J Clin Aesthet Dermatol. 2026;19(5–6 Suppl 1):S10–S14.
by Kyle Machynia, MPAS, PA-C
Mr. Machynia is with University of Nevada, Reno School of Medicine, Reno, Nevada.
Funding: Support for this publication was provided by Bausch Health Companies Inc.
Disclosures: KM is an honorary speaker for AbbVie, Eli Lilly, Galderma, Johnson & Johnson, and Sanofi Regeneron; and has served on advisory boards for AbbVie, Bausch, Blueprint Medicines Corporation, Bristol Myers Squibb, Castle Biosciences, Galderma, Johnson & Johnson, Leo Pharma, Ortho Dermatologics, and Sanofi Regeneron.
Introduction
Palmoplantar psoriasis is a localized and often disabling subtype of psoriasis, substantially impairing hand function and diminishing quality of life.1,2 Hyperkeratosis, fissuring, and involvement of digits frequently result in significant limitations in daily activities and occupational capacity.2–4 This form of psoriasis remains therapeutically challenging, as it is often refractory to topical and systemic agents and exhibits a heightened tendency toward Koebnerization.2 Although biologic therapies targeting the interleukin (IL)-23/IL-17 axis have revolutionized the treatment of moderate-to-severe psoriasis, palmoplantar disease remains prone to therapeutic failure and represents a persistent clinical challenge.2,5 Explaining these therapeutic failures necessitates examining how the mechanisms of individual biologics intersect with the complex immunopathogenesis of psoriasis.
The pathophysiology of psoriasis is summarized in Figure 1A.6–13 Briefly, psoriasis is driven by an inflammatory feedback loop involving keratinocytes, dendritic cells (DCs), and T helper 17 (Th17) cells.6 Environmental triggers (eg, infection, trauma) lead keratinocytes to release self-nucleotides and antimicrobial peptides that activate DCs, which produce inflammatory mediators, including IL-23, that promote and maintain