Mark Lebwohl, MD; Norman Preston, PhD; Ronald W. Gottschalk, MD, FRCPC
Dr. Lebwohl is from Mount Sinai School of Medicine, New York, New York; Drs. Preston and Gottschalk are from Galderma Laboratories, L.P., Fort Worth, Texas
Disclosure: Dr. Lebwohl is a consultant for Abgenomics, Allos, Amgen Inc., Astellas Pharma Inc., Can-Fite Biopharma, Centocor, Inc., DermaGenoma, DermiPsor, Galderma Laboratories, L.P., Glenmark Pharmaceuticals, GSK-Stiefel, Inc., HelixBioMedix, Janssen Ortho Biotech, Leo Pharmaceuticals, Medicis Pharmaceutical Corporation, Novartis Pharmaceuticals Corporation, Pfizer, PharmaDerm Ranbaxy, and Valeant Pharmaceuticals. Drs. Preston and Gottschalk are employed by Galderma Laboratories, L.P., Fort Worth, Texas. Funding for these analyses and for manuscript preparation was provided by Galderma Laboratories, L.P., Fort Worth, Texas.
Abstract
Objective: Calcitriol 3µg/g ointment has been shown to be a safe and effective treatment for adults with mild-to-moderate plaque psoriasis. This analysis evaluated the response to calcitriol 3µg/g ointment relative to baseline disease. Design: Retrospective analysis of data from a 12-month safety and tolerability trial. Setting and participants: At baseline, 40.1 percent (130/324) of patients had an affected body surface area of 11 to 20 percent, and 55.2 percent (179/324) had moderate and 25.9 percent (84/324) had severe disease according to global severity score. Patients applied calcitriol 3µg/g ointment twice daily for up to 52 weeks. Measurements: Change in investigator’s global severity scores and involved body surface area at Week 26 (N=249) and Week 52 (N=130) relative to baseline. Results: Compared with baseline, most patients experienced at least a 1-grade improvement in global severity score at Weeks 26 (195/249, 78.3%) and 52 (109/130, 83.8%). Stabilization (i.e., no change in global severity score) was reported in 19.3 percent (48/249) at Week 26 and in 12.3 percent (16/130) at Week 52. Most patients also experienced at least a 1-grade improvement in body surface area involved at Weeks 26 (152/249, 61.0%) and 52 (95/130, 73.1%). Stabilization (no change in affected body surface area) was reported in 32.5 percent (81/249) at Week 26 and 24.6 percent (32/130) at Week 52. The proportion of patients experiencing improvement in global severity score and body surface area was comparable across all categories of severity and disease extent at baseline. Conclusion: This analysis suggests that calcitriol 3µg/g ointment use for 26 weeks (N=249) and 52 weeks (N=130) was associated with disease improvement or stabilization in most patients with plaque psoriasis.
(J Clin Aesthet Dermatol. 2012;5(2):28–33.)
