J Clin Aesthet Dermatol. 2026;19(7):47–51.
by Aaron Cheng, BA, BS; Katelyn Cornelius, MD; David Cotter, MD, PhD; Thuy L. Phung, MD, PhD; Rodrigo Valdes Rodriguez, MD; Emily M. Becker, MD; Katie Wiggins-Dohlvik, MD; Richard Thomson, MD; and Aaron Sugalski, DO
Mr. Cheng is with the Long School of Medicine, University of Texas Health San Antonio, San Antonio, Texas. Dr. Cornelius is with the Florida State University College of Medicine, Tallahassee, Florida. Dr. Cotter is with Las Vegas Dermatology and the University of Nevada Las Vegas School of Medicine, Las Vegas, Nevada. Dr. Phung is with the Long School of Medicine, University of Texas Health San Antonio, and the Department of Pathology and Laboratory Medicine, Division of Dermatology and Cutaneous Surgery, University of Texas Health San Antonio, San Antonio, Texas. Dr. Valdes Rodriguez is with the Department of Pathology and Laboratory Medicine, Division of Dermatology and Cutaneous Surgery, University of Texas Health San Antonio, San Antonio, Texas. Dr. Becker is with the Department of Medicine, Division of Dermatology, University of Texas Health San Antonio, San Antonio, Texas. Dr. Wiggins-Dohlvik is with the Department of Surgery, Division of Pediatric Surgery, University of Texas Health San Antonio, San Antonio, Texas. Dr. Thomson is with the Department of Surgery, Division of Plastic Surgery, University of Texas Health San Antonio, San Antonio, Texas. Dr. Sugalski is with the Department of Pediatrics, Division of Pediatric Hematology-Oncology, University of Texas Health San Antonio, San Antonio, Texas.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
Abstract: In this article, we describe 3 distinct subtypes of pediatric melanoma with atypical clinical features and unique molecular testing, suggesting de novo tumor development, treated surgically. Keywords: Melanoma, pediatrics, oncodermatology
Introduction
Pediatric melanoma, while exceedingly rare, is the most commonly diagnosed skin cancer in children, with an average of 300 to 500 new diagnoses annually.1 Historically, the annual incidence has increased by an average of 2.8% per year, making it one of the faster growing pediatric neoplasms.2 However, recent studies show a decline in pediatric melanoma incidence, though it remains a serious clinical concern.3 The prognosis of pediatric melanoma, as in adults, depends on several factors, including the Breslow depth, ulceration status, mitotic rate, and presence or absence of lymphovascular invasion.2–4 Wide local excision (WLE) is the mainstay of treatment but may be combined with sentinel lymph node biopsy (SLNB) and/or neoadjuvant or adjuvant medical therapy depending on tumor stage.
Clinical characteristics of melanoma often differ significantly in the pediatric population, with many lacking the typical “ABCDE” detection criteria of asymmetry, border irregularity, color variation, diameter >6 mm, and/or evolution.5 The most common pediatric melanoma characteristics are amelanosis, bleeding, and “bumps” with uniform color that are often mistaken for benign skin lesions.5,6 Combined with the rarity of the disease itself, diagnostic delays and misclassifications delay appropriate treatment and complicate efforts to establish robust pediatric-specific guidelines.
In this article, we describe 3 distinct subtypes of pediatric melanoma with atypical clinical features and unique molecular testing, suggesting de novo tumor development, treated surgically.
