J Clin Aesthet Dermatol. 2026;19(7):41–46.
by Sebastian Kosasih, MBBS, BSc (Hons), MRCS; Chrysavgi Mavrokefalou, MUDr; Shahab Shahid, BSc, MBBS, PGCert, MRCS; Naguib El-Muttardi, MD, FRCS(Plast); and Ben Miranda, BSc, MBBS, MRCS, FRCS(Plast), DipHandSurg (BSSH), PhD
All authors are with St. Andrew’s Centre for Plastic Surgery & Burns, Broomfield Hospital, Chelmsford, United Kingdom. Drs. Kosasih, Shahid, and El-Muttardi, and Professor Miranda are additionally with St. Andrew’s Anglia Ruskin (StAAR) Research Group, School of Medicine, Faculty of Health, Education, Medicine, and Social Care, Anglia Ruskin University, Chelmsford, United Kingdom.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
Abstract: Background: The aim of nonmelanoma skin cancer (NMSC) excision is histologic clearance with margins of ≥1 mm, but evidence for close-margin management is scarce. Objective: To compare complete, close, and incomplete excision recurrences. Methods: We performed a retrospective study of a subset of patients who underwent NMSC excision during 2020 to 2021. Lesions were grouped as complete (≥1 mm clearance), close (<1 mm), or incomplete (involved) and recurrence data were collected. Discrete data were analyzed using a χ2 test. Results: There were 421 lesions comprising 194 squamous cell carcinomas (SCCs; 49%) and 227 basal cell carcinomas (BCCs; 51%) included in the analysis. The mean follow-up was 29.3 months (standard deviation: 3.2), and the recurrence rate was 5%. There was a significantly greater risk of recurrence in closely (12%) vs completely (3%) excised SCCs (χ2=4.71; degrees of freedom [df]=1; P=0.03); however, no difference was demonstrated between close (12%) and incompletely (12%) excised SCCs (χ2<0.05; df=1; P=0.98). There was no statistical difference in recurrence rates between completely (1%) and closely (3%) excised BCCs (χ2=1.08; df=1; P=0.30), but a difference was found between closely (3%) and incompletely (16%) excised BCCs (χ2=6.33; df=1; P=0.01). Limitations: Follow-up was <5 years, after which NMSCs may still recur. Conclusion: Our results support the clinical practice of treating closely excised SCCs as incomplete and treating closely excised BCCs as complete, perhaps with a follow-up period, in select cases such as when satisfying patient preference or minimising morbidity due to re-excision. Keywords: Nonmelanoma skin cancer, close excision, recurrence, squamous cell carcinoma, basal cell carcinoma
Introduction
Nonmelanoma skin cancers (NMSCs) include both squamous cell carcinoma (SCC) and basal cell carcinoma (BCC) and represent the most common type of skin cancer in the White population.1 The mainstay of NMSC treatment is surgical excision, including a safety margin surrounding the lesion, with the intent of complete tumor clearance ≥1 mm at both the peripheral and deep margins. Updated British Association of Dermatologists (BAD) guidelines on excision margins were published in 2020 and 2021 for SCCs and BCCs, respectively.2,3 Involved margins are considered incompletely excised and usually require further treatment, unless contraindicated due to patient comorbidity or patient preference. A clearance <1 mm is considered a close margin, and the decision to clinically monitor, re-excise, or undergo an alternative form of therapy (such as radiotherapy or immunotherapy) is a patient-tailored decision based on risk factors and patient preference. This decision is often discussed at multidisciplinary team meetings (MDTs), particularly in the case of SCCs. National audit data suggest that NMSC incomplete excision rates are around 2.3% to 3%.4,5 However, a more recent meta-analysis by Nolan et al6 suggests that incomplete excision rates may be underreported, reporting 11.0% for BCCs and 9.4% for SCCs in a pool of 53,796 patients. Furthermore, ongoing delays and backlogs related to the COVID-19 pandemic are likely to allow for more advanced tumor progression, and with previous studies showing that increasing tumor size is correlated with incomplete excision, it is possible that this incomplete excision rate may worsen.7–9 In either case, close-margin excisions are inconsistently reported and are often included in the complete excision cohort. There is a theoretically higher risk of recurrence with close-margin excisions due to the possibility of malignant cells being missed on microscopic review (ie, a false negative if considered complete).10 Additionally, close excisions may have occurred in the first place due to more aggressive or insidious disease phenotypes such as infiltrative BCCs, which are less easily marked up pre-operatively.11 However, there are also a fair proportion of incompletely excised lesions that show no residual malignancy on re-excision.12 Therefore, it remains unclear as to whether close-margin NMSC excisions should be treated as complete or incomplete, though in our center, close margins are often treated as incomplete and re-excised if possible. This is dependent, however, on anatomical location (eg, wider or deeper excision of close-margin excisions on the midface may result in unacceptable morbidity or cosmesis and may be better treated with an alternative modality such as radiotherapy) and patient factors such as ability to travel to our tertiary center for surgery.