a Th17 phenotype.6,11 Th17-derived IL-17 cytokines stimulate keratinocytes, promoting hyperproliferation, impaired differentiation, and perpetuation of chronic cutaneous inflammation.6,7 Additionally, keratinocyte-derived IL-17C and IL-17E signal in an autocrine manner to amplify inflammatory signaling and enhance keratinocyte activity (eg, proliferation, differentiation, migration).9,12 Targeted therapies for the treatment of psoriasis disrupt pathophysiology through the inhibition of key inflammatory mediators (Figure 1B).14–18
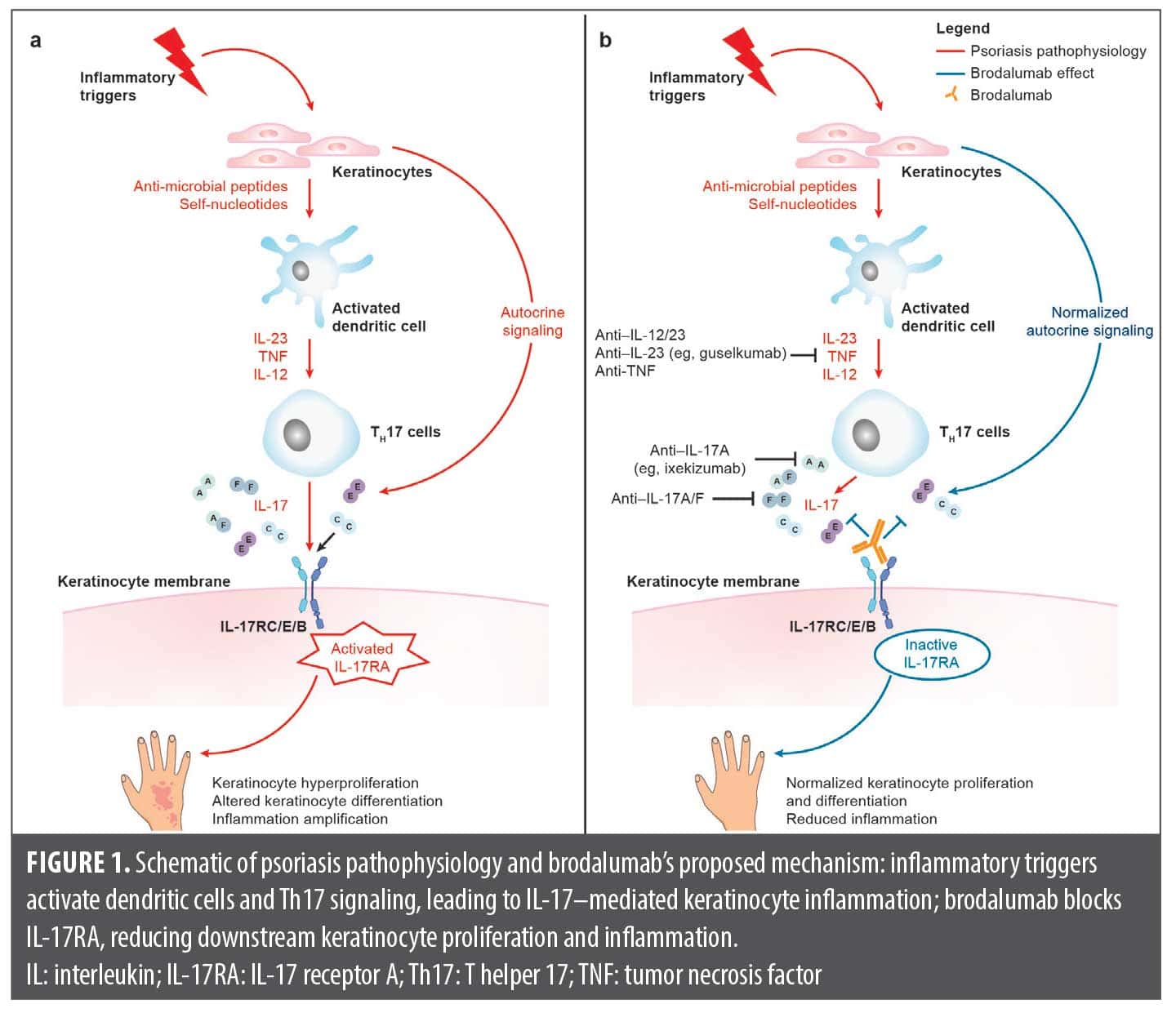
Several biologics targeting the IL-23/IL-17 pathway are approved for the treatment of moderate-to-severe plaque psoriasis in patients who are candidates for systemic therapy or phototherapy.16,17 Guselkumab, an IL-23p19 antagonist, and ixekizumab, a selective IL-17A antagonist, each inhibit discrete cytokines within this pathway.16,17 In contrast, brodalumab, a human IL-17 receptor A (IL-17RA) antagonist, blocks the IL-17 receptor itself, thereby inhibiting signaling from multiple cytokines, including IL-17A, IL-17C, IL-17E, IL-17F, and IL-17A/F.15 By inhibiting multiple IL-17 cytokines through IL-17RA antagonism, brodalumab could offer benefit in cases unresponsive to more selective pathway inhibitors.
To our knowledge, few cases have documented complete clearance with IL-17RA blockade after sequential failure of IL-23 or IL-17A inhibitors in localized palmoplantar disease. Herein, we describe a case of chronic palmoplantar psoriasis refractory to guselkumab and ixekizumab that achieved complete clearance with brodalumab. The patient provided written informed consent to publish anonymized data included in this article. As this is a case report describing retrospective and fully anonymized data from a single patient, formal approval from an institutional review board or ethics committee is not required.
