treatment modalities. If AA fails to respond after between 3 to 6 months, therapeutic resistance may be deemed probable.2
Multiple investigations have demonstrated that AA impacts 1% to 2% of the general population, with an estimated lifetime risk of 1.7%. Nevertheless, prevalence may fluctuate between 0.1% and 6.9% depending on the population. Several smaller investigations suggest a minor female-to-male gender bias, potentially attributable to greater female concern over hair loss and subsequent therapy.3
The condition may manifest at any age, and the lifetime frequency seems to rise at an almost linear rate.4 The median age at diagnosis is 33 years old.5 Men are more frequently diagnosed in childhood, while women are more susceptible to diagnosis throughout adolescence and demonstrate elevated concomitant nail involvement or related autoimmune disorders.6
Trichloroacetic acid (TCA) is a chemical peeling agent that denatures epidermal proteins and damages the superficial dermis. TCA, 35%, has exhibited efficacy in treating patchy AA. The suggested mechanism of action involves the stimulation of growth factor and cytokines during the wound healing process.7
Superficial cryotherapy (SC) is a brief exposure to liquid nitrogen to induce reactive vasodilation and enhance blood flow, potentially improving microcirculation and nutritional conditions surrounding hair follicles. Cryotherapy is an effective and safe method for treating AA patches.8
This study aimed to compare the efficacy and safety of TCA, 35%, vs SC in the management of resistant AA.
Methods
This single-blinded, double-armed, randomized clinical trial enrolled 32 patients with treatment-resistant AA. Participants were randomly allocated into 2 groups of 16 patients each: one group received SC and the other received topical TCA, 35%. The study was conducted at tertiary-care university-affiliated teaching hospitals including Al-Azhar University Hospital (New Damietta) and Al-Hussein University Hospital (Cairo), Egypt.
Sample size calculation. Sample size was calculated based on the change in the number of hair follicles before and after liquid nitrogen cryotherapy, as previously reported.7 Using G*Power (version 3.1.9.7) and assuming an effect size of 0.769, a 2-tailed test with α=0.05 and 80% power indicated a minimum sample of 16 patients per group. Randomization was performed using a computer-generated random number sequence prepared by an independent investigator. Allocation was concealed using sequentially numbered opaque sealed envelopes. Equal group sizes were achieved through 1:1 allocation.
Inclusion criteria. Patients of both sexes with resistant patchy AA who had discontinued topical treatments, minoxidil lotion, and intralesional corticosteroid injections at least 2 months before enrollment were included. Patients aged 10 years and older were eligible for inclusion.
Exclusion criteria. Patients with current or past scalp dermatoses, recent (within 2 months) use of hair growth–promoting agents, or severe systemic illnesses were excluded.
Ethical considerations. The study protocol and potential risks were explained in detail to participants and guardians. Written informed consent and photographic consent were obtained. Ethical approval was secured from the Institutional Review Board (IRB) of the Faculty of Medicine, Al-Azhar University, Damietta.
Procedures. All participants underwent a comprehensive history, physical examination, and dermoscopic evaluation. Patients were randomized into:
Group A: Treated with SC using liquid nitrogen spray for 15 seconds per cycle, with 2 additional cycles following thawing. Sessions were conducted biweekly over 3 months (6 sessions total).
Group B: Treated with TCA, 35%, monthly for 3 months (3 sessions). The target area was degreased with 70% alcohol and acetone before applying 1 mL of TCA using a cotton-tipped applicator until mild burning or level I frosting occurred. The agent was feathered into surrounding normal skin to avoid demarcation.
Follow-ups occurred at Weeks 4, 8, and 12.
Outcome measures. Efficacy was assessed using the Severity of Alopecia Tool (SALT) score, clinical hair regrowth, dermoscopic evaluation, and photographic documentation. Progressive disease was defined as enlargement of existing patches or appearance of new lesions during the preceding three months, whereas stable disease was defined as absence of new lesions and no increase in lesion size during the same period. Clinical improvement was categorized according to percentage hair regrowth relative to baseline as follows: no improvement (<10%), mild improvement (10–25%), moderate improvement (26–50%), and excellent improvement (>50%).
Trichoscopic assessment was performed with a handheld polarized dermoscope. Images were captured using a digital single-lens reflex camera and reviewed by a blinded dermatologist. The SALT score categorizes AA severity as 1 to 20 (mild), 21 to 49 (moderate), 50 to 94 (severe), and 95 to 100 (very severe).8
Statistical analysis. Data were analyzed using SPSS version 22. Qualitative variables were presented as counts and percentages. The Shapiro-Wilk test assessed normality of quantitative variables, which were expressed as means±SD (normal distribution) or median (range) for non-normal data. Statistical tests included χ2, Mann-Whitney U, and t test, as appropriate.