Psoriasis is a chronic, immune-mediated disease that affects 2 to 3 percent of the United States population and causes significant psychological and social distress and impairment of health-related quality of life (QoL).[1–3] Infiltration of T lymphocytes into the skin, release of inflammatory mediators, keratinocyte hyperplasia, and proliferation of skin epithelial cells gives rise to the thick hyperkeratotic inflammatory plaques that are a common manifestation of the disease.[4] Topical therapies are used frequently and are effective across the full spectrum of disease severity when used alone or in combination with other topical therapies or systemic agents.[5] Topical vitamin D products have emerged as effective and well-tolerated treatments for adult patients with mild-to-moderate plaque psoriasis. Vitamin D products have shown a number of physiological effects that are thought to be important in the treatment of psoriasis. These include inhibition of T-cell proliferation, T-cell mediated immune responses, suppression of inflammatory mediators, and reduction in epidermal keratinocyte proliferation.[6,7] For example, vitamin D is known to alter the release of cytokines, chemokines, and growth factors from activated T-cells that contribute to the proliferation and differentiation of keratinocytes.[6–8]
Until recently, calcipotriene, a vitamin D analog, was the only topical vitamin D product approved for the treatment of psoriasis. This agent has been shown to produce improvement and clearing of lesions when used alone or in combination with a topical corticosteroid in patients with plaque psoriasis.[9–13]
Calcitriol 3µg/g ointment has also been developed and was approved in 2009 by the US Food and Drug Administration (FDA) for the treatment of mild-to-moderate plaque psoriasis in patients 18 years and older. When applied twice daily for up to 8 or 12 weeks in randomized clinical trials, this formulation produced improvement of the signs and symptoms of psoriasis and was well tolerated with a low incidence of adverse events and no clinically significant effects on calcium homeostasis.[14,15]
The long-term safety and efficacy of calcitriol ointment was evaluated in patients with stable, mild-to-moderate plaque psoriasis involving up to 35 percent of the body surface area (BSA).[16] The post-hoc analysis presented here reviews some data relevant to BSA outcomes in subjects who finished at various time points during the study. Patients were treated with calcitriol 3µg/g ointment twice daily for 26 weeks (Phase 1) in an uncontrolled fashion with an option to continue for up to 52 weeks (Phase 2).16 In this study, calcitriol was found to be safe and well tolerated.
A total of eight participants withdrew from the study because of adverse events, four (1.2%) of which were deemed related to study treatment and included irritant dermatitis, pruritus, kidney pain, and urine abnormality (1 each). None of the serious or severe adverse events were attributed to study treatment. The proportion of patients rated as clear or almost clear increased over the study period, from 22.1 percent (63/285) at the end of 26 weeks to 47.1 percent (66/140) at the end of 52 weeks.16 However, because participation in Phase 2 of the study (i.e., beyond the initial 26 weeks) was optional, the exclusion of patients who opted to not participate in Phase 2 (possibly for lack of efficacy) may have biased the efficacy results at the end of 52 weeks.
The objective of this retrospective analysis of data from the trial is to examine the extent of improvement in involved BSA and investigator’s global severity score (GSS) at Week 26 and Week 52 relative to baseline severity and duration of subject participation in the trial.
METHODS
The complete study design and primary results of this open-label, multicenter study are published elsewhere.[16] Briefly, patients in the trial were older than 12 years of age and had stable, chronic plaque psoriasis affecting up to 35 percent BSA that was of mild-to-moderate severity, defined as a rating of at least 2 on a 6-point GSS.[16]
Patients were excluded if they had other forms of psoriasis; if they had recently received antipsoriatic therapy, including topical vitamin D3 derivatives, corticosteroids, or retinoids within the preceding two weeks, or systemic corticosteroids, retinoids, immunomodulatory drugs, or psoralen plus ultraviolet A (UVA) therapy within the preceding four weeks; if they had recently started medications that could aggravate psoriasis; if they had medical conditions requiring treatment with vitamin D3 or calcium; if they had hypercalcemia, renal dysfunction, or calcium-based calculi; or if they had medical or psychiatric conditions that, in the opinion of the investigator, might put the participant at risk or confound the results of the study. Pregnant and breastfeeding women were also excluded from participation.
All patients were instructed to apply calcitriol 3µg/g ointment (Galderma Laboratories, L.P., Fort Worth, Texas) twice daily for up to 52 weeks to psoriasis plaques. Patients were considered to have completed the study if they participated for 26 or 52 weeks. The study was performed in accordance with the Declaration of Helsinki and all patients provided written informed consent before undergoing any study procedures.