Due to a paucity of literature available regarding the outcomes following close-margin NMSC excision, recurrence rates of such cases remain unclear. The aim of this study is to investigate recurrence rates from a cohort of NMSC incomplete excisions and in particular to compare these rates between incomplete, closely, and completely excised lesions.
Methods
Clinical governance approval was granted prior to commencing the study (CA21-089).
This cohort study was based on a subset of data used in a previous study conducted at our institution.13 In the previous study, we identified patients who underwent standard surgical excision for NMSC (both SCCs and BCCs) at our tertiary plastic surgery center hub site (our center operates at multiple sites in a hub-and-spoke model, serving a population of approximately 3.2 million)14 over 1 year from April 1, 2020, to March 31, 2021. Cases were therefore included in the study after being identified at our National Health Service trust via a computerized operative theater database. Our center practice generally treats close-excision margins as incomplete, especially in the case of SCC. For closely excised SCCs, re-excision or alternative therapy (eg, immunotherapy) are offered, though sometimes patients will be monitored only due to patient preference or other factors such as multiple comorbidities. Closely excised patients with BCCs are offered re-excision, radiotherapy, or clinical monitoring. Mohs surgery is sometimes offered to these patients, but due to difficulty of access at our centre, this is often declined by patients. Our aim was to examine recurrence rates in these lesion excisions. Therefore, for comparison, we obtained data for similarly sized cohorts of completely, closely, and incompletely excised SCCs and BCCs from the previous study.13
Data collected included age, gender, comorbidities, operation date, anatomical site, histologic type, margins, recurrence, follow-up time, and further re-excisions. For individuals with multiple lesions, each lesion was treated as a discrete data point. Regarding margins, a tumor excised by ≥1 mm was considered complete, <1 mm as close, and involved margins incomplete. Patients without follow-up data due to being followed up at other sites in the trust or with other specialties were excluded from the study.
In order to analyze if closely excised lesions should be treated as completely or incompletely excised, statistical analysis was performed using Microsoft Excel for Office 365 (Microsoft Corporation) for a χ2 test to examine if the proportion of recurrences was statistically similar between close and complete excisions, between close and incomplete excisions, and finally between complete and incomplete excisions (with the null hypothesis of no difference in recurrence between the groups). The χ2 statistic, degrees of freedom (df), and P values for the χ2 test are reported. Significance was set to P<0.05.
Results
We identified a pool of 468 NMSC lesions that had been excised; 47 lesions that were followed up externally at other sites or lacked follow-up data were excluded, leaving 421 lesions for analysis in 380 patients (247 male, 133 female) with median age of 81 years (interquartile range [IQR]: 75–87). The lesions comprised 194 SCCs (49%, 194/421) and 227 BCCs (51%, 227/421), and 85% (357/421) were located on the head and neck. Mean follow-up time for high-risk monitored lesions was 29.3 months (SD: 3.2; range: 18.1–38.2 months), while mean follow-up times for low-risk lesions discharged at first follow-up was 2.3 months (SD: 3.3; range: 0.3–25.3 months).
