 by Hayaat F. Almaary, BDS; Ramakrishnan Karthik, MDS; and Cynthia Scott, MDS
by Hayaat F. Almaary, BDS; Ramakrishnan Karthik, MDS; and Cynthia Scott, MDS
Drs. Almaary, Karthik, and Scott are affiliated with the SRM Kattankulathur Dental College and Hospital in Chennai, India.
J Clin Aesthet Dermatol. 2018;11(5):22–26
Funding: No funding was provided for this article.
Disclosures: The authors have no conflicts of interest relevant to the content of this article.
Abstract: Dimleplasty is the surgical creation of dimples. The demand for dimpleplasty has increased over the past few years. Despite this increasing demand, the most widely used reference point for determining where to place a surgically created dimple, the Khoo Boo Chai (KBC) point, dates back more than 60 years. The aim of our study was to assess the facial shape of a sample of men and women, all of whom had natural dimples, to determine if characteristic patterns in dimple size, location, and shape existed according to each specific facial shapes. For our study, 1,194 people were examined for dimples and of these, 216 individuals with a group total of 336 naturally occurring dimples were included in the study. Facial form was categorized as mesoprosopic, euryprosopic, or leptoprosopic. We found that 54.8 percent of the total dimples were not positioned on the KBC point. In mesoprosopic group, out of 204 dimples, 117 were not positioned on the KBC point (87 were); in leptoprosopic group, out of 66 dimples, 30 dimples were not positioned on the KBC point (36 were); and in the euryprosopic group, out of 66 dimples, 36 were not positioned on the KBC point (30 were). Most of the dimples in the mesoprosopic group were positioned 4mm anterior to the KBC point, and in the eryprosopic group, most dimples were positioned 3mm above and behind the KBC point. Most of the dimples in the leptoprosopic group were positioned on the KBC point. We also observed differing patterns in size and shape between the groups. Understanding these differences could help surgeons achieve optimal outcomes by creating more natural looking and thus more aesthetically pleasing dimples among their patients seeking dimpleplasty.
Keywords: Dimpleplasty, facial form, facial shape, leptoprosopic, mesoprosopic, eryprosopic, Khoo Boo Chai’s point, KBC Point, dimple
Facial dimples, according to the Oxford English Dictionary, are defined as small hollows typically seen on the cheek or chin. The presence of dimples on the cheek is considered to be a symbol of good luck in Chinese culture and is seen as a sign of beauty in Arabian society.1,2 Dimples can be seen to accentuate the smile, which might in turn increase one’s perception of attractiveness, sociability, and facial beauty. Some believe that dimples make a person’s smile more memorable and distinct, associating it with cheerfulness.
Dimples occur in both sexes, with no predominance in either sex.3–6 The occurrence of dimples on the face is an autosomal dominant trait. Cheek dimples are believed to occur on chromosome 16, whereas cleft chin dimples occur on chromosome 5.3
According to a study published by Pessa et al in 1998,7 cheek dimples are caused by dermocutaneous insertion of the fibers on the inferior bundle of the double or bifid zygomaticus major muscle. Smiling makes the overlying skin draw inward, making the dimples larger and more visible. However, in contrast, chin dimples are formed because of an underlying bone defect.8
Facial dimples are located on more mobile tissue.9 They are mainly seen on the cheeks, followed by the regions of the angle of the mouth. They are categorized as those opposite the angle of the mouth (para-angle), those below (lower para-angle) the angle of the mouth, and those above (upper para-angle) the angle of the mouth. Lower para-angle dimple is the most common type of facial dimple.2
Currently, there has been an increased demand worldwide for the surgical creation of facial dimples.1,4,10,11 When surgically creating a dimple, the ideal location would usually be at the site of a pre-existing faint dimple, making it more prominent. If a unilateral dimple is present, the ideal position for the other dimple would usually be marked at the corresponding site on the contralateral side.2
When no pre-existing dimple exists on the patient’s face, the most common point for creation is the Khoo Boo-Chai’s point (KBC point), which lies at the intersection between a horizontal line drawn from the corner of the mouth and a vertical line dropped from the outer canthi of the eye.2
For more than 60 years, the KBC point has been the “gold standard” positioning guide for the surgical creation of the dimples; however, differences in facial shape have not traditionally been taken into consideration when determining the optimal size, shape, and location of surgically created dimples. In this study, we assessed the facial shape of a sample of men and women, all of whom had natural dimples, to determine if characteristic patterns in dimple size, location, and shape existed according to each specific facial form. We hypothesized that certain characteristics of dimples are predominant among certain facial shapes. Understanding these differences could help surgeons achieve optimal outcomes by creating more natural looking and thus more aesthetically pleasing dimples among their patients seeking dimpleplasty.