Case Report
We report the case of a 62-year-old White male patient with obesity (body mass index: 41.6 kg/m2). The patient, who had no other history of psoriasis, presented to the clinic after experiencing a chronic eruption involving the palms and soles for approximately 1 year. He previously experienced minimal improvement with medium-potency topical corticosteroids and partial, temporary relief after intramuscular triamcinolone injection. The patient’s hands were more severely affected than his feet, with examination revealing thick, hyperkeratotic plaques with fissuring on the palms. Functional impairment from palm involvement substantially affected the patient’s ability to perform occupational duties as an electrician, resulting in frequent absenteeism. With corticosteroid-refractory psoriasis that substantially impaired daily functioning, the decision was made to escalate treatment to systemic biologic therapy.
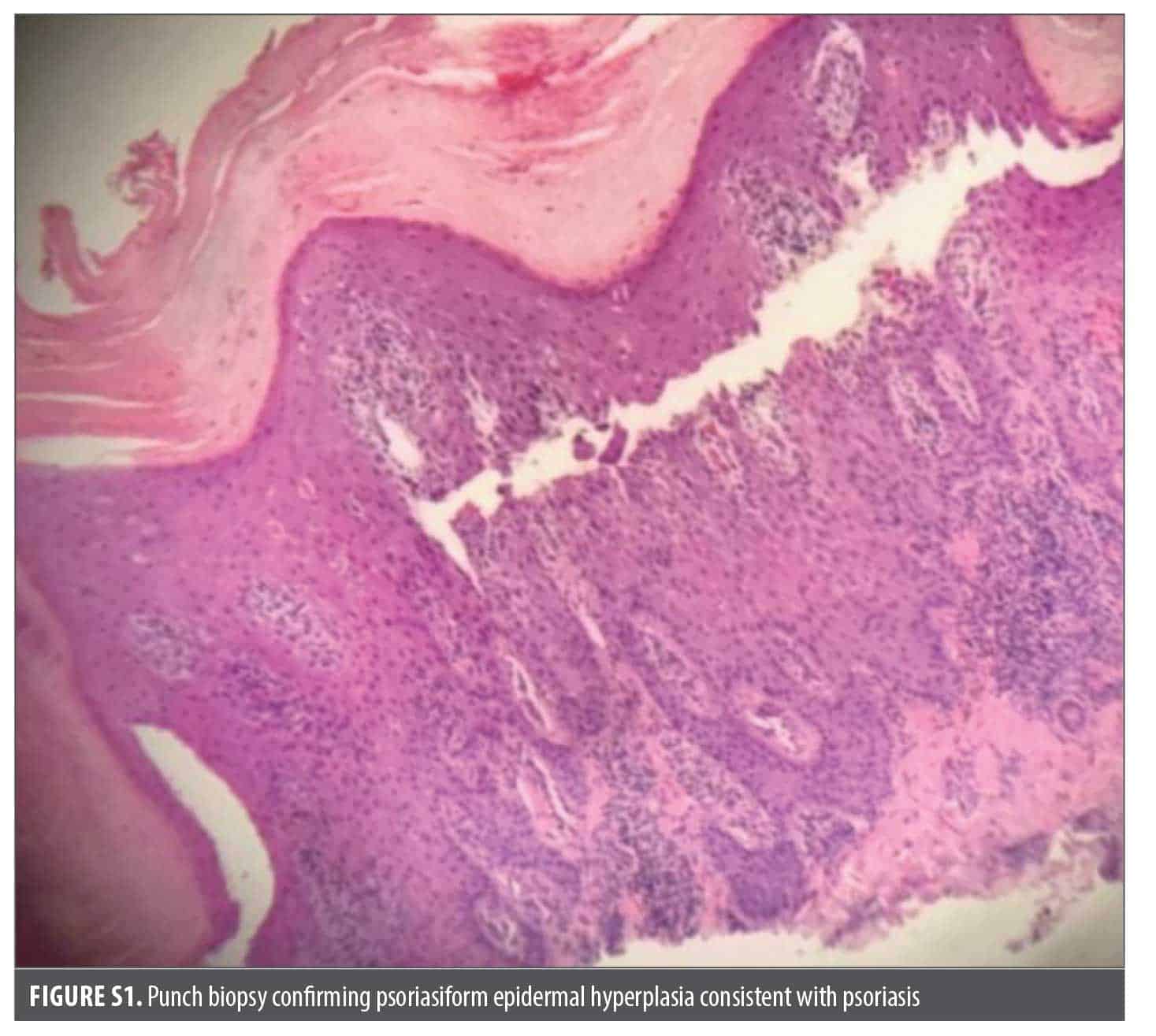
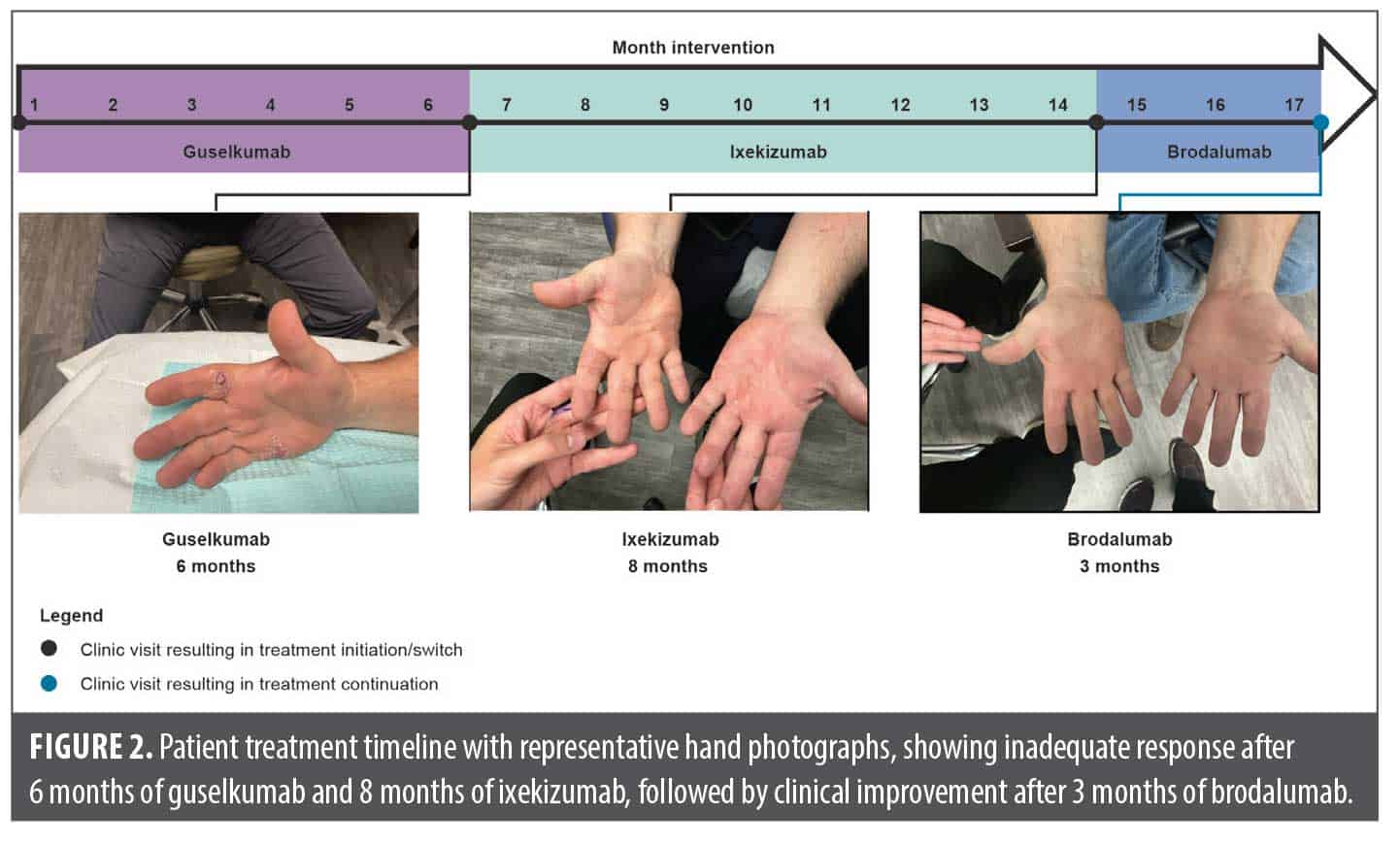
Initial treatment with guselkumab in combination with clobetasol 0.05% cream for 6 months resulted in limited improvement. To confirm the diagnosis, a 4-mm punch biopsy was performed, which revealed psoriasiform epidermal hyperplasia consistent with psoriasis (Figure S1). The patient was subsequently transitioned to ixekizumab with no washout period, with adjunctive topical clobetasol prescribed as needed for breakthrough disease. After 8 months, the patient exhibited persistent plaques and reported moderate pruritus, scoring 4 out of 10 on an itch numeric rating scale (NRS).