Case 1
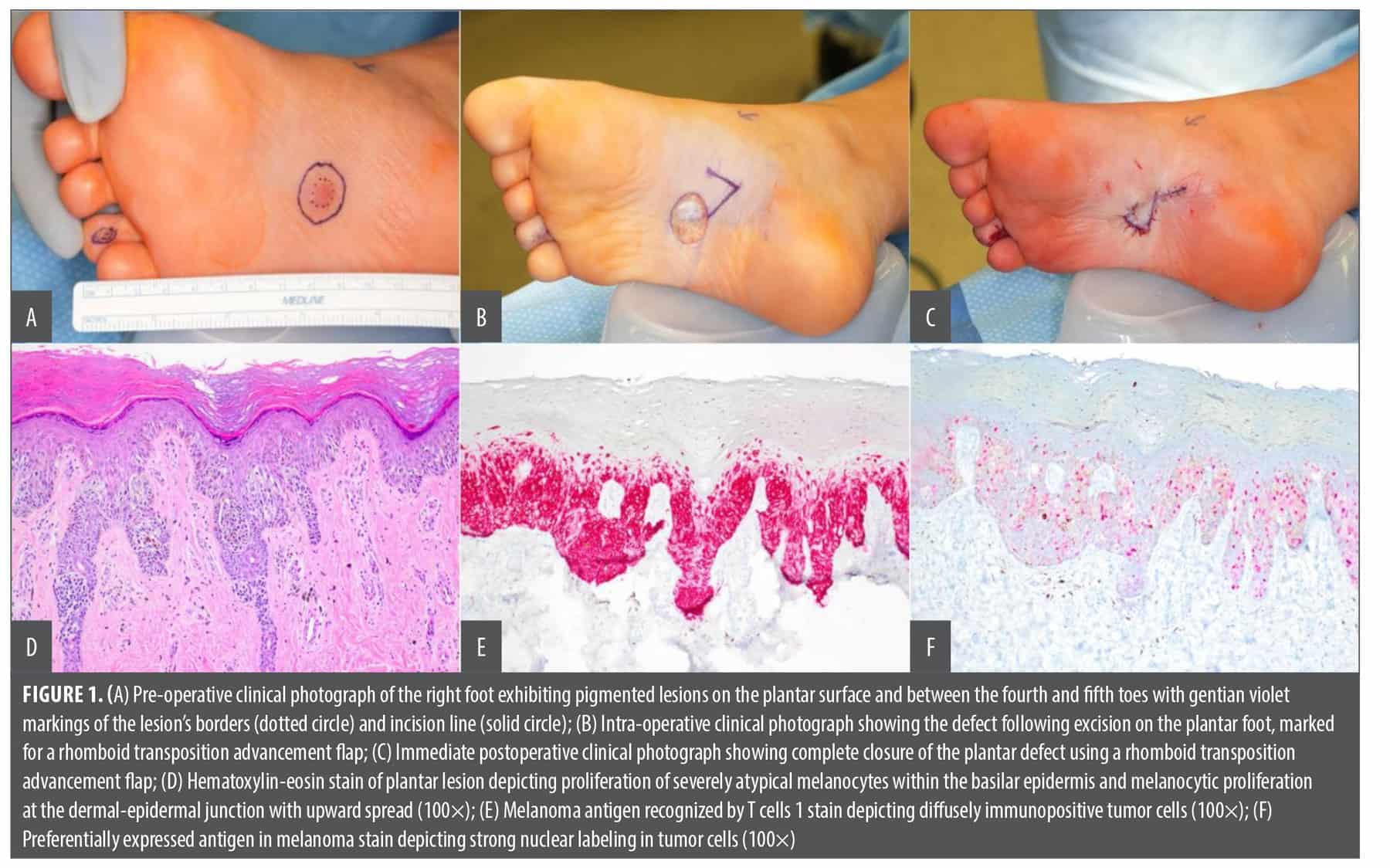
A previously healthy 11-year-old girl presented for evaluation of 2 pigmented lesions on the right plantar foot and right fourth toe (Figure 1A). Additional intraoperative images are shown in Figure 1B and Figure 1C. The lesion on her right plantar foot, present since age 2, had undergone gradual, consistent growth and darkening over the past few years. Shave biopsies of the lesions were obtained by the referring community dermatologists, after which the patient was transferred to our institution for further evaluation and care. The right plantar foot lesion showed proliferation of severely atypical melanocytes within the basilar epidermis and melanocytic proliferation at the dermal-epidermal junction, with upward spread consistent with early malignant melanoma in situ (MMIS; Figure 1D), and the right fourth toe lesion was diagnosed as an acral type compound melanocytic nevus with severe atypia. This MMIS was immunoreactive for melanoma antigen recognized by T cells 1 (MART-1) and preferentially expressed antigen in melanoma (PRAME; Figure 1E, Figure 1F). The shave biopsy of the lesion on the right fourth toe showed proliferation of nested and single melanocytes, demonstrating moderate-to-severe cellular atypia at the dermal-epidermal junction and focally within the dermis consistent with an acral type compound melanocytic nevus. This lesion was MART-1 positive and PRAME negative. Both lesions were completely excised with WLE performed under general anesthesia, with final surgical pathology showing no residual tumor. The patient remains disease free and continues to be followed by a multidisciplinary team to monitor for disease recurrence.
