aJ Clin Aesthet Dermatol. 2026;19(5):50–53.
by Elise Lau, BS; Jeremy Haskins, MS; Vishnu Palaniappan, BA; and Kumar Nadhan, MD
Ms. Lau, Mr. Haskins, and Dr. Nadhan are with Schweiger Dermatology Group in San Francisco, California. Mr. Palaniappan is with Kansas City University, Kansas City, Missouri.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
ABSTRACT: OBJECTIVE: To improve patient-centered dermatology care by identifying how patients prefer to approach medical decision-making and structuring their visit, using a brief 4-question intake survey focused on cognitive style. METHODS: New patients at 2 dermatology clinics within the California Skin Institute completed a multiple-choice intake questionnaire before their first visit. The survey asked patients how many concerns they wanted to address, how much guidance they preferred in selecting treatment, whether they prioritized diagnosis or treatment during the visit, and their expected timeline for results. Associations between patient responses and demographics (sex, age, chief complaint) were analyzed using χ2 tests. RESULTS: Among 257 patients (mean age: 38; 43% female), 96% of patients preferred to address only 1 or 2 concerns during their first visit; 75% preferred shared decision-making and 70% prioritized discussing treatment over their medical history. Patients bringing multiple concerns were significantly more likely to prefer autonomous decision-making (χ2=24.0; P<0.001). Women more often preferred to discuss multiple concerns and to balance history with treatment (both P<0.01), while men leaned toward single-concern, treatment-focused visits. LIMITATIONS: Single-center design and moderate sample size may limit generalizability. CONCLUSION: This brief, previsit framework offers a structured method to align dermatologic care with patients’ cognitive and decision-making preferences—enhancing efficiency, rapport, and mutual understanding prior to the clinical encounter. By facilitating clearer communication from the outset, it may improve the quality of patient-centered care. Future studies will explore whether tailoring consultation styles to patient preferences can impact adherence, satisfaction, and clinical outcomes. KEYWORDS: Shared decision-making, selective paternalism, patient-centered care, dermatology, cognitive style, expectations, efficiency
Introduction
In dermatology, unmet expectations—not clinical complexity—are often the biggest drivers of patient dissatisfaction.1 While clinicians strive to deliver evidence-based treatment, patients arrive with diverse goals, timeframes, and cognitive approaches to decision-making. In a time-limited visit, misalignment on these factors can lead to confusion, overwhelm, disengagement, or an asymmetrical physician-patient relationship. To address this, we piloted a 4-question intake survey to help patients identify their medical decision-making style before their first new patient appointments. The goal was simple to conceive but difficult to achieve: to frame the visit around how a patient would like to approach their concerns, not just what kind of skin problem they have.
The survey asked patients how many concerns they want to tackle, how much guidance they prefer, whether the clinician should focus more on diagnosis or treatment, and how long they expect results to take. While shared decision-making (SDM) was a generational revelation to improve adherence and satisfaction, not every patient wants—or is ready—to engage the same way. Preferences are shaped by values, lifestyle, and emotional context, all of which can change daily. This study explores how preferences vary across patients and identifies patterns by sex, age, and visit type to better tailor the clinical encounter.
Methods
Over a 3-month period, new patients at 2 California Skin Institute clinics (San Mateo and Nob Hill, San Francisco) were invited to complete a brief intake questionnaire in the examination room before their dermatology appointments. The survey included 4 multiple-choice questions designed to uncover each patient’s cognitive style and consultation preferences:
1. How many skin issues would you like to focus on today?
- A. 1 project
- B. 2 projects
- C. 3 projects
2. How much guidance would you prefer in choosing a treatment plan?
- A. I will decide based on the options provided
- B. I prefer shared-decision making between you and me
- C. I don’t want treatment; I want answers only
3. How would you prefer to focus our time together?
- A. I want to focus on the past (medical history)
- B. I want to focus on the future (treatment)
- C. A little bit of each
4. How long do you expect it will take to achieve the desired results?
- A. 1 week
- B. 2–4 weeks
- C. 2–3 months
- D. 4–12 months
Responses were excluded if incomplete or if multiple answers were selected per question. Although anonymous, patients were encouraged to share their answers with their provider to guide the visit.
