J Clin Aesthet Dermatol. 2026;19(7):8–9.
Recognizing Pyoderma Gangrenosum as a Rare Complication of Breast and Gynecologic Surgery
Dear Editor:
Pyoderma gangrenosum (PG) is a rare neutrophilic dermatosis characterized by painful, rapidly progressive ulcers with undermined borders and delayed wound healing.1 It is a reactive, noninfectious, inflammatory condition that often presents following trauma or surgery. Due to its overlapping clinical presentation with postoperative infections and pathergy phenomenon, PG has become increasingly recognized as a diagnostic challenge following breast and gynecologic surgery. This brief narrative review aims to increase recognition and treatment of PG after breast and gynecologic surgery by highlighting key lessons from published studies.
Postoperative PG often presents with features that mimic infection, contributing to frequent misdiagnosis. In a systematic review of 49 case reports of PG following breast surgery, 27 (55%) cases involved concomitant fever, and 21 (43%) cases had leukocytosis.2 Such clinical signs drive suspicion for infection, confound the clinical picture, and delay recognition of PG after breast surgery. Furthermore, early signs of PG following breast surgery can be mistaken for tissue necrosis. In a case series study by Hammond et al,3 one particular case showed impending necrosis of a mastectomy flap at 48 hours after surgery. Routine oral and systemic antibiotics were unable to treat the wound. However, when PG was considered and steroid therapy was initiated, the progression of the wound slowed down, allowing for re-epithelization.3 Consistent with these findings, PG is easily misinterpreted as infection due to its nonspecific, mimical presentation, leading to delays in appropriate immunosuppressive therapy.
Diagnostic delay of PG is well-documented. Case series indicate the average time for symptoms of PG to appear was 11 days postoperatively, yet the average time it took from symptom onset to PG diagnosis was 41 days.3 Surgical debridement and trials of antibiotic therapy contribute to the delay in diagnosis due to the misattribution of PG to postoperative infection. Consequently, the disease course of PG is exacerbated through ineffective interventions and pathergy from surgical debridement.
Similar diagnostic challenges are observed after gynecologic procedures in which PG has been reported, including cesarean sections and hysterectomies. For instance, Shen et al4 presented a case of postcesarian section PG, in which a patient developed wound breakdown 1 day following surgery. Despite a negative wound culture, PG was misdiagnosed as an infection. The patient did not respond to antibiotic therapies. Following consideration of PG and initiation of steroid therapy, the lesion healed with no adverse effects.4 Likewise, Güth et al5 highlighted PG as a late complication after hysterectomy. In this case, a patient developed vaginal dehiscence and presumed infection following a vaginal hysterectomy. The patient underwent ineffective antibiotic therapy and additional surgical procedures. Ultimately, PG of the vaginal vault was diagnosed, and dexamethasone was initiated, resulting in complete resolution of symptoms.5 Both of these cases underscore the importance of considering PG early in the course when a presumed surgical site infection is unresponsive to antibiotic therapy and wound cultures are negative. The consequences of misdiagnosing PG after a gynecologic procedure include unnecessary antibiotic courses and repeated surgeries. Not only do these procedures fail to treat PG, but they also prolong disease course by increasing wound destruction, inflammatory response, and morbidity through pathergy.