Brodalumab 210 mg every 2 weeks was initiated with no washout period following shared decision-making and counseling regarding potential risks and benefits. At a follow-up visit 3 months after brodalumab initiation, the patient demonstrated complete clearance of the hands and feet, with resolution of pruritus (scoring 0 out of 10 on the itch NRS) and restoration of hand function. The patient was able to resume full-time work and discontinued topical clobetasol to manage breakthrough disease. The patient experienced no adverse events. Figure 2 illustrates the treatment timeline along with representative clinical photographs of the hands.
Discussion
Our patient achieved complete clearance with brodalumab after failing to adequately respond to topical corticosteroids, intramuscular triamcinolone injection, guselkumab, and ixekizumab. The limited efficacy of topical corticosteroids in palmoplantar psoriasis is well recognized.2 In contrast, the lack of response to guselkumab and ixekizumab after 6 and 8 months of treatment, respectively, followed by complete clearance with brodalumab within 3 months of treatment, warrants further consideration. Although results cannot be directly compared across studies, phase 3 trials have consistently demonstrated robust efficacy of guselkumab, ixekizumab, and brodalumab in moderate-to-severe psoriasis, with approximately 68% to 84% of patients achieving at least a 90% improvement from baseline in Psoriasis Area and Severity Index (PASI) by 12 to 16 weeks.19–24 Clinical success with brodalumab after failure of guselkumab and ixekizumab potentially points to mechanistic differences driving divergent treatment outcomes.
Unlike other approved psoriasis biologics that selectively target 1 to 2 cytokines (eg, guselkumab [IL-23] and ixekizumab [IL-17A]), brodalumab targets IL-17RA, a shared receptor subunit, which results in inhibition of signaling from multiple IL-17 family cytokines (IL-17A, IL-17C, IL-17E, IL-17F, and IL-17A/F; Figure 1B).14–18 Beyond IL-17RA blockade, brodalumab also modulates upstream and downstream inflammatory pathways, as demonstrated by reduced expression of IL-17A, IL-17F, and IL-23A/p19 messenger ribonucleic acid (mRNA) and downregulation of genes involved in neutrophil activation, DC function, Th17 signaling, and keratinocyte proliferation.25 Moreover, unlike other biologics, IL-17RA blockade inhibits IL-17C and IL-17E, which contribute to dysregulation of keratinocyte proliferation, differentiation, and migration.9,13 Keratinocytes of psoriasiform lesions in acral regions have been shown to upregulate IL-17C and IL-36γ, driving feed-forward loops that perpetuate inflammation.26 Furthermore, although a causal relationship of IL-17E and Koebnerization is not confirmed, IL-17E induces expression of keratins characteristic of wound-repair responses, raising the possibility that IL-17E contributed to Koebnerization in our patient.9 These mechanisms might be particularly relevant in palmoplantar psoriasis, where the epidermis is anatomically distinct, with a prominent stratum lucidum, site-specific keratin expression (eg, KRT9), and dense eccrine acrosyringeal units.27,28 Taken together, the intricate cytokine signaling network of psoriasis coupled with the broad inhibitory profile of brodalumab might explain its efficacy in cases unresponsive to selective cytokine inhibitors, in palmoplantar psoriasis, and in lesions exhibiting Koebnerization.