Materials and Methods
Our study included a randomized convenient sampling of 1,194 people. Two-hundred and sixteen people (18%) with 336 naturally occurring dimples were chosen for the study. Informed consent was obtained from all participants. Photoconsent was obtained from participants featured in this publication. The ethical guidelines of the Declaration of Helsinki were followed.
The ages of the study population ranged from 18 to 42 years. The study was conducted from April 2017 to June 2017. Facial forms and the deepest points of the naturally occurring dimples of the participants were examined. For each patient, the distance between the deepest point of the dimple and the KBC point was calculated. A woolen string coated with plaster of Paris was used to mark a horizontal line from the corner of the mouth and a vertical line from the outer canthi of the eye. The difference between the KBC point (which is at the intersection of the two lines) and the deepest point of the naturally occurring dimples was calculated. Facial forms of the participants were categorized as euryprosopic (short and/or broad face), mesoprosopic (average width face), or leptoprosopic (long and/or narrow face).12 All of the patients were evaluated according to a standard evaluation form (Figure 1) and a single observer.

Results
Out of the 216 people included in this study, all of whom had naturally occurring dimples, 120 (55.6%) had bilateral dimples and 96 (44.4%) had unilateral dimples, for a total of 336 dimples (Table 1). Forty-five (21%) of the 216 participants were male and 171 (79%) were female (Figure 2).


Among the 120 individuals with bilateral dimples, 99 (82.5%) were female and 21 (17.5%) were male. Regarding the 96 participants with unilateral dimples, 72 (75%) were female and 24 (25%) were male. Of the 96 unilateral dimples, 51 (53.1%) were on the right side and 45 (46.9%) were on the left.
We observed that 152 dimples lay on the KBC point (45.2%) and 184 lay elsewhere on the face (54.8%) (Figure 3).

In addition to the KBC point, the number of dimples per different facial form was also assessed. Most of the people included in this study had the mesoprosopic facial form (132 (61.1%), followed by 48 people with the leptoprosopic form (22.2%) and 36 people with the euryprosopic form (16.7%) (Table 2).

In the mesoprosopic group, 60 people had unilateral dimples and 72 had bilateral dimples, for a total of 132 people with 204 dimples. Of these, 117 dimples did not lie on the KBC point and 87 dimples did. In the leptoprosopic group, 30 people had unilateral dimples and 18 people had bilateral dimples, for a total of 48 people with 66 dimples. Thirty of these dimples did not lie on the KBC point and 36 dimples did. In the euryprosopic group, six people had unilateral dimples and 30 had bilateral dimpless, for a total of 36 people with 66 dimples. Of these, 36 dimples did not lie on the KBC point and 30 dimples did (Table 3).

Discussion
Dimple surgery has become a common cosmetic procedure.1,4,10,11 Though the frequency of dimple surgery has increased in recent years, the most commonly used reference point (i.e., the KBC point) for dimple surgery dates back 50 years. In 1962, Khoo Boo-Chai studied the dimples of about 500 female individuals aged between one day and 50 years.2 From his observations, he concluded that the majority of dimples are located at a point of intersection between a perpendicular line dropped from the outer canthi of the eye and a horizontal line drawn out from the angle of the mouth. Over the years, along with the KBC point, surgeons have also used other reference points for creating dimples. For example, Lari,13 in 2012, suggested two methods for determining the site of dimple creation: 1) using the point of intersection of a perpendicular line dropped from the external canthus and a horizontal line drawn from the highest point of the Cupid’s bow and 2) asking patients to suck in their cheeks and then marking the site of maximum depression as the location for the dimple.13
Shaker10 created a dimple by asking the patient to smile and then marking the dimple site 2 to 2.5cm lateral to the nasolabial fold at the same level or slightly above the angle of the mouth.
El-Sabbagh11 suggested creating a dimple at a point that is level with or above the angle of mouth, according to the vector of smile.
For our study, we sought to determine the most natural location of dimples based on the individual’s facial shape to provide guidance to surgeons for achieving optimal outcomes by creating more natural and thus more aesthetically pleasing dimples in their patients seeking dimpleplasty.