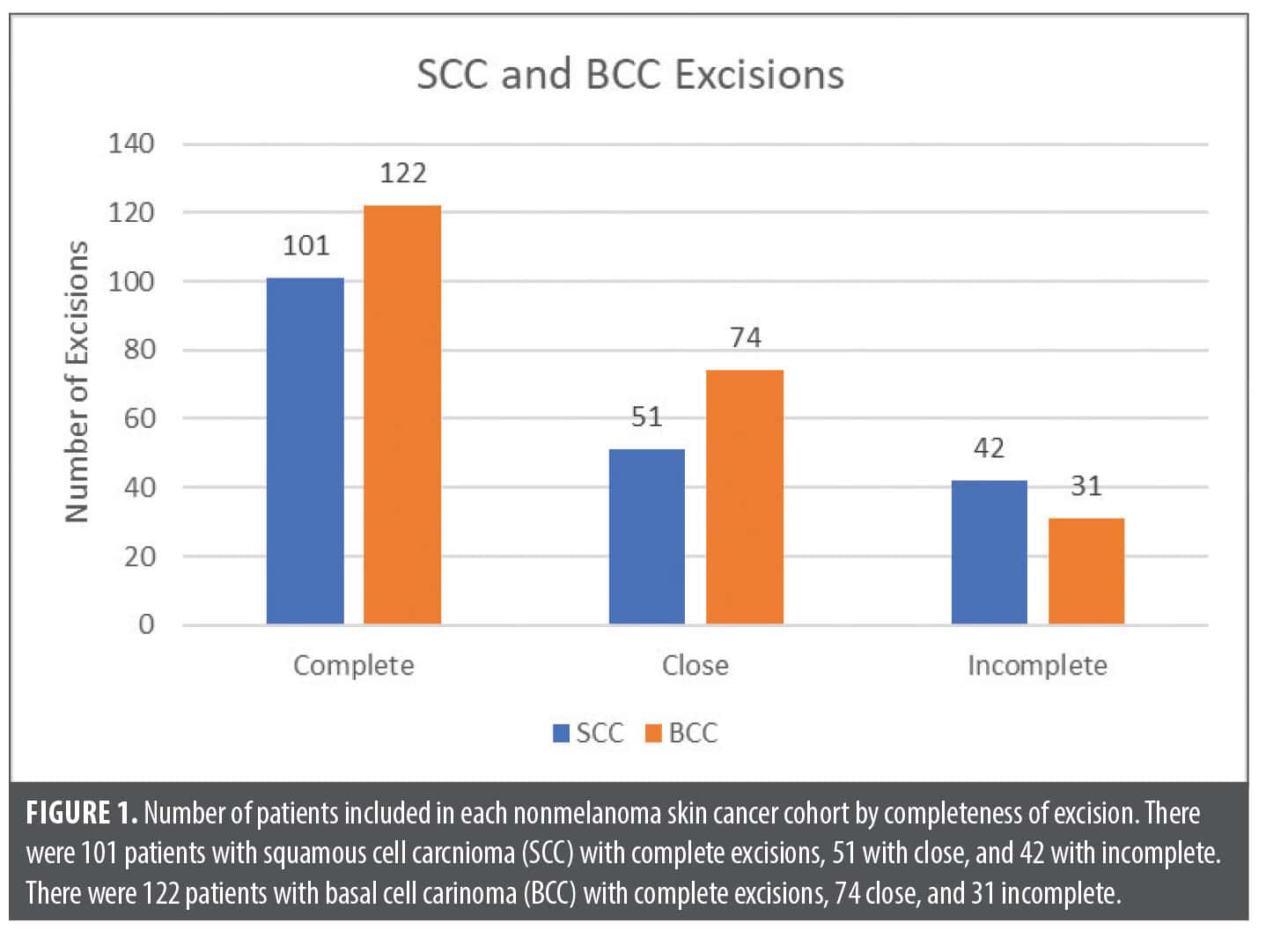
The selected SCC group (n=194) comprised 52% (101/194) complete excisions, 26% (51/194) close excisions, and 22% (42/194) incomplete excisions. In the selected BCC group (n=227), there were 54% (122/227) complete excisions, 32% (74/227) close, and 14% (31/227) incomplete (Figure 1).
In the closely excised SCC group, 14% (7/51) were planned for re-excision at first follow-up. Regarding anatomical site, 92% (47/51) of close excisions were in the head and neck region vs 8% (4/51) in the lower-risk anatomical sites of the limbs.
In the closely excised BCC group (n=74), only 1 was planned for re-excision at first follow-up; 93% (69/74) of close excisions were in the head and neck region vs 7% (5/74) in the lower-risk areas of the trunk or limbs.