This case report aligns with existing evidence demonstrating efficacy of brodalumab in patients who have failed prior biologic therapies and in individuals with obesity as a risk factor for treatment failure.29–33 Across several open-label postmarketing and real-world studies, 44% to 59% of participants with prior biologic failure achieved at least a 90% improvement from baseline in PASI within 12 to 16 weeks of brodalumab treatment.29,31–33 Moreover, a post-hoc analysis of AMAGINE-2/-3 trials reported that brodalumab was similarly efficacious in patients with and without obesity, despite consistent dosing of brodalumab regardless of weight.30 These data are consistent with findings from our case report, supporting the use of brodalumab in patients with prior biologic failure (including anti–IL-17A therapy) and obesity.
Additional reports have described the efficacy of brodalumab in recalcitrant palmoplantar psoriasis.34,35 In a case series of patients with extensive disease, a 33-year-old male patient with palmoplantar involvement who failed multiple systemic agents achieved substantial improvement with brodalumab as measured by PASI score, which ranges from 0 to 72, (PASI score 25 at brodalumab initiation, 7.4 at 5 weeks, and 1.9 at 44 weeks).34 Another report describes a 66-year-old male patient with a 30-year history of psoriasis (baseline PASI: 26) who had inadequate response to adalimumab after 2 months (PASI: 17.4) and subsequently developed worsening palmoplantar disease while receiving secukinumab for 7 months despite overall improvement (PASI: 3.6; Palmoplantar Pustular Area and Severity Index [PPASI]: 22.4).35 Switching to brodalumab resulted in rapid and durable improvement (PPASI: 13.2 at 2 weeks and 4.0 at 6 months), with no flares or adverse events over 1 year of follow-up. Together with our case, these findings highlight the potential role of IL-17RA antagonism in palmoplantar psoriasis unresponsive to other biologics.
This case underscores the importance of rapid clearance in patients with palm involvement to alleviate functional impairment. In our patient, brodalumab treatment led to restored hand function and improved work performance, consistent with evidence of brodalumab’s rapid onset of action.36,37 In a systematic review of phase 3 trials of IL-17 and IL-23 inhibitors, brodalumab demonstrated the shortest weighted mean time until 50% of patients achieved at least a 90% improvement from baseline in PASI compared with other agents.36 Similarly, a network meta-analysis of phase 3 trials reported that among IL-17, IL-23, IL-12/-23, and tumor necrosis factor inhibitors, brodalumab and ixekizumab were associated with the fastest onset of skin clearance.37 Consistent with the rapid functional improvement observed in our patient, a pooled subanalysis of AMAGINE-2/-3 trials reported significant improvement in Dermatology Life Quality Index (DLQI) scores compared with ustekinumab as early as Week 4 (P<0.001).38 Additionally, the aforementioned meta-analysis reported that the IL-17 class of biologics (brodalumab, ixekizumab, and secukinumab) had the greatest positive effect on DLQI.37
Conclusion
Genetic testing and cytokine profiling might improve treatment selection in psoriasis.39,40 Because these tools are not yet validated for clinical use, therapeutic sequencing in psoriasis relies on a trial-and-error approach, which often leads to treatment switching and delayed disease control.41 Brodalumab could attenuate cytokine-amplification loops more comprehensively than agents that selectively block IL-17A or indirectly reduce IL-17 activity via IL-23 inhibition, resulting in clinical benefit for patients with prior biologic treatment failure, as suggested by several studies.15,23,29,31–33 Although this case provides clinical support for the potential advantage of IL-17RA blockade, further research is needed. Robust interventional studies in larger cohorts are required to confirm these findings and to define the role of IL-17RA blockade in the management of acral-predominant psoriasis.