For analysis, age was grouped (18–29, 30–64, 65+ years), and chief complaint categories included rash, full-body skin exam (FBSE), neoplasm, and hair concerns. Associations between demographics or clinical variables and survey responses were assessed using χ2 tests (P<0.05).
This study involved anonymous survey responses and did not include identifiable personal data. It was conducted in accordance with the ethical standards of the institutional research committee and with the 2013 revision of the Helsinki Declaration. Formal IRB approval was not sought, as the study posed minimal risk.
Results
A total of 257 patients (146 male, 111 female; mean age: 38 [range: 18–87]) completed the questionnaire. Key findings included:
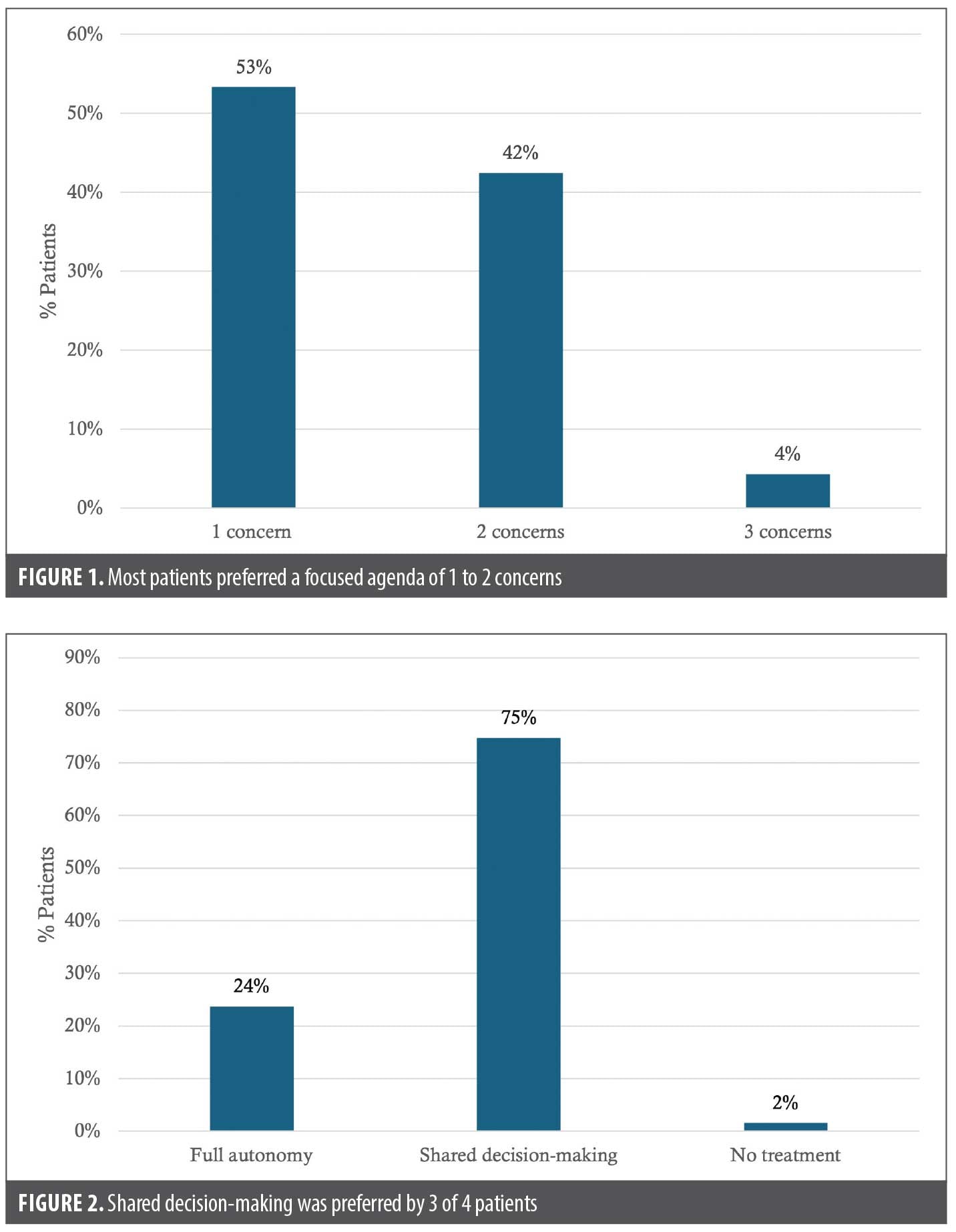
- Scope of visit: 95.7% of patients preferred to focus on 1 or 2 issues during their initial visit (Figure 1).