Results
Demographics and baseline characteristics. The mean age in the SC group was 24.37±9.72 years (range: 10–41) vs 25.37±10.97 years (range: 10–45) in the TCA group. Female patients constituted 53.1% (n=17) of the total study population, and male patients comprised 46.9% (n=15). The average disease duration was 8.25±2.38 months (range: 5–13), and 47.5% of patients reported a positive family history of AA in a first-degree relative. No statistically significant differences were observed between the groups in terms of age, sex, disease duration, progression, or family history (Table 1).
Baseline trichoscopic findings. Prior to treatment, trichoscopic evaluation revealed yellow dots as the most common feature in the SC group (81.25%), followed by black dots (56.25%), dystrophic hairs (50%), and exclamation mark hairs (18.75%). In the TCA group, dystrophic hairs were most frequent (62.5%), followed by yellow dots (56.25%). The differences between groups in these baseline trichoscopic features were not statistically significant (Table 2).
Post-treatment trichoscopic changes. Both treatment groups exhibited significant reductions in yellow dots, black dots, and dystrophic hairs (P<0.05). While no significant intergroup differences were found in the reduction of black dots, exclamation mark hairs, and dystrophic hairs, the reduction in yellow dots was significantly greater in the TCA-treated group (P=0.02; Table 3).