Acknowledgments
Medical writing support and editorial assistance were provided under the direction of the author by Fingerpaint Medical and funded by Bausch Health Companies Inc.
References
- Chung J, Callis Duffin K, Takeshita J, et al. Palmoplantar psoriasis is associated with greater impairment of health-related quality of life compared with moderate to severe plaque psoriasis. J Am Acad Dermatol. 2014;71(4):623–632.
- Menter A, Bhutani T, Ehst B, et al. Narrative review of the emerging therapeutic role of brodalumab in difficult-to-treat psoriasis. Dermatol Ther (Heidelb). 2022;12(6):1289–1302.
- Engin B, Aşkın Ö, Tüzün Y. Palmoplantar psoriasis. Clin Dermatol. 2017;35(1):19–27.
- Murakami M, Terui T. Palmoplantar pustulosis: current understanding of disease definition and pathomechanism. J Dermatol Sci. 2020;98(1):13–19.
- Campa M, Mansouri B, Warren R, Menter A. A review of biologic therapies targeting IL-23 and IL-17 for use in moderate-to-severe plaque psoriasis. Dermatol Ther (Heidelb). 2016;6(1):1–12.
- Brembilla NC, Boehncke WH. Revisiting the interleukin 17 family of cytokines in psoriasis: pathogenesis and potential targets for innovative therapies. Front Immunol. 2023;14:1186455.
- Zhou X, Chen Y, Cui L, et al. Advances in the pathogenesis of psoriasis: from keratinocyte perspective. Cell Death Dis. 2022;13(1):81.
- Vidal S, Puig L, Carrascosa-Carrillo JM, et al. From messengers to receptors in psoriasis: the role of IL-17RA in disease and treatment. Int J Mol Sci. 2021;22(13):6740.
- Borowczyk J, Buerger C, Tadjrischi N, et al. IL-17E (IL-25) and IL-17A differentially affect the functions of human keratinocytes. J Invest Dermatol. 2020;140(7):1379–1389.e2.
- Song X, Zhu S, Shi P, et al. IL-17RE is the functional receptor for IL-17C and mediates mucosal immunity to infection with intestinal pathogens. Nat Immunol. 2011;12:1151–1158.
- Gonçalves MBS, Fonseca M, Mascarenhas-Melo F, Figueiras A. Advancing insights into psoriasis: from pathogenesis to current and emerging therapies. Int Immunopharmacol. 2025;165:115429.
- Lauffer F, Jargosch M, Baghin V, et al. IL-17C amplifies epithelial inflammation in human psoriasis and atopic eczema. J Eur Acad Dermatol Venereol. 2020;34(4):800–809.
- Johnston A, Fritz Y, Dawes SM, et al. Keratinocyte overexpression of IL-17C promotes psoriasiform skin inflammation. J Immunol. 2013;190(5):2252–2262.
- Menter A, Strober BE, Kaplan DH, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2019;80(4):1029–1072.
- Siliq. Package insert. Bausch Health US, LLC; 2020.
- Taltz. Package insert. Eli Lilly and Company; 2024.
- Tremfya. Package insert. Janssen Biotech, Inc; 2017.
- Bimzelx. Package insert. UCB, Inc; 2023.
- Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405–417.
- Reich K, Armstrong AW, Foley P, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76(3):418–431.
- Gordon KB, Colombel JF, Hardin DS. Phase 3 trials of ixekizumab in moderate-to-severe plaque psoriasis. N Engl J Med. 2016;375(21):2102.
- Griffiths CEM, Reich K, Lebwohl M, et al. Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): results from two phase 3 randomised trials. Lancet. 2015;386(9993):541–551.
- Lebwohl M, Strober B, Menter A, et al. Phase 3 studies comparing brodalumab with ustekinumab in psoriasis. N Engl J Med. 2015;373(14):1318–1328.
- Papp KA, Reich K, Paul C, et al. A prospective phase III, randomized, double-blind, placebo-controlled study of brodalumab in patients with moderate-to-severe plaque psoriasis. Br J Dermatol. 2016;175(2):273–286.