- Decision-making: 75% favored SDM, while a minority preferred either full autonomy or answers without treatment (Figure 2).
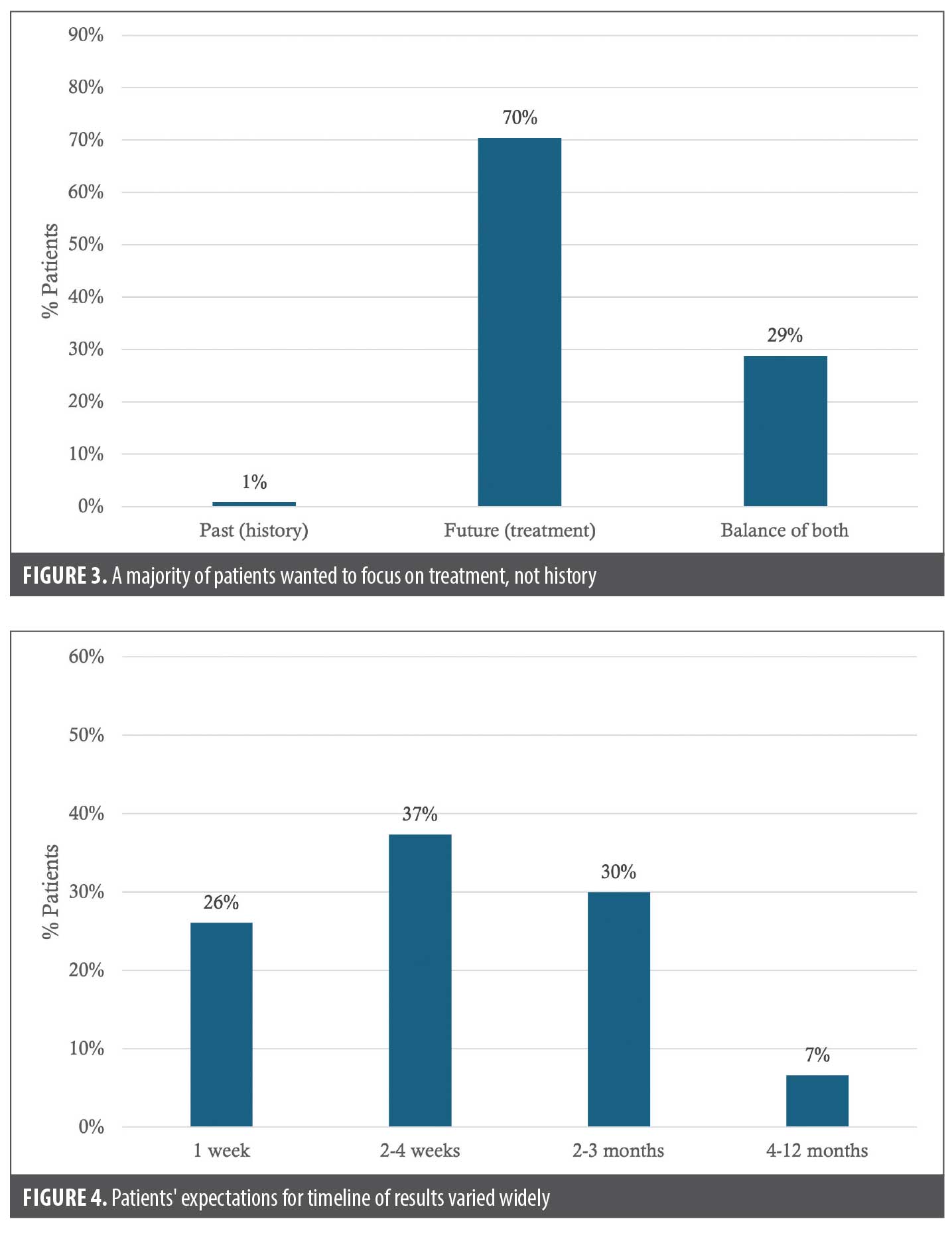
- Consultation focus: 70% prioritized discussing future treatments, while 1% chose to discuss, though many also valued integrating medical history (29%) (Figure 3).