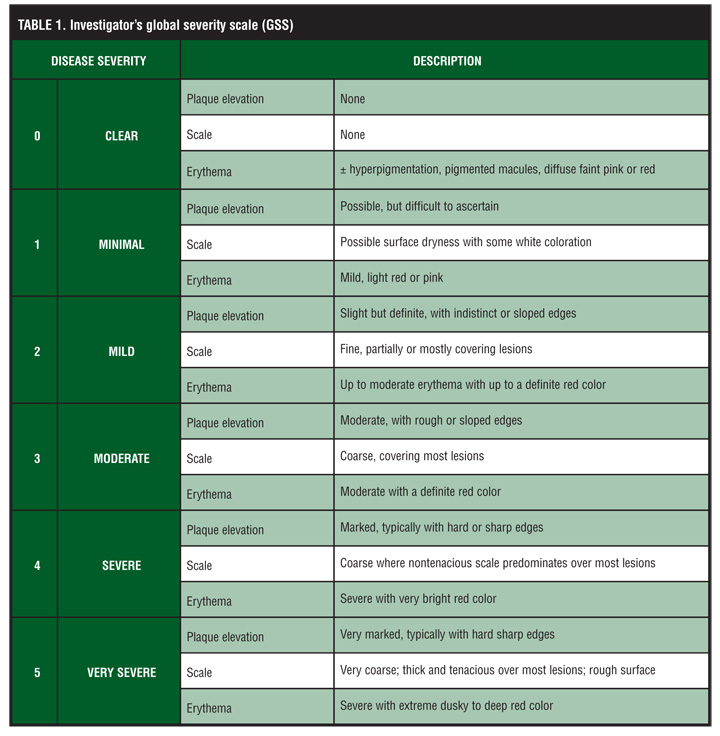
Assessments. At baseline and at each visit during treatment, investigators evaluated patients and rated disease severity according to the 6-point psoriasis GSS (Table 1). Disease severity was also assessed according to the percentage of affected BSA, which was divided into seven categories (0–5%, 6–10%, 11–15%, 16–20%, 21–25%, 26–30%, 31–35%, and >35%). For the present analysis, patients within each category of disease severity at baseline (according to GSS and BSA affected) were evaluated to determine whether signs and symptoms improved (at least 1-grade/category decrease in GSS/BSA affected), worsened (at least 1-grade/category increase in GSS/BSA affected), or remained in the same category relative to baseline.
{kind=link}
Statistical analyses. All patients with an investigator’s GSS score and an assessment of BSA affected at baseline, 26 weeks, and 52 weeks were included in this analysis. The endpoints of interest in this retrospective analysis were the proportion of patients with improved or stable GSS score and BSA affected after 26 and 52 weeks.
RESULTS
A total of 324 patients were enrolled in the study and received calcitriol ointment 3µg/g. Of these, investigator’s GSS score and assessment of BSA affected were available for 249 (76.8%) and 130 (40.1%) patients at 26 weeks and 52 weeks, respectively. Per the study protocol, patients had the option of stopping treatment at Week 26; thus, electing to complete the study after 26 weeks was the most common reason for not completing 52 weeks of treatment. The baseline characteristics of patients who completed 26 and 52 weeks of treatment are shown in Table 2 and a title=”Table 3
“href=” https://jcadonline.com/wp-content/uploads/lebfebtable3.jpg”>Table 3.
{kind=link}
At baseline, most patients had moderate (179/324; 55.2%) or severe (84/324; 25.9%) disease according to GSS. A total of 35.8 percent (116/324) had an affected BSA of ?10 percent, and 40.1 percent (130/324) of patients had an affected BSA of 11 to 20 percent at baseline (a title=”Table 3
“href=” https://jcadonline.com/wp-content/uploads/lebfebtable3.jpg”>Table 3). The distribution of baseline GSS scores and percentage of involved BSA at baseline was similar in the subgroups of patients who completed 26 and 52 weeks of treatment (a title=”Table 3
“href=” https://jcadonline.com/wp-content/uploads/lebfebtable3.jpg”>Table 3).
Compared with baseline, most patients experienced an improvement in GSS score at Week 26 (195/249, 78.3%) and at Week 52 (109/130, 83.8%). Disease stabilization (no change in GSS score) was reported in 19.3 percent of patients (48/249) at Week 26 and in 12.3 percent of patients (16/130) at Week 52. Thus, 97.6 percent (243/249) and 96.1 percent (125/130) of all patients completing 26 and 52 weeks of therapy, respectively, experienced either improvement or stabilization in their GSS score.