SALT score analysis. The baseline SALT scores were similar between the 2 groups (SC group: 10.93±3.90; TCA group: 10.81±4.91; P=0.93). Post-treatment SALT score significantly decreased in both groups (P<0.001):
- SC group: 10.93±3.90 to 7.28±3.27
- TCA group: 10.81±4.91 to 4.46±2.88
- The reduction was significantly more pronounced in the TCA group (P<0.01). Regarding clinical outcomes:
- No change was noted in 43.75% of the SC group vs 12.5% of the TCA group (P=0.04)
- Excellent improvement occurred in 37.5% of the TCA group vs 6.25% of the SC group (P=0.03)
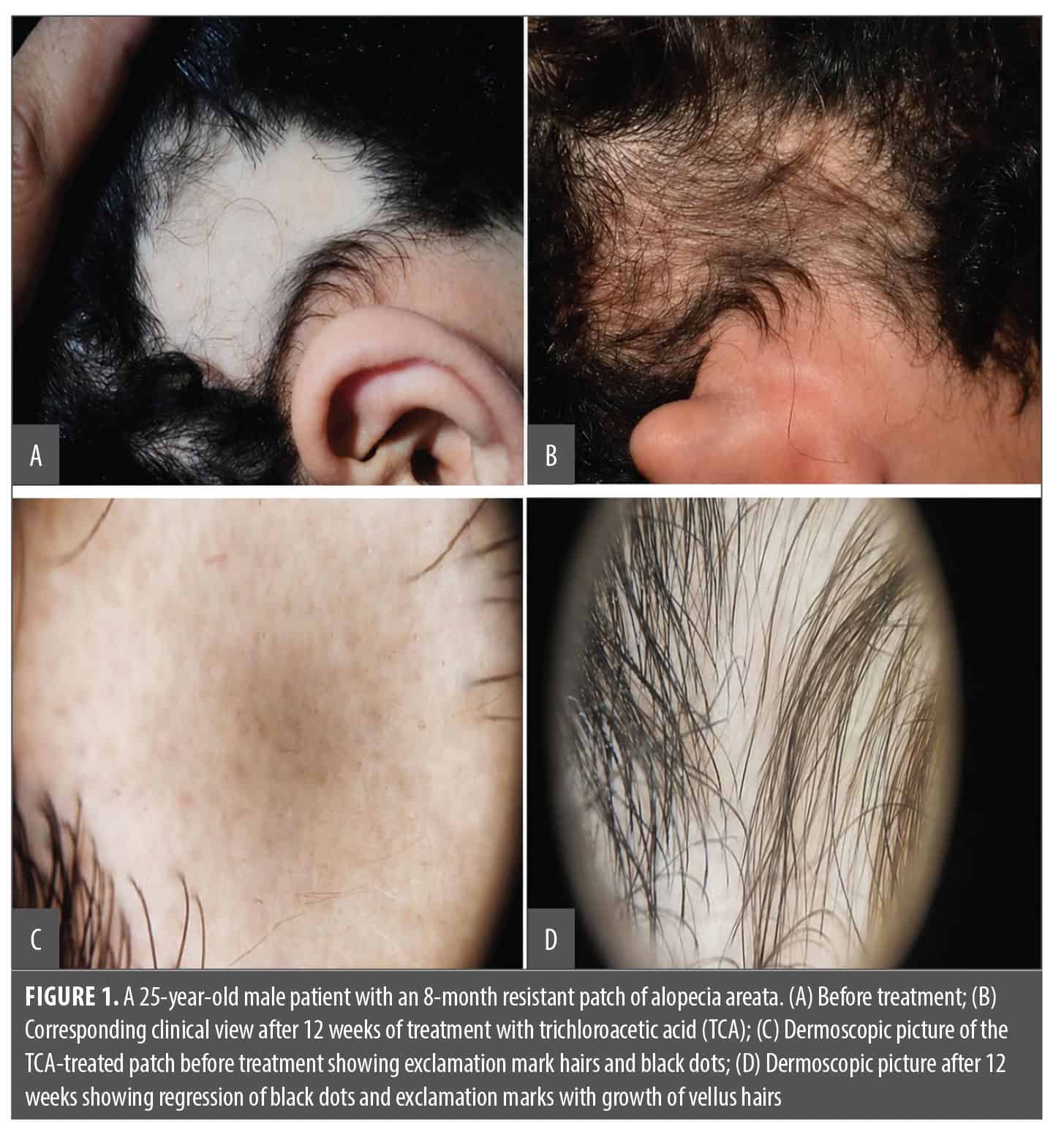
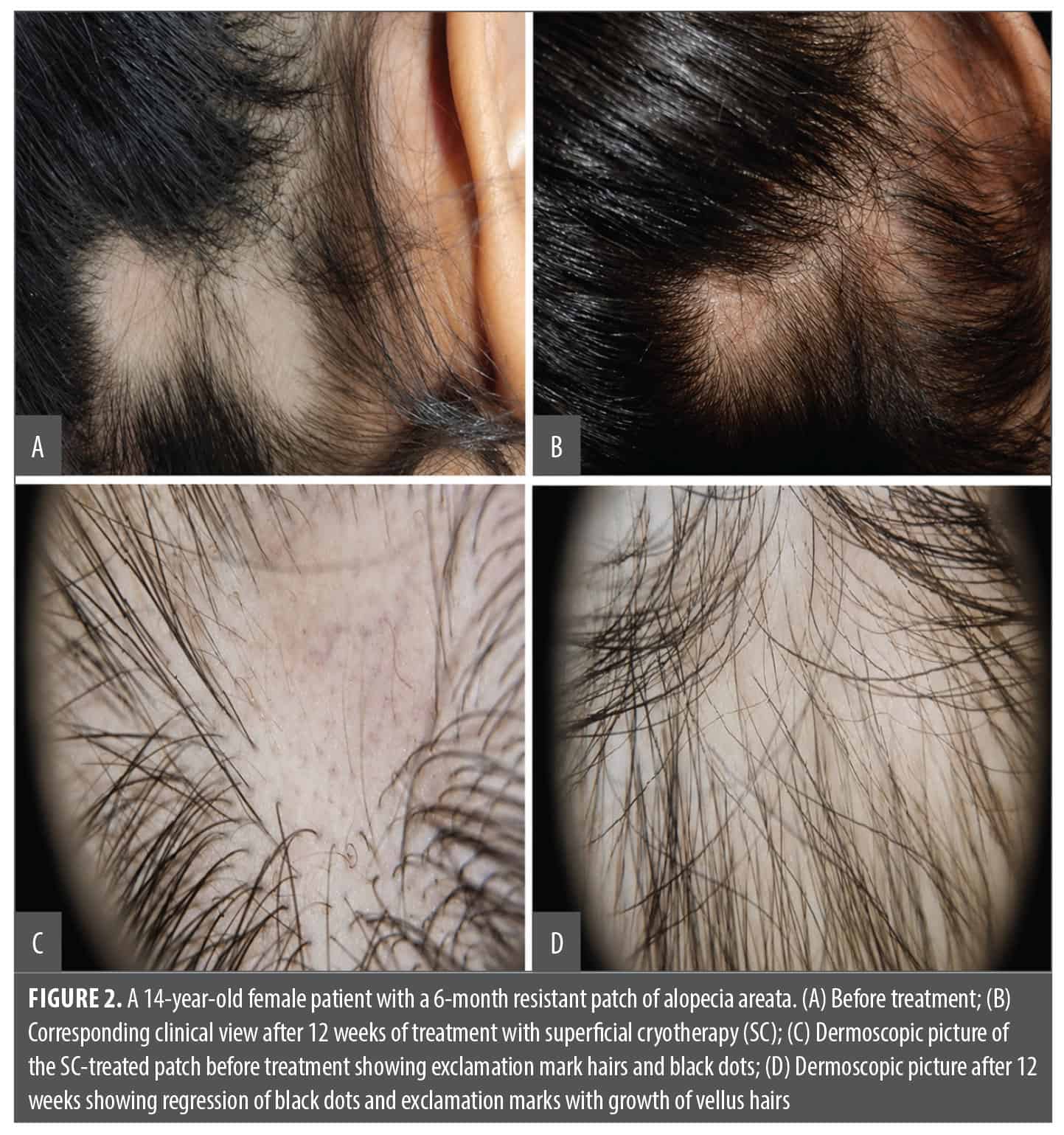
- Differences in mild and moderate improvement were not statistically significant (Table 4, Table 5, Figure 1, Figure 2)
Effect based on disease activity. In the SC group, significant improvement was only seen in patients with stable AA, whereas no significant change was observed in those with progressive disease. Conversely, in the TCA group, a significant reduction in severity was observed in both stable and progressive disease (Table 6).