- Outcome expectations: Responses were evenly distributed across projected timelines from 1 week to 12 months (Figure 4).
Notable associations emerged:
- Scope vs style: Patients who aimed to address multiple concerns were significantly more likely to prefer autonomous decision-making (χ2=24.0; P<0.001).
- Sex differences: Women were more inclined to discuss multiple concerns (χ2=29.6; P=0.0003) and to balance discussion between history and treatment (χ2=24.0; P=0.0023). Men more often focused on a single concern and prioritized treatment discussions alone.
- Expectation timelines: Men most often expected results in 2 to 3 months, while women were split between short (2–4 weeks) and long (4–12 months) expectations (χ2=22.1; P=0.037).
Discussion
Our findings reinforce a central insight in contemporary dermatology: while SDM has reshaped the clinical landscape, true patient-centered care requires understanding how patients want to participate, not just that they should. Most patients in our study preferred to tackle a focused agenda of 1 or 2 concerns while favoring collaborative involvement in treatment decisions. These preferences suggest that SDM is not a one-size-fits-all approach but a framework that must flex to fit individual cognitive and emotional needs.
The widespread adoption of SDM marked a necessary evolution away from traditional paternalism in medicine. Research has consistently shown that SDM improves patient satisfaction, treatment adherence, and even clinical outcomes.2,3 However, as our data show, not all patients seek the same level of engagement or guidance. Some prefer decisional autonomy, particularly when discussing multiple concerns, while others prioritize reassurance or information. This echoes work in mental health and internal medicine that highlights how decision-making preferences are shaped by psychological state, trust in the provider, and perceived complexity of care.4,5
Sex-based differences in our cohort—such as women being more likely to prefer multitopic visits and a balance between history and treatment—align with literature showing that women often engage more relationally in clinical encounters.6 Interestingly, age did not predict preferences, suggesting a cultural shift where patient autonomy and collaborative care are now normative expectations across generations.7
While SDM has rightly been celebrated, there is increasing recognition of the gray zone between autonomy and guidance. The concept of selective paternalism—where clinicians adapt their level of persuasion based on context and patient vulnerability—has been proposed as a way to ethically support patients without overriding them.8,9 Indeed, multiple studies have shown that some patients, especially in high-stress or low-literacy scenarios, may prefer a more directive style.10,11 Our results suggest that such preferences can also be inferred by visit scope and decision fatigue.
Beyond the statistical insights, we observed consistent and unsolicited positive feedback from patients about the survey itself. Many described it as calming, clarifying, and helpful in setting the tone for their visit. Patients frequently noted that the questions reduced anxiety by giving structure to what can otherwise feel like an ambiguous or rushed experience. Several remarked that the process helped them better understand their own goals and decision-making style. This qualitative response reinforces the survey’s dual utility as both a clinical tool and a patient-centered intervention in its own right.