Case 2
A previously healthy 15-year-old girl presented to podiatry for evaluation of a brownish-black right great toenail (Figure 2A). Over several years, the lesion widened from a linear hyperpigmented streak across her nail plate, initially thought to be a splinter, to a blackened nail bed and nail plate with proximal ulceration with granulation tissue.The nail was removed, and a darkened portion was sent for pathology, which showed no signs of malignancy. The nail subsequently regrew darker and more brittle with onycholysis and erythema of the surrounding skin. Punch biopsy through the nail plate showed severely atypical melanocytes with pleomorphic and hyperchromatic nuclei within the dermis, which extended to the peripheral edges and base of the specimen to a depth of at least 0.9 mm, consistent with an ulcerated subungual melanoma. Additionally, positive MART-1 and PRAME staining confirmed melanocytic origin. Complete surgical excision of the lesion, underlying nail bed, and germinal matrix was performed under general anesthesia (Figure 2B). Surgical pathology showed severely atypical melanocytes along the nail bed epithelium arranged in nests and solitary melanocytes demonstrating confluent growth with pagetoid spread and a residual depth of 0.4 mm (Figure 2C). SOX10 and MART-1 immunostaining were positive, further confirming melanocytic origin (Figure 2D, Figure 2E). Ultimately, the patient underwent amputation of the right great toe at the interphalangeal joint and SLNB under general anesthesia. The SLNB was negative and final surgical pathology showed no residual tumor. The patient continues to show no evidence of disease and is being monitored by a multidisciplinary team for any signs of recurrence.

Case 3
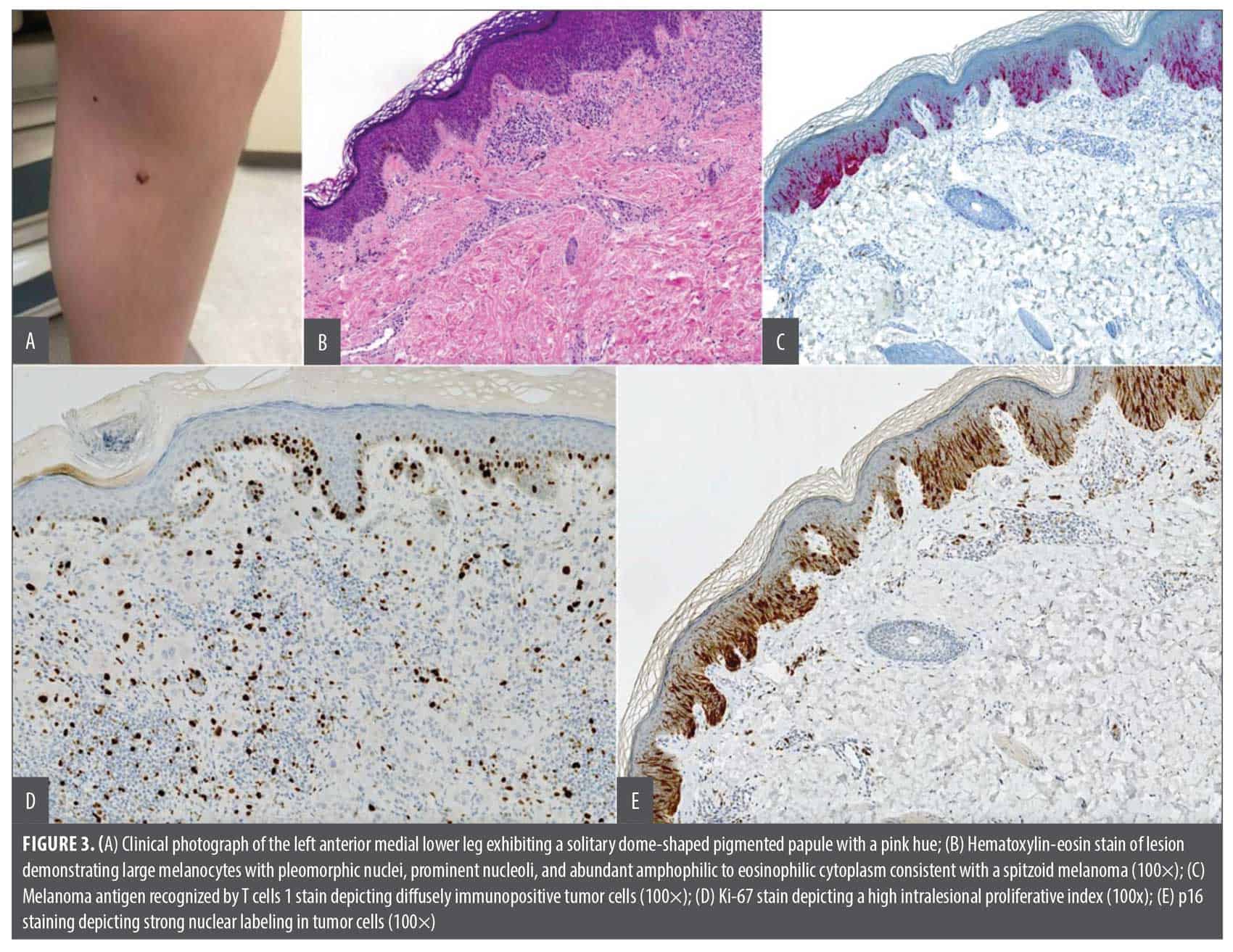
An 11-year-old boy presented to the clinic with a solitary, dome-shaped, pigmented papule on the left anterior medial lower leg (Figure 3A). The lesion arose at 4 years of age; however, over the course of several months, it had elevated and developed a pink hue, prompting referral for evaluation. Punch biopsy showed large melanocytes with pleomorphic nuclei, prominent nucleoli, and abundant amphophilic to eosinophilic cytoplasm consistent with a spitzoid melanoma (Figure 3B). Pathologic staging showed a maximal tumor thickness of 1.1 mm, without ulceration, and a mitotic rate of 1/mm2. Additionally, MART-1, p16, and Ki-67 staining were positive, confirming melanocytic origin with a high proliferative index (Figure 3C, Figure 3D, Figure 3E). Multiplex morphometric melanoma fluorescence in situ hybridization (FISH) analysis revealed a markedly abnormal CDKN2A locus, further supporting the diagnosis. The patient underwent WLE and SLNB of the melanoma under general anesthesia. Final surgical pathology showed no residual tumor and a negative sentinel lymph node. The patient remains disease free and continues to receive multidisciplinary follow-up care to monitor for recurrence.
Discussion