Eighteen percent of our total study population had naturally occurring dimples, and among those study subjects, 79.2 percent were female. This significant difference in prevalence of dimples according to sex was not observed in previous literature, in which dimple prevalence was reported as equal between the sexes. Among our study population, we observed a greater number of bilateral dimples, which corresponds with other published findings.11 There was no noted difference in the occurrence of dimples on the right side or left side. However, according to Koo Bhoo-Chai, dimples are predominantly on the left side of the face (60%).2
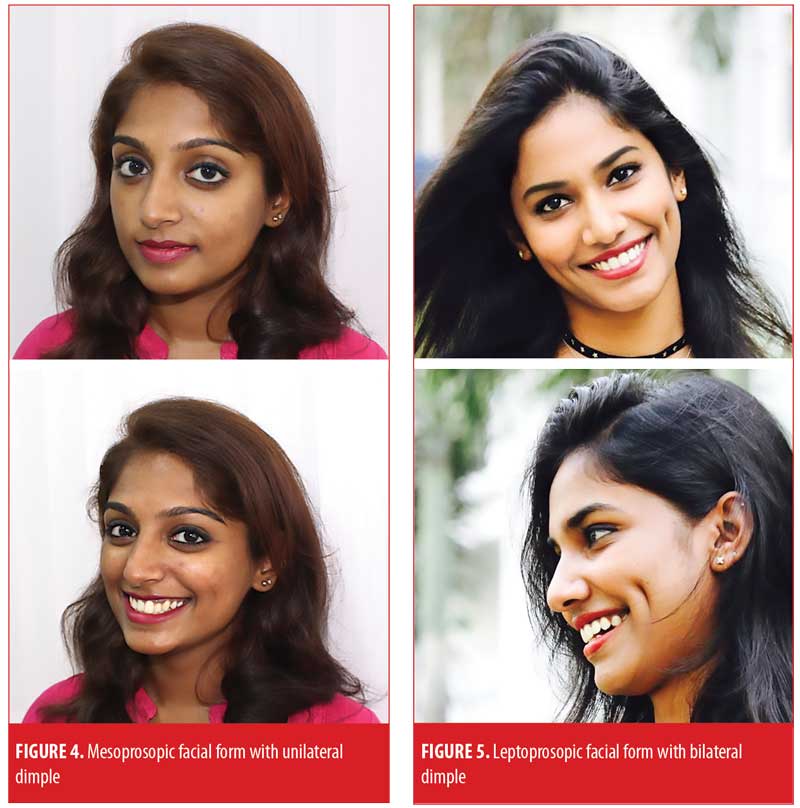
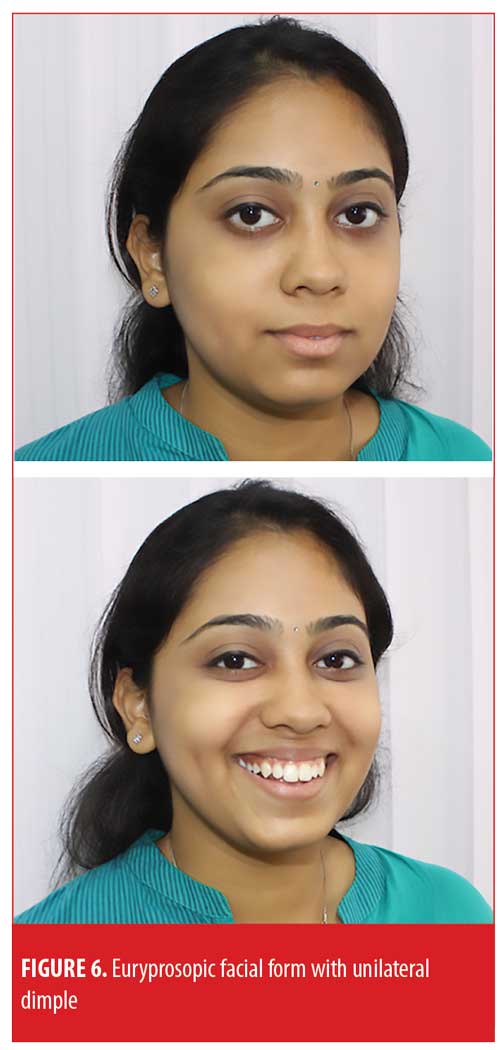
Though many reference points for creating dimples have been used in practice,2,10–13 we were unable to find reports in the existing literature that indicated consideration of an individual’s facial shape when choosing the optimal location for dimples. In our study, we found that the morphology of dimples was analogous to the shape of the individual’s face. We observed a higher prevalence of dimples among the mesoprosopic group, compared to the other two groups, with no unilateral or bilateral predominence (Figure 4). Conversely, we observed a predominance of unilateral dimples in the leptoprosopic group and a predominence of bilateral dimples in the euryprosopic group. The shape of the dimple also varied according to the facial shape—leptoprosopic individuals tended to have long, narrow dimples (Figure 5), while the euryprosopic group tended to have short and circular dimples (Figure 6). The depth of the dimples did not vary significantly between the three groups.