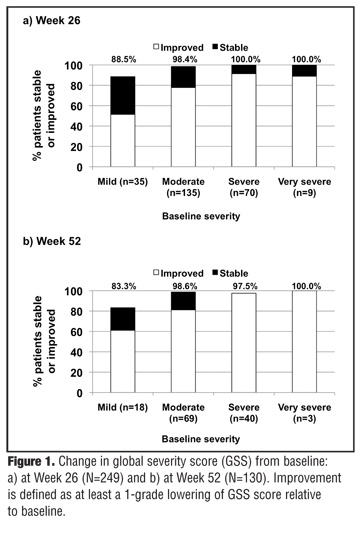
Overall, of the patients with moderate, severe, or very severe GSS scores at baseline, 82.7 percent (177/214) had an improved GSS score at 26 weeks and 87.5 percent (98/112) had an improved GSS score at 52 weeks. Among these, 31.3 percent (67/214) and 39.3 percent (44/112) had a rating of either clear or almost clear at 26 and 52 weeks, respectively. The breakdown of GSS at 26 and 52 weeks according to baseline GSS is illustrated in Figure 1.
{kind=link}
Consistent with the trends in GSS scores, most patients also experienced improvement in BSA involved at Week 26 (152/249, 61.0%) and at Week 52 (95/130, 73.1%). Disease stabilization (no change in affected BSA) was reported in 32.5 percent of patients (81/249) at Week 26 and 24.6 percent of patients (32/130) at Week 52. Thus, the overall percentage of patients who experienced either an improvement or stabilization of the affected BSA was 93.5 percent and 97.7 percent of those who completed 26 and 52 weeks, respectively.
Of the patients with psoriasis affecting >10-percent BSA at baseline, an improvement in BSA affected was exhibited by 75.3 percent (119/158) and 85.9 percent (67/78) at 26 and 52 weeks, respectively. Among these, 26.6 percent (42/158) and 42.3 percent (33/78) had 0 to 5 percent BSA affected at 26 and 52 weeks, respectively. The breakdown of BSA affected at 26 and 52 weeks according to baseline BSA affected is shown in Figure 2.
{kind=link}
DISCUSSION
The results of this analysis suggest that many patients with plaque psoriasis derive benefit from twice-daily treatment with calcitriol 3µg/g ointment for up to 52 weeks, regardless of the severity at baseline. After 26 weeks, 97.6 percent of patients remaining in the study at that time point experienced improvement or stabilization in GSS scores and 93.5 percent experienced an improvement or stabilization in the percentage of BSA affected. Consistent with these results, 96.1 percent of patients who remained in the study for 52 weeks experienced improvement or stabilization in GSS scores and 97.7 percent experienced an improvement or stabilization in the percentage of affected BSA after 52 weeks of treatment. Among patients with moderate, severe, or very severe disease according to baseline GSS ratings, 82.7 percent exhibited an improvement in GSS score at 26 weeks and 87.5 percent exhibited improvement at 52 weeks. Similarly, among patients with >10 percent BSA affected at baseline, 75.3 percent exhibited improvement in BSA affected at 26 weeks, and 85.9 percent exhibited improvement in BSA affected at 52 weeks. The observation that none of the patients with 0 to 5 percent affected BSA at baseline improved at 26 and 52 weeks is not surprising, given the difficulty in achieving clinical improvement with relatively limited disease. Nevertheless, 100 percent of patients with 0 to 5 percent affected BSA at baseline exhibited stable disease at 26 weeks, and 92 percent exhibited stable disease at 52 weeks.