The overall NMSC recurrence rate was 5% (22/421), with 64% (14/22) of recurrences being SCCs (3 from completely excised lesions, 6 from closely excised, and 5 from incomplete excisions) and 36% (8/22) being BCCs (1 from a completely excised lesion, 2 from closely excised, and 5 from incomplete excisions). Therefore, the SCC close-excision recurrence rate was 12% (6/51) and the BCC close-excision recurrence rate was 3% (2/74). Overall, 91% (20/22) of recurrences were in lesions from the head and neck, with the remaining 9% (2/22) from the forearm and chest. Of the recurrent lesions that were closely or incompletely excised at initial histology (n=18), only 1 patient (6%, 1/18) was referred for radiotherapy with an incompletely excised SCC; the other 94% (17/18) either listed for re-excision or monitored if not suitable for re-excision. One patient (25%, 1/4) of the completely excised lesions that recurred had additionally developed multiple new SCCs at follow-up and was referred for immunotherapy. Median time to recurrence was 5.7 months (range: 1.8–23.2; IQR: 4.4–8.1). Further recurrence data are presented in Table 1.
On χ2 testing, when comparing the recurrence rates between the completely excised (3%, 3/101) and closely excised (12%, 6/51) SCCs, the chance of recurrence was statistically different (χ2=4.71; df=1; P=0.03). However, when comparing recurrence rates in the close (12%, 6/52) and incomplete (12%, 5/42) SCC groups, there was no difference (χ2<0.05; df=1; P=0.98). As expected, there was a statistically significant difference between the complete (3%, 3/101) and incomplete (12%, 5/42) excision groups (χ2 =4.48; df=1; P=0.03).
For BCCs, in the completely (1%, 1/122) vs closely (3%, 2/74) excised groups, there was no statistical difference in recurrence rates (χ2=1.08; df=1; P=0.30). Looking at the closely (3%, 2/74) and incompletely (16%, 5/31) excised groups, there was a statistical difference in recurrence (χ2=6.33; df=1; P=0.01). Once again, recurrence rates in completely (1%, 1/122) vs incompletely (16%, 5/31) excised BCCs were statistically different (χ2 =15.48; df=1; P<0.01).
Discussion
This study builds upon previous work by our team, which highlighted the need for clarity on whether close excisions should be considered complete or incomplete.13 Our main findings are that regarding recurrence, closely excised SCCs recur in a manner similar to incompletely excised tumors whereas for BCCs, closely excised lesions appear to behave more similarly to completely excised tumors. The logical conclusion is that closely excised SCCs should be managed with further treatment (re-excision, Mohs surgery, or radiotherapy) or at least discussion in an MDT as for incompletely excised SCCs. This lends some evidence to the most recent iteration of the British Association of Dermatologists guidelines for SCCs, which suggest managing closely excised lesions similarly to incompletely excised tumors, though they report there is little strong evidence to support this practice.2 Conversely, as closely excised BCCs have recurrence rates statistically similar to completely excised BCCs, we may be able to treat these more conservatively, as wider or deeper re-excisions, particularly in cosmetically sensitive areas such as the nose and eyelids, may be associated with higher morbidity and impairments to social functioning for some patients.15 To our knowledge, there is a paucity of literature regarding the best treatment options for closely excised lesions, which has also contributed to the inconsistently reported nature of close margins, with some authors considering these completely excised,16–27 while others consider them incomplete.28–32 Therefore, the results of our study offer some evidence toward the ongoing debate of best practice for closely excised lesions.
In our selected cohort of patients, there were 42 incompletely excised SCCs from the total 194 SCCs (22%) in the dataset and 31 incompletely excised BCCs from the total of 227 (13%). Due to the study design (looking for recurrences in cohorts matched to the incomplete and close excisions), this is not a proportion of total NMSCs excised over the study period. The total incomplete excision rate in our previous study was 6.6% for SCC rate and 3.2% for BCC, from a total pool of 2,554 NMSC excisions, which is in line with other studies in the literature.6,13 Head and neck lesions are known to confer a high risk of incomplete excision, partly due to a difficult balance between oncologic control and functional or cosmetic concerns.33,34
Interestingly, in the time since our study cohort of patients received surgery, the British Association of Dermatologists guidance for standardized excision margins has been updated, with suggested peripheral-excision margins for low-risk BCCs increasing from 3 mm to 4 mm, the same as for low-risk SCCs.2,3 Therefore, it is possible that newer populations of patients with BCCwith excisions based on the updated guidelines may have an even lower rate of close or incomplete margins; this should be investigated in the future to clarify the merits of a wider excision, particularly in cosmetically sensitive areas.