Patient satisfaction and adverse events. Patient satisfaction was reported by 25% in the SC group and 62.5% in the TCA group, though this did not reach statistical significance (P=0.09; Table 7). All patients experienced mild transient discomfort during treatment. In the SC group, 2 patients developed transient hypopigmentation and 1 experienced vesiculation, which resolved spontaneously. No severe adverse events were reported in either group.
Discussion
AA is an autoimmune condition primarily affecting the scalp but can also involve other hair-bearing areas.1 This study aimed to compare the efficacy and safety of TCA, 35%, vs SC in managing resistant cases of AA.
Both treatment modalities resulted in significant clinical and trichoscopic improvement. However, the TCA group exhibited greater reductions in SALT score and trichoscopic disease markers, particularly yellow dots, suggesting superior efficacy.
Mechanisms of action. The therapeutic effects of TCA may be attributed to its irritant properties, inducing the release of cytokines and growth factors such as platelet-derived growth factor, vascular endothelial growth factor, keratinocyte-derived growth factor, and interleukin (IL)-10.11 Additionally, TCA may promote dermal remodeling and hair follicle stimulation through localized inflammation and immunomodulatory effects, potentially reducing autoreactive T-cell activity.12
Anter et al13 observed clinical improvement in AA using TCA, 35%, reporting a reduction in trichoscopic markers and inflammatory infiltrates on histopathology. Another study comparing intralesional corticosteroids with topical TCA showed comparable efficacy, with TCA significantly reducing all disease activity markers including yellow dots and exclamation mark hairs.14 These findings are consistent with the present study’s results, where TCA achieved superior outcomes compared to cryotherapy.
Comparison with previous cryotherapy studies. Sardana et al15 found cryotherapy to be effective, especially in stable cases, which aligns with our observation that SC was more effective in nonprogressive AA. Cryotherapy has been proposed to enhance circulation and modulate immune responses through localized inflammation and cytokine suppression, including reduced levels of IL-17, IL-1β, and IL-23.16–19
Studies such as that by Huang et al16 and others20,21 have also reported positive outcomes with SC, especially when applied in dual freeze/thaw cycles. A recent meta-analysis demonstrated major and minor regrowth in 26.2% and 37.8% of patients treated with cryotherapy, respectively.22 While our study confirms its utility, TCA demonstrated more consistent improvement across both stable and progressive disease subgroups.
Limitations
The primary limitations include a relatively small sample size, gender imbalance, and limited follow-up duration, which may have impacted the assessment of recurrence. Additionally, the absence of a control (untreated) group limits comparative interpretation. Despite these, the study provides meaningful insight into the comparative efficacy of 2 promising AA treatment options.
Conclusion
Both SC and TCA, 35%, are effective treatments for resistant AA. However, TCA demonstrated significantly superior outcomes in disease severity reduction, trichoscopic improvement, and patient satisfaction. Given its ease of application and effectiveness in both stable and progressive disease, TCA may be considered a preferred therapeutic option.
References
- Elsaie ML, Hasan MS. Successful treatment of long-standing alopecia totalis with intralesional methotrexate. J Cosmet Dermatol. 2022;21(2):855–856.
- Salem AS, Ibrahim HS, Abdelaziz HH, Elsaie ML. Implications of cigarette smoking on early-onset androgenetic alopecia: a cross-sectional study. J Cosmet Dermatol. 2021;20(4):1318–1324.