Guidelines for Surgical Creation of Dimples
We offer the following guidelines, based on our observations, for surgeons who perform dimpleplasty (see Figure 7 for an overview of guidelines):
- The sex of the patient does not impact the number or position of dimples.
- The unilateral dimple is predominant among individuals with the leptoprosopic facial shape; thus, this type of dimple is recommended among those with the leptoprosopic shape. For those with the euryprosopic facial shape, bilateral dimples are recommended, and for mesoprosopic individuals, either can be done. When choosing which side of the face to create the dimple, preference should be given to the side with the dominant hand.
- If an existing unilateral dimple is present and the patient would like a dimple on the contralateral side, the dimple should be made at the same level as the existing dimple or at the point of a pre-existing faint dimple.
- For the mesoprosopic facial form, the point of the dimple should be 4mm anterior to the KBC point. The shape of the dimple can be long, short, narrow, or circular. For patients with the leptoprosopic facial form, the dimple should be positioned at the KBC point and ideally should have a long, narrow shape. For a euryprosopic facial form, the dimple should be positioned 3mm above and behind the KBC point or at the level of the Cupid’s bow horizontally, and ideally should be short and circular in shape.
- Ultimately, regardless of facial form, the positioning, size, shape, and number of dimples should be based on each individual patient’s preference. If the patient has no specific requests, then the clinician can use dimple characteristics associated with the patient’s facial form as a guide for determining the optimal position, size, shape, and number of dimple(s).
Conclusion
We have observed certain characteristic patterns in the position, size, shape, and number of dimples among three primary facial shapes: mesoprosopic, leptoprosopic, and euryprosopic. We therefore recommend that, barring specific patient requests, surgeons consider each patient’s facial shape and its associated dimple characteristics as a guide when performing dimpleplasties. This will help ensure an optimal outcome by creating more natural looking and thus more aesthetically pleasing dimples.
References
- Bao S, Zhou C, Li S, Zhao M. A new simple technique for making facial dimples. Aesth Plast Surg. 2007;31(4):380–383.
- Boo-Chai K. The facial dimple—clinical study and operative technique. Plast Reconstr Surg Transplant Bull. 1962;30:281–288.
- Omotoso GO, Adeniyi PA, Medubi LJ. Prevalence of facial dimples amongst South-western Nigerians: a case study of Ilorin, Kwara State of Nigeria. Int J Biomed Sci. 2010;6( 4):241–244.
- Thomas M, Menon H, D’Silva J.
Improved surgical access for facial dimple creation. Aesthet Surg J. 2010;30(6):798–801. - Argamaso RV. Facial dimple: Its formation by a simple technique. Plast Reconstr Surg. 1971;48(1):40–43.
- Pentozos Daponte A, Vienna A, Brant L, Hauser G. Cheek dimples in Greek children and adolescents. Int J Anthropol. 2004;19(4):289–295.
- Pessa JE, Zadoo VP, Garza PA, et al: Double or bifid zygomaticus major muscle: Anatomy, incidence, and clinical correlation. Clin Anat 11:310, 1998
- Keyhan SO, Khiabani K, Hemmat S. Dimple creation surgery technique: a review of the literature and technique note. J Oral Maxillofac 8Surg. 2012;70(6):e403–e407.
- Cummins H. In: Morris’ Human Anatomy. 12th ed. New York, NY: McGraw Hill Book Co.; 1966: 112.
- Shaker AA, Aboelatta YA, Attia KS. A simple technique to create cheek dimples. Ann Plast Surg. 2015;75(5):493–496.
- El-Sabbagh AH. Simple technique for facial dimple. J Cutan Aesthet Surg. 2015;8(2):102–105.
- K. Lakshmi Kumari, P. V. S. S. Vijaya Babu, P. Kusuma Kumari, M. Nagamani. A study of cephalic index and facial index in Visakhapatnam, Andhra Pradesh, India. International Journal of Research in Medical Science. DOI: 10.5455/2320-6012.ijrms20150324
- Lari AR, Panse N. Anatomical basis of dimple creation – a new technique: our experience of 100 cases. Indian J Plast Surg. 2012;45(1):89–93.