As a final point, with regards to re-operation, one might argue that closely excised lesions are an ideal case use for Mohs surgery given ability for immediate margin control. However, there is large variability in availability of Mohs surgeons worldwide, with countries such as the United States having far greater access than some European countries. Therefore, this study offers most benefit to areas in which there are fewer Mohs services and treatment of closely excised lesions is more of a dilemma.
Limitations of this study include the lack of data on lesion size or intra-operative margins (peripheral or deep plane) and, for close-margin excisions, our histologic data were limited in some cases as reports only mentioned a margin <1 mm but not the specific measurement. Follow-up is also <5 years, a period in which NMSCs may still recur. While continuous data on closeness of excision were not required for our current study, future work using regression analysis could investigate closeness of excision with recurrence as well as the differences in recurrence rates between close-peripheral and close-deep margins. Finally, given that we had a high caseload of head and neck cases, these results may not be entirely generalizable to a general lower-risk population.
Conclusion
Our study demonstrated that closely excised SCCs recur as frequently as incompletely excised lesions, while closely excised BCCs have a similar recurrence pattern to completely excised lesions. In this area where there is a paucity of literature and ongoing debate, our results provide some support to the clinical practice of treating closely excised SCCs as incomplete and to consider treating closely excised BCCs as complete, perhaps with a period of follow-up, which may help to decrease the excess morbidity caused by wider re-excision.
Acknowledgements
The authors would like to thank the Plastic Surgery Department at St. Andrew’s Centre for Plastic Surgery and Burns for their assistance and support with the preparation of this study.
References
- Samarasinghe V, Madan V. Nonmelanoma skin cancer. J Cutan Aesthet Surg. 2012;5(1):3–10.
- Keohane SG, Botting J, Budny PG, et al; British Association of Dermatologists’ Clinical Standards Unit. British Association of Dermatologists guidelines for the management of people with cutaneous squamous cell carcinoma 2020. Br J Dermatol. 2021;184(3):401–414.
- Nasr I, McGrath EJ, Harwood CA, et al; British Association of Dermatologists’ Clinical Standards Unit. British Association of Dermatologists guidelines for the management of adults with basal cell carcinoma 2021. Br J Dermatol. 2021;185(5):899–920.
- Keith DJ, de Berker DAR, Bray AP, Cheung ST, Brain A, Mohd Mustapa MF. British Association of Dermatologists’ national audit on nonmelanoma skin cancer excision, 2014. Clin Exp Dermatol. 2017;42(1):46–53.
- Keith DJ, Bray AP, Brain A, et al. British Association of Dermatologists (BAD) national audit on non-melanoma skin cancer excision 2016 in collaboration with the Royal College of Pathologists. Clin Exp Dermatol. 2020;45(1):48–55.
- Nolan GS, Kiely AL, Totty JP, et al. Incomplete surgical excision of keratinocyte skin cancers: a systematic review and meta-analysis. Br J Dermatol. 2021;184(6):1033–1044.
- Mavrokefalou C, Corriero AC, Shahid S, Miranda BH. A study of the effects of pre-operative cutaneous BCC duration on tumour progression. J Plast Reconstr Aesthetic Surg. 2022;75(8):2831–2870.
- Shahid S, Gao J, Corriero AC, Roszpopa J, Miranda BH. A study of the effects of delayed patient presentation on cutaneous SCC progression. J Plast Reconstr Aesthetic Surg. 2022;75(2):722–729.
- Svensson H, Paoli J. Clinicopathological factors associated with incomplete excision of cutaneous squamous cell carcinoma. Acta Derm Venereol. 2020;100(13):adv00188.
- Mackiewicz-Wysocka M, Bowszyc-Dmochowska M, Strzelecka-Węklar D, Dańczak-Pazdrowska A, Adamski Z. Basal cell carcinoma – diagnosis. Contemp Oncol (Pozn). 2013;17(4):337–342.
- Pampena R, Parisi G, Benati M, et al. Clinical and dermoscopic factors for the identification of aggressive histologic subtypes of basal cell carcinoma. Front Oncol. 2020;10:630458.
- Swetter SM, Boldrick JC, Pierre P, Wong P, Egbert BM. Effects of biopsy-induced wound healing on residual basal cell and squamous cell carcinomas: rate of tumor regression in excisional specimens. J Cutan Pathol. 2003;30(2):139–146.
- Mavrokefalou C, Katechia D, Kosasih S, Miranda BH. Close and incomplete excision margins in non-melanoma skin cancer: a tertiary plastic surgery center experience. J Plast Reconstr Aesthet Surg. 2023;79:36–38.