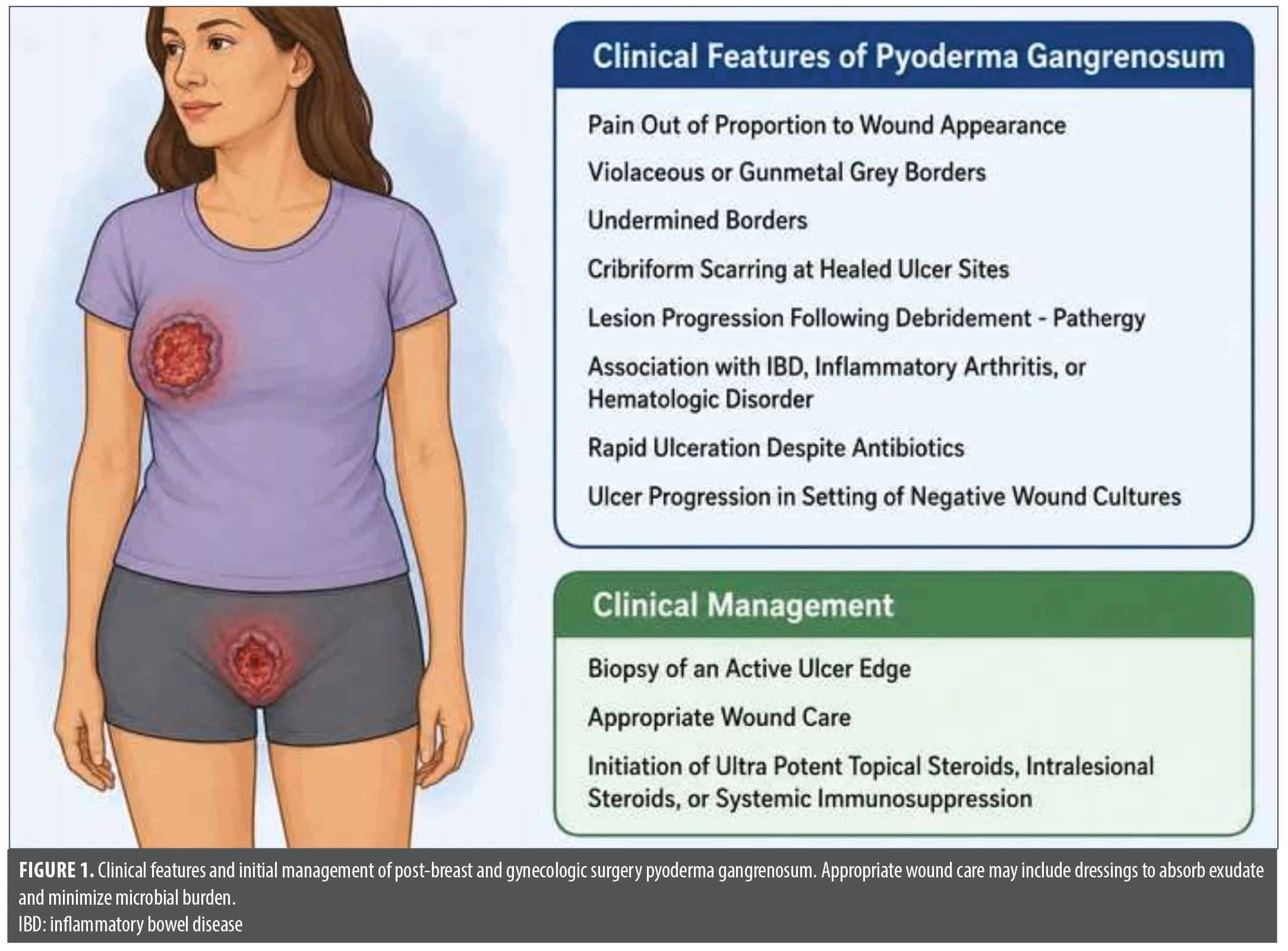
Across both breast and gynecologic surgery, the rarity and presentation of postoperative PG pose unique diagnostic and therapeutic challenges, frequently resulting in misdiagnosis. Accordingly, PG should be suspected in wounds that demonstrate rapid ulceration despite antibiotic therapy, especially when wound cultures are negative. Additional features that support the diagnosis of PG and prompt reconsideration of presumed infection include pain disproportionate to wound appearance, violaceous or undermined wound borders, cribriform scarring at healed ulcer sites, and lesion progression following debridement, consistent with pathergy.6 Underlying inflammatory bowel disease, inflammatory arthritis, or hematologic disorder should also heighten suspicion, as these are the most common systemic associations with PG.6 When clinical suspicion for PG is high, early biopsy of the active ulcer edge is advised to rule out alternative causes, such as infection, vascular disease, and malignancy, and typically reveals neutrophilic infiltration.6 Once the diagnosis is made, in addition to appropriate wound care measures, ultrapotent topical steroids, intralesional steroids, and in refractory cases, systemic immunosuppressants, such as corticosteroids, should be initiated promptly (Figure 1).6
Postoperative PG after breast and gynecologic surgery often follows a clinical pattern marked by initial misdiagnosis, delayed recognition, and disease progression exacerbated by standard medical and surgical interventions. This pattern underscores a critical gap in awareness among surgical teams that contributes to avoidable morbidity. This paper highlights the importance of recognizing key features that distinguish PG from postoperative infections to enable early consideration of the diagnosis and initiation of immunosuppressive medications, preventing postoperative morbidity from delayed wound healing and pathergy.
With regard,
Toan N. Vu, BS, and David Cotter, MD, PhD
Keywords: Pyoderma gangrenosum, neutrophilic dermatosis, breast surgery, hysterectomy, cesarean section, complication
Affiliations: Mr. Vu is with the University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin. Dr. Cotter is with Las Vegas Dermatology and the UNLV School of Medicine, Las Vegas, Nevada.
Funding: No funding was provided for this article.
Disclosures: The authors have no relevant conflicts of interest.
Correspondence: David Cotter, MD, PhD;
References
- Maronese CA, Pimentel MA, Li MM, et al. Pyoderma gangrenosum: an updated literature review on established and emerging pharmacological treatments. Am J Clin Dermatol. 2022;23(5):615–634.
- Tuffaha SH, Sarhane KA, Mundinger GS, et al. Pyoderma gangrenosum after breast surgery: diagnostic pearls and treatment recommendations based on a systematic literature review. Ann Plast Surg. 2016;77(2):e39–e44.
- Hammond D, Chaudhry A, Anderson D, et al. Postsurgical pyoderma gangrenosum after breast surgery: a plea for early suspicion, diagnosis, and treatment. Aesthetic Plast Surg. 2020;44(6):2032–2040.
- Shen J, Zhang W, Jiang X. Pyoderma gangrenosum after cesarean section treated with skin graft: a case report. Medicine (Baltimore). 2019;98(18):e15380.
- Güth U, Wagner S, Huang DJ, et al. Pyoderma gangrenosum of the vaginal vault after vaginal hysterectomy: only the correct diagnosis of a rare entity can prevent long-term morbidity. Arch Gynecol Obstet. 2013;288(1):79–82.
- Maverakis E, Ma C, Shinkai K, et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: a Delphi consensus of international experts. JAMA Dermatol. 2018;154(4):461–466.