Integrating brief decision-style surveys like ours may help clinicians tailor their communication strategies in real-time, setting clear expectations and reducing the emotional friction that often leads to dissatisfaction. This approach does not negate SDM; it enhances it by making the process itself collaborative and responsive. From the provider’s perspective, dermatologists consistently support SDM but face common barriers in practice including consultation time, patient misconceptions, and indecision.12 Our 4-question framework is a practical, workflow-friendly tool that directly addresses these concerns. It is brief, requires no specialized training, and offers immediate insight into patient preferences to structure visits effectively reducing clinician burden.
While implementing new clinical tools can often be perceived as an additional administrative burden, our experience in a high-volume dermatology practice demonstrates that this 4-question framework actually enhances clinic efficiency. To minimize workflow disruption, the survey is best administered via the patient portal previsit or on paper immediately after the medical assistant rooms the patient; we found the latter particularly effective, as it reduces the patient’s perceived waiting time for the provider. A brief, 30-second review of the results prior to or upon entering the room allows the clinician to immediately frame the encounter according to the patient’s cognitive style. Establishing priorities early prevents agenda creep, the common clinical phenomenon where additional concerns are raised at the end of a visit. Furthermore, by encouraging a focus on 1 or 2 prioritized concerns with scheduled follow-ups for secondary issues, this framework aligns with the current state of scheduling and reimbursement constraints in most clinics.
As we seek to refine dermatologic care, the next frontier lies not only in choosing the right treatment but in codesigning the decision-making process itself. Future work should explore whether matching communication styles to patient preferences improves adherence, satisfaction, or outcomes. Our single-network setting and modest sample size are limitations, but the trends observed here support a broader call: patient-centered care must account not just for what patients want but for how they want to engage.
References
- Cline A, Gomolin T, Safai B. Factors influencing patient satisfaction in dermatology. SKIN J Cutan Med. 2020;4:543–547.
- Tan J, Linos E, Sendelweck MA, et al. Shared decision making and patient decision aids in dermatology. Br J Dermatol. 2016;175(5):1045–1048.
- Barry MJ, Edgman-Levitan S. Shared decision making–the pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–781.
- Eliacin J, Salyers MP, Kukla M, Matthias MS. Factors influencing patients’ preferences and perceived involvement in shared decision-making in mental health care. J Ment Health. 2015;24(1):24–28.
- Kassirer S, Levine EE, Gaertig C. Decisional autonomy undermines advisees’ judgments of experts in medicine and in life. Proc Natl Acad Sci U S A. 2020;117(21):11368–11378.
- Roter DL, Hall JA. Doctors Talking with Patients/Patients Talking with Doctors: Improving Communication in Medical Visits. 2nd ed. Praeger Publishers/Greenwood Publishing Group; 2006:xvi, 238.
- Kilbride MK, Joffe S. The new age of patient autonomy. JAMA. 2018;320(19):1973–1974.
- Drolet BC, White CL. Selective paternalism. AMA J Ethics. 2012;14(7):582–588.
- Aggarwal A, Davies J, Sullivan R. “Nudge” in the clinical consultation – an acceptable form of medical paternalism? BMC Med Ethics. 2014;15(1):31.
- Bailoor K, Valley T, Perumalswami C, et al. How acceptable is paternalism? A survey-based study of clinician and nonclinician opinions on paternalistic decision making. AJOB Empir Bioeth. 2018;9(2):91–98.
- Murgic L, Hébert PC, Sovic S, Pavlekovic G. Paternalism and autonomy: views of patients and providers in a transitional (post-communist) country. BMC Med Ethics. 2015;16(1):65.
- van der Kraaij GE, Vermeulen FM, Smeets PMG, Smets EMA, Spuls PI. The current extent of and need for shared decision making in atopic dermatitis and psoriasis in the Netherlands: an online survey study amongst patients and physicians. J Eur Acad Dermatol Venereol. 2020;34(11):2574–2583.