Pediatric melanoma is an exceedingly rare but impactful malignancy, accounting for approximately 1% to 4% of all melanoma cases and 1% to 3% of pediatric cancers.7 While historically considered to be increasing in incidence at an annual rate of 2%, more recent data suggest that this trend may have reversed.8,9 A large cohort study using data from the National Childhood Cancer Registry found a significant decline in incidence rates for patients younger than 20 years beginning in 2014.3 The observed decrease may reflect increased public awareness around sun protection, reduced indoor tanning among adolescents, or earlier detection of atypical lesions.10 However, despite these encouraging trends, pediatric melanoma remains a potentially lethal disease that often presents in atypical clinical patterns, leading to delayed diagnosis and worse outcomes.
Of the 3 cases presented, each represents a distinct and exceptionally rare subtype of pediatric melanoma. The first case—a MMIS on the plantar surface of the right foot—is extremely uncommon in the pediatric population. Notably, the location of the lesion itself was highly unusual and could have contributed to initial misclassification, as acral lesions in children are far more likely to be benign. A high clinical suspicion for malignancy and early multidisciplinary collaboration were critical in achieving prompt diagnosis and treatment in this case.
The second case involved a pediatric subungual melanoma that further showed how pediatric melanomas can masquerade as benign disease. Subungual melanomas are exceptionally uncommon, especially in children, and are often misdiagnosed as benign lesions, such as striate melanonychia, onychomycosis, or even as a subungual hematoma, often leading to delayed diagnosis. Unfortunately, in this case, the lesion’s progressive pigmentation and nail dystrophy were initially attributed to benign causes. Definitive diagnosis was made only after the nail regrew with an irregular appearance that prompted further workup. Unfortunately, interphalangeal amputation was required to achieve complete local disease control. Although amputation is particularly challenging in a pediatric patient given the functional and cosmetic concerns, it was necessary in this case to ensure complete extirpation of the tumor.
Finally, the third case highlights the diagnostic gray zone unique to pediatric spitzoid melanomas. Clinically, atypical spitzoid tumors can mimic benign Spitz nevi due to overlapping histopathologic features and presentations.11 Despite their sometimes indolent behavior, spitzoid-type melanomas have documented metastatic capability, making early detection and treatment essential.12 In our case, multiplex FISH assisted in the diagnosis and WLE provided definitive treatment. The patient continues to do well with no evidence of recurrence. These cases collectively demonstrate the clinical and biologic diversity seen in pediatric melanoma. On a larger scale, this variability is reflected in epidemiologic patterns observed across pediatric populations.
Interestingly, despite the rarity of pediatric melanoma, distinct incidence patterns have emerged. Rates are highest among non-Hispanic White adolescents, especially girls, increasing with age and peaking in mid-to-late adolescence.3 Anatomic distribution varies by age and sex; girls more often present with lower extremity lesions, while trunk involvement is more common in adolescent boys.7 Recent geographic analyses reveal that patients in the southern United States and patients exposed to higher UV indices are more likely to present with advanced-stage disease, despite no significant regional differences in overall incidence or mortality.3 These findings suggest that environmental exposures may affect disease severity at presentation.