These findings add to what was previously known about the efficacy of this drug. In large, randomized, vehicle-controlled trials, the therapeutic effects of calcitriol 3µg/g ointment became evident within two weeks and were sustained throughout the eight-week planned duration of treatment.[15]
The clinical benefit of vitamin D products in psoriasis is thought to be the result of effects on the keratinocyte (inhibiting proliferation, normalizing differentiation). As such, calcitriol 3µg/g ointment offers a mechanism of action that is complementary to corticosteroids for addressing different aspects of a multifactorial disease. The results of this analysis suggest the ability of calcitriol 3µg/g ointment to improve or stabilize psoriasis patients for the long-term management of their disease.
The long-term safety and tolerability of calcitriol 3µg/g ointment was demonstrated in the original clinical trial from which the present analysis was derived. In this and other studies, the incidence of hypercalcemia has been rare and generally not of clinical significance, even in patients who have used the drug to treat 25 to 35 percent of BSA for several months or longer.[15–17] The incidence of local, treatment-related adverse events is generally low and the intensity is mostly mild.[15–17] Additionally, calcitriol 3µg/g ointment may be used in even sensitive skin areas (flexural areas such as axillae and groin) with limited irritation.[18]
The findings from the present analysis suggest that calcitriol is suitable for consideration in longer term management of plaque psoriasis as part of a regimen since its use as monotherapy has been safe and generally well tolerated over extended periods of time (up to 26 to 52 weeks).[16] With respect to changes in GSS and BSA affected, “stabilization” was characterized as a favorable outcome in addition to the proportion who experienced improvement in these parameters. The clinical relevance of stabilization should not be discounted, especially for a chronic condition such as plaque psoriasis, in which symptom severity can vary considerably over time, with periods of quiescence interposed with periods of exacerbation.[19] Similarly, a “rebound phenomenon” with topical corticosteroids has been described, in which symptoms recur and are often more severe relative to symptom severity prior to initiating topical corticosteroid therapy.[5,20,21] As such, the observation in the present analysis that many patients did not worsen during treatment (for up to 26 to 52 weeks) with little to no impact on safety may be an important consideration for clinicians.
However, although intriguing, this analysis is limited by the fact that it was a retrospective analysis of data from a trial that was not designed to assess efficacy. Furthermore, the lack of a control group in the original trial makes it difficult to determine whether the changes in disease severity were influenced by fluctuations in the natural course of disease that may be expected over 26 to 52 weeks. As such, adequately designed, prospective, controlled studies are required to confirm the efficacy of calcitriol 3µg/g ointment across the spectrum of disease severity. Another limitation of the present analysis is that patients had the option to complete the study at Week 26, which resulted in a large number of patients electing to complete the study at that time point.
In conclusion, the results of this retrospective, long-term study suggest that treatment for up to 52 weeks with calcitriol 3µg/g ointment resulted in improvement or stabilization of disease (with little or no impact on safety) in many patients with plaque psoriasis, regardless of baseline disease severity.
ACKNOWLEDGMENT
The authors wish to acknowledge the role of Kevin Jarvis, PharmD, from BioCentric, Inc., in helping prepare the manuscript (drafting an outline and manuscript first draft), compiling author comments, and styling and submitting the manuscript to the journal.
References
1. Koo J. Population-based epidemiologic study of psoriasis with emphasis on quality of life assessment. Dermatol Clin. 1996;14(3):485–496.
2. Rapp SR, Feldman SR, Exum ML, Fleischer AB, Jr, Reboussin DM. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41(3 Pt 1):401–407.
3. Rapp SR, Cottrell CA, Leary MR. Social coping strategies associated with quality of life decrements among psoriasis patients. Br J Dermatol. 2001;145(4):610–616.
4. Krueger JG, Bowcock A. Psoriasis pathophysiology: current concepts of pathogenesis. Ann Rheum Dis. 2005;64 (Suppl 2):ii30–ii36.
5. Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 3. Guidelines of care for the management and treatment of psoriasis with topical therapies. J Am Acad Dermatol. 2009;60(4):643–659.