- Elshahid AR, Kadah AS, Hassan EA, Elsaie ML. Efficacy of Jessener solution versus intralesional steroid in treatment of alopecia areata. J Cosmet Dermatol. 2023;22(2):529–533.
- Pratt CH, King LE Jr, Messenger AG, et al. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011.
- Lee HH, Gwillim E, Patel KR, et al. Epidemiology of alopecia areata, ophiasis, totalis, and universalis: a systematic review and meta-analysis. J Am Acad Dermatol. 2020;82(3):675–682.
- Elsaie LT, Elshahid AR, Hasan HM, Soultan FAZM, Jafferany M, Elsaie ML. Cross sectional quality of life assessment in patients with androgenetic alopecia. Dermatol Ther. 2020;33(4):e13799.
- Elshahed AR, Ammar AM, Ali AM, Elsaie ML. Clinical and dermoscopic assessment of the efficacy of topical trichloroacetic acid 70% versus methoxsalen 0.2% paint in stable acral vitiligo. Sci Rep. 2025;15(1):4756.
- Choe SJ, Lee WS. Efficacy of superficial cryotherapy on the eyebrows of patients with alopecia universalis also treated with contact immunotherapy on the scalp: a prospective, split-face comparative study. Int J Dermatol. 2017; 56(2):184–189.
- Aboeldahab S, Nada EEA, Assaf HA, Gouda ZAE, El-Hamd MA. Superficial cryotherapy using dimethyl ether and propane mixture versus microneedling in the treatment of alopecia areata: a prospective single-blinded randomized clinical trial. Dermatol Ther. 2021;34(5):e15044.
- Olsen EA, Canfield D. SALT II: a new take on the Severity of Alopecia Tool (SALT) for determining percentage scalp hair loss. J Am Acad Dermatol. 2016;75(6):1268–1270.
- Atwa MA, Ahmed AH, Nada HA, Refaey SM, Jafferany M, Elsaie ML. Combined chemical peels versus trichloroacetic acid (TCA) for treating melasma: a split face study. J Dermatolog Treat. 2022;33(2):959–964.
- Aboelghait RM, Zaki AM, El Rewiny EM. Topical 15% lactic acid solution versus topical betamethasone valerate lotion in treatment of multiple patchy alopecia aerate. Al-Azhar Int Med J. 2024;5(2):113–119.
- Anter HM, Zaky AM, Nouh AH, El-Khalawany M. Efficacy of trichloroacetic acid in patients with alopecia areata: a clinico-histopathological study. Int J Med Arts. 2023;5(2):3033–3038.
- Mahgoub D, Mohye Eldeen R, Saadi D, El‐Samanoudy S, Ibrahim S. Clinical and trichoscopic evaluation of trichloroacetic acid 35% vs phenol 88% peels in treatment of alopecia areata. J Cosmet Dermatol. 2021;20(1):143–149.
- Sardana S, Goyal T, Kushwaha P, Jha P. A prospective study to compare the efficacy of cryotherapy versus intralesional steroid in alopecia areata. J Cutan Aesthet Surg. 2022;15(2):175–178.
- Huang P, Huang S, Wei G. One-hundred twenty-three cases of alopecia areata treated with liquid nitrogen cryotherapy. J Clin Dermatol. 1986;15:269.
- Pimentel CB, de Moraes AM, Cintra ML. Angiogenic effects of cryosurgery with liquid nitrogen on the normal skin of rats, through morphometric study. An Bras Dermatol. 2014;89(3):410–413.
- Mesinkovska NA. Emerging unconventional therapies for alopecia areata. J Investig Dermatol Symp Proc. 2018;19(1): S32–S33.
- Lindsay A, Othman MI, Prebble H, Davies S, Gieseg SP. Repetitive cryotherapy attenuates the in vitro and in vivo mononuclear cell activation response. Exp Physiol. 2016;101(7):851–865.
- Nouh AH, Kadah AS, Said M. Comparative study of the use of fractional CO2 laser versus the use of liquid nitrogen cryotherapy in the treatment of alopecia areata in a sample of the Egyptian population. Dermatol Ther. 2022;35(4):e15358.
- Abdel Motaleb AA, Sayed DS. Different freezing time of superficial liquid nitrogen cryotherapy in treatment of recalcitrant alopecia areata: randomized clinical trial. Dermatol Ther. 2020;33(4):e13640.
- Lim SH, Lee WS. Hair regrowth outcomes of superficial cryotherapy in patients with alopecia areata: a systematic review. Ann Dermatol. 2023;35(6):464–467.