- St Andrew’s Centre for Plastic Surgery and Burns. Mid and South Essex NHS Foundation Trust. Accessed 14 Mar 2023. https://www.mse.nhs.uk/plastic-surgery-and-burns
- Lee EH, Klassen AF, Lawson JL, Cano SJ, Scott AM, Pusic AL. Patient experiences and outcomes following facial skin cancer surgery: a qualitative study. Australas J Dermatol. 2016;57(3):e100–e104.
- Wong KY, Gilleard O, Price RD. Are non-melanoma skin cancer incomplete excision rates different between grades of plastic surgeons? J Plast Reconstr Aesthet Surg. 2013;66:e146–148.
- Riml S, Larcher L, Kompatscher P. Complete excision of nonmelanotic skin cancer: a matter of surgical experience. Ann Plast Surg. 2013;70:66–69.
- Mourouzis C, Boynton A, Grant J, et al. Cutaneous head and neck SCCs and risk of nodal metastasis – UK experience. J Craniomaxillofac Surg. 2009;37:443–447.
- Pua VSC, Huilgol S, Hill D. Evaluation of the treatment of non-melanoma skin cancers by surgical excision. Australas J Dermatol. 2009;50:171–5.
- Delaney EK, Duckworth L, Thompson WD, et al. Excising squamous cell carcinomas: comparing the performance of GPs, hospital skin specialists and other hospital specialists. Fam Pract. 2012;29:541–546.
- Bhatti AZ, Asif S, Alwan M. Factors affecting incomplete excision of nonmelanoma skin cancers in New Zealand. Ann Plast Surg. 2006;57:513–516.
- Mirshams M, Razzaghi M, Noormohammadpour P, et al. Incidence of incomplete excision in surgically treated cutaneous squamous cell carcinoma and identification of the related risk factors. Acta Med Iran. 2011;49:806–809.
- Tan P-Y, Ek E, Su S, et al. Incomplete excision of squamous cell carcinoma of the skin: a prospective observational study. Plast Reconstr Surg. 2007;120:910–916.
- Haisma MS, Plaat BEC, Bijl HP, et al. Multivariate analysis of potential risk factors for lymph node metastasis in patients with cutaneous squamous cell carcinoma of the head and neck. J Am Acad Dermatol. 2016;75:722–730.
- Bogdanov-Berezovsky A, Cohen AD, Glesinger R, et al. Risk factors for incomplete excision of squamous cell carcinomas. J Dermatolog Treat. 2005;16:341–344.
- Stewart TJ, Saunders A. Risk factors for positive margins after wide local excision of cutaneous squamous cell carcinoma. J Dermatolog Treat. 2018;29:706–708.
- Rubino C, Soggiu D, Farace F, et al. Treatment of non-melanoma skin cancer in North Sardinia: is there a need for biopsy? Acta Chir Plast. 2004;46:110–114.
- Bovill ES, Cullen KW, Barrett W, et al. Clinical and histological findings in re-excision of incompletely excised cutaneous squamous cell carcinoma. J Plast Reconstr Aesthet Surg. 2009;62:457–461.
- Ang P, Tan AWH, Goh CL. Comparison of completely versus incompletely excised cutaneous squamous cell carcinomas. Ann Acad Med Singap. 2004;33:68–70.
- Seretis K, Thomaidis V, Karpouzis A, et al. Epidemiology of surgical treatment of nonmelanoma skin cancer of the head and neck in Greece. Dermatol Surg. 2010;36:15–22.
- Brinkman JN, Hajder E, van der Holt B, et al. The effect of differentiation grade of cutaneous squamous cell carcinoma on excision margins, local recurrence, metastasis, and patient survival: a retrospective follow-up study. Ann Plast Surg. 2015;75:323–326.
- Genders RE, Marsidi N, Michi M, et al. Incomplete excision of cutaneous squamous cell carcinoma; systematic review of the literature. Acta Derm Venereol. 2020;100(6):adv00084.
- Hansen C, Wilkinson D, Hansen M, Soyer HP. Factors contributing to incomplete excision of nonmelanoma skin cancer by Australian general practitioners. Arch Dermatol. 2009;145(11):1253–1260.
- Nolan GS, Dunne JA, Lee AE, et al. National audit of non-melanoma skin cancer excisions performed by plastic surgery in the UK. Br J Surg. 2022;109(11):1040–1043.