In addition to environmental influences, genetic factors contribute to the biological and clinical complexity of pediatric melanomas. High-penetrance germline mutations such as CDKN2A or CDK4 are infrequently identified in children.11 Pellegrini et al12 found CDKN2A pathogenic variants in only 9% of pediatric patients. However, moderate-risk variants, especially in the MC1R gene, are common. MC1R variants were identified in over two-thirds of patients in 1 cohort and more than 40% of patients with spitzoid melanomas in another.11,12 Importantly, UV damage–associated mutational signatures (SBS7 and DBS1) were detected in more than 80% of tumors studied, further implicating environmental exposure as a key factor in disease pathogenesis.11
Despite these advances in understanding, there remains a lack of pediatric-specific clinical guidelines for melanoma. Current treatment algorithms are largely extrapolated from adult populations, despite well-established differences in histopathology, clinical behavior, and prognosis.13 Pediatric melanomas are more often nodular, epithelioid, or spindle cell tumors, and sentinel lymph node positivity is more common in children compared to adults.6,8
For our cases, we followed the most current National Comprehensive Cancer Network melanoma guidelines. However, without pediatric-specific diagnostic criteria and standardized treatment recommendations, diagnostic delays and variations in care are frequent. This highlights the need for prospective pediatric studies and tailored guidelines that account for the unique biology and clinical presentation of melanoma in the pediatric population. The 3 cases presented in this series showcase the clinical heterogeneity and diagnostic complexity observed in pediatric melanoma. Each case demonstrated unique clinical features and atypical growth patterns as compared to the adult population. Lesion morphology and behavior also varied across all 3 cases, further complicating diagnosis and reinforcing the need for individualized assessment and tailored surgical management.
As the molecular and clinical understanding of pediatric melanoma advances, opportunities to improve early detection and treatment are emerging. Until pediatric-specific guidelines exist, clinicians must remain vigilant for atypical lesions in high-risk populations to avoid delays and enhance outcomes.
References
- Tracy ET, Aldrink JH. Pediatric melanoma. Semin Pediatr Surg. 2016;25(5):290–298.
- Hawryluk EB, Liang MG. Pediatric melanoma, moles, and sun safety. Pediatr Clin North Am. 2014;61(2):279–291.
- Ituarte BE, Taylor MA, Thomas SI, et al. Clinical presentations and decreasing incidence of melanoma in pediatric and adolescent and young adult patients: 76,108 cases from a nationally representative cohort. J Am Acad Dermatol. 2025;92(3):511–519.
- Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27(36):6199–6206.
- Cordoro KM, Gupta D, Frieden IJ, McCalmont T, Kashani-Sabet M. Pediatric melanoma: results of a large cohort study and proposal for modified ABCD detection criteria for children. J Am Acad Dermatol. 2013;68(6):913–925.
- Mitkov M, Chrest M, Diehl NN, Heckman MG, Tollefson M, Jambusaria-Pahlajani Al. Pediatric melanomas often mimic benign skin lesions: a retrospective study. J Am Acad Dermatol. 2016;75(4):706–711.e4.
- Yousif R, Boull C, Gerami P, Nardone B, Vivar KL, Liszewski W. THE demographics and trends in pediatric melanoma in the United States: an analysis of the National Cancer Database. Pediatr Dermatol. 2021;38(5):1191–1197.
- Wong JR, Harris JK, Rodriguez-Galindo C, Johnson KJ. Incidence of childhood and adolescent melanoma in the United States: 1973–2009. Pediatrics. 2013;131(5):846–854.
- Borad A, Deianni E, Peña K, Burjonrappa S. Pediatric melanoma: geographic trends in incidence, stage, and mortality in the United States. J Surg Res. 2023;290:215–220.
- Swetter SM, Tsao H, Bichakjian CK, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019;80(1):208–250.
- Liebmann A, Admard J, Armeanu-Ebinger S, et al. UV-radiation and MC1R germline mutations are risk factors for the development of conventional and spitzoid melanomas in children and adolescents. EBioMedicine. 2023;96:104797.
- Pellegrini C, Raimondi S, Di Nardo L, et al. Melanoma in children and adolescents: analysis of susceptibility genes in 123 Italian patients. J Eur Acad Dermatol Venereol. 2022;36(2):213–221.
- Sepehr A, Chao E, Trefrey B, et al. Long-term outcome of Spitz-type melanocytic tumors. Arch Dermatol. 2011;147(10):1173–1179.