- Tomalin LE, Russell CB, Garcet S, et al. Short-term transcriptional response to IL-17 receptor-A antagonism in the treatment of psoriasis. J Allergy Clin Immunol. 2020;145(3):922–932.
- Friedrich M, Tillack C, Wollenberg A, et al. IL-36γ sustains a proinflammatory self-amplifying loop with IL-17C in anti-TNF-induced psoriasiform skin lesions of patients with Crohn’s disease. Inflamm Bowel Dis. 2014;20(11):1891–1901.
- Tsai J, Rostom M, Garza LA. Understanding and harnessing epithelial–mesenchymal interactions in the development of palmoplantar identity. J Invest Dermatol. 2022;142(2):282–284.
- Murakami M, Ohtake T, Horibe Y, et al. Acrosyringium is the main site of the vesicle/pustule formation in palmoplantar pustulosis. J Invest Dermatol. 2010;130(8):2010–2016.
- Balestri R, Odorici G, Magnano M, et al. Switching to brodalumab after failure of IL-17A inhibitors in psoriatic patients: a real-life multicentre study. J Eur Acad Dermatol Venereol. 2026;40(1):e48–e51.
- Hsu S, Green LJ, Lebwohl MG, et al. Comparable efficacy and safety of brodalumab in obese and nonobese patients with psoriasis: analysis of two randomized controlled trials. Br J Dermatol. 2020;182(4):880–888.
- Kimmel G, Chima M, Kim HJ, et al. Brodalumab in the treatment of moderate to severe psoriasis in patients when previous anti-interleukin 17A therapies have failed. J Am Acad Dermatol. 2019;81(3):857–859.
- Papp K, Prajapati VH, Maari C, et al. Efficacy of brodalumab in moderate-to-severe plaque psoriasis after failure of previous biologic therapy: a phase 4, multicenter, open-label study. J Am Acad Dermatol. 2024;90(6):1254–1256.
- Yeung J, Vender R, Turchin I, et al. Brodalumab success in patients with moderate-to-severe psoriasis who failed previous interleukin-17A inhibitors. J Am Acad Dermatol. 2021;84(4):1169–1171.
- Pinter A, Bonnekoh B, Hadshiew IM, Zimmer S. Brodalumab for the treatment of moderate-to-severe psoriasis: case series and literature review. Clin Cosmet Investig Dermatol. 2019;12:509–517.
- Nakao M, Asano Y, Kamata M, et al. Successful treatment of palmoplantar pustular psoriasis with brodalumab. Eur J Dermatol. 2018;28(4):538–539.
- Egeberg A, Andersen YMF, Halling-Overgaard AS, et al. Systematic review on rapidity of onset of action for interleukin-17 and interleukin-23 inhibitors for psoriasis. J Eur Acad Dermatol Venereol. 2020;34(1):39–46.
- Warren RB, See K, Burge R, et al. Rapid response of biologic treatments of moderate-to-severe plaque psoriasis: a comprehensive investigation using Bayesian and frequentist network meta-analyses. Dermatol Ther (Heidelb). 2020;10(1):73–86.
- Lambert J, Hansen JB, Sohrt A, Puig L. Dermatology Life Quality Index in patients with moderate-to-severe plaque psoriasis treated with brodalumab or ustekinumab. Dermatol Ther (Heidelb). 2021;11(4):1265–1275.
- Dand N, Mahil SK, Capon F, et al. Psoriasis and genetics. Acta Derm Venereol. 2020;100(3):adv00030.
- Solberg SM, Sandvik LF, Eidsheim M, et al. Serum cytokine measurements and biological therapy of psoriasis – prospects for personalized treatment? Scand J Immunol. 2018;88(6):e12725.
- Strober B, Pariser D, Deren-Lewis A, et al. A survey of community dermatologists reveals the unnecessary impact of trial-and-error behavior on the psoriasis biologic treatment paradigm. Dermatol Ther (Heidelb). 2021;11(5):1851–1860.