6. Jones G, Byford V, Makin HL, et al. Anti-proliferative activity and target cell catabolism of the vitamin D analog 1 alpha,24(S)-(OH)2D2 in normal and immortalized human epidermal cells. Biochem Pharmacol. 1996;52(1):133–140.
7. Shahriari M, Kerr PE, Slade K, Grant-Kels JE. Vitamin D and the skin. Clin Dermatol. 2010;28(6):663–668.
8. Scott LJ, Dunn CJ, Goa KL. Calcipotriol ointment. A review of its use in the management of psoriasis. Am J Clin Dermatol. 2001;2(2):95–120.
9. Dubertret L, Wallach D, Souteyrand P, et al. Efficacy and safety of calcipotriol (MC 903) ointment in psoriasis vulgaris. A randomized, double-blind, right/left comparative, vehicle-controlled study. J Am Acad Dermatol. 1992;27(6 Pt 1):983–988.
10. Green C, Ganpule M, Harris D, et al. Comparative effects of calcipotriol (MC903) solution and placebo (vehicle of MC903) in the treatment of psoriasis of the scalp. Br J Dermatol. 1994;130(4):483–487.
11. Highton A, Quell J. Calcipotriene ointment 0.005% for psoriasis: a safety and efficacy study. Calcipotriene Study Group. J Am Acad Dermatol. 1995;32(1):67–72.
12. Kragballe K, Barnes L, Hamberg KJ, et al. Calcipotriol cream with or without concurrent topical corticosteroid in psoriasis: tolerability and efficacy. Br J Dermatol. 1998;139(4): 649–654.
13. Papp KA, Guenther L, Boyden B, et al. Early onset of action and efficacy of a combination of calcipotriene and betamethasone dipropionate in the treatment of psoriasis. J Am Acad Dermatol. 2003;48(1):48–54.
14. Barker JN, Berth-Jones J, Groves R, et al. Calcium homeostasis remains unaffected after 12 weeks’ therapy with calcitriol 3 microg/g ointment; no correlation with extent of psoriasis. J Dermatolog Treat. 2003;14(1):14–21.
15. Lebwohl M, Menter A, Weiss J, et al. Calcitriol 3 microg/g ointment in the management of mild to moderate plaque type psoriasis: results from 2 placebo-controlled, multicenter, randomized double-blind, clinical studies. J Drugs Dermatol. 2007;6(4):428–435.
16. Lebwohl M, Ortonne JP, Andres P, Briantais P. Calcitriol ointment 3 microg/g is safe and effective over 52 weeks for the treatment of mild to moderate plaque psoriasis. Cutis. 2009;83(4):205–212.
17. Langner A, Ashton P, van de Kerkhof PC, Verjans H. A long-term multicentre assessment of the safety and tolerability of calcitriol ointment in the treatment of chronic plaque psoriasis. Br J Dermatol. 1996;135(3):385–389.
18. Ortonne JP, Humbert P, Nicolas JF, et al. Intra-individual comparison of the cutaneous safety and efficacy of calcitriol 3 microg g(-1) ointment and calcipotriol 50 microg g(-1) ointment on chronic plaque psoriasis localized in facial, hairline, retroauricular or flexural areas. Br J Dermatol. 2003;148(2):326–333.
19. Nevitt GJ, Hutchinson PE. Psoriasis in the community: prevalence, severity, and patients’ beliefs and attitudes towards the disease. Br J Dermatol. 1996;135:533–537.
20. Menter A, Abramovits W, Colon LE, Johnson LA, Gottschalk RW. Comparing clobetasol propionate 0.05% spray to calcipotriene 0.005% betamethasone dipropionate 0.064% ointment for the treatment of moderate to severe plaque psoriasis. J Drugs Dermatol. 2009;8(1):52–57.
21. Mommers JM, van Erp PE, van De Kerkhof PC. Clobetasol under hydrocolloid occlusion in psoriasis results in a complete block of proliferation and in a rebound of lesions following discontinuation. Dermatology. 1999;199(4):323–327.