J Clin Aesthet Dermatol. 2026;19(5):57–62.
by Victoria Garfinkel, BSA, and Kaveh Nezafati, MD
Ms. Garfinkel is with Medical School, University of Texas Southwestern Medical Center, Dallas, Texas. Dr. Nezafati is with the Department of Dermatology, University of Texas Southwestern Medical Center, Dallas, Texas.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
ABSTRACT: OBJECTIVE: To evaluate whether a 3-part dermatology-specific curriculum improves resident competency in process mapping, root cause analysis, and adverse event disclosure. METHODS: A pre-post educational intervention study was conducted in 2025 across 3 ACGME-accredited dermatology residency programs affiliated with a Texas-based academic medical center. The curriculum consisted of 3 sequential 1-hour sessions covering patient safety fundamentals, quality improvement tool application via flipped classroom, and peer-led adverse event disclosure simulation. Primary outcomes measured self-reported confidence in systems analysis, root cause analysis, and disclosure communication using 5-point Likert scales. Secondary outcomes assessed the knowledge of dermatology-specific error types and disclosure components. Twenty-seven residents completed pre-intervention surveys and 20 completed post-intervention surveys. Data were analyzed using Mann-Whitney U test and Fisher exact test. RESULTS: Residents demonstrated significant improvements across all primary competencies. Median confidence in process mapping increased from 1 to 4 (P<0.001), fishbone diagramming from 2 to 4 (P<0.001), and adverse event disclosure from 3 to 4 (P=0.001). Knowledge of common outpatient dermatology error types improved from 7.4% to 60% correct responses (P=0.00019). No significant differences were observed by postgraduate year level. Postcourse evaluations showed 95% rated duration as appropriate and 100% reported improved knowledge. LIMITATIONS: Study limitations include reliance on self-reported measures, anonymous survey design precluding paired analysis, modest sample size, lower postintervention response rates with potential volunteer and nonresponse bias due to voluntary participation, and single-institution implementation without long-term follow-up assessment; the curriculum was locally developed without external funding or institutional support that influenced its design or implementation. CONCLUSION: This dermatology-specific curriculum significantly improved resident competencies in systems analysis, root cause analysis, and adverse event disclosure. The specialty-focused design and scalable peer-led simulation model offer a practical approach for adoption across dermatology residency programs. Keywords: Dermatology residency education, patient safety, quality improvement, adverse event disclosure, medical error, process mapping, root cause analysis
Introduction
The Accreditation Council for Graduate Medical Education (ACGME) requires resident education in patient safety, quality improvement (QI), and adverse event disclosure as core subjects across all specialties.1 Despite these universal requirements, dermatology has historically placed less emphasis than other medical specialties on education in these domains.2 A recent national survey of dermatology residency program directors revealed substantial variation in patient safety and QI educational requirements across programs.3 As a result, many residents enter practice without formal instruction in systems analysis or adverese event disclosure. Several structural factors may contribute to this educational gap. Dermatology residencies have fewer core teaching faculty (mean: 10.4; range: 1–29) and smaller resident cohorts (mean: 10) compared to other specialties.4 This structural reality creates variability in the consistency, depth, and delivery of formal educational content across programs. Developing specialty-relevant, practical, and ready-to-use curricula may help address the need for consistent, dermatology-specific patient safety and QI education.
Additionally, increasing education in patient safety and QI can improve the safety and quality of care delivered to dermatology patients. This training may also prepare graduates to participate in multispecialty teams and institutional committees, strengthening dermatology’s contribution to health systems and healthcare delivery. Given these potential benefits, there remains a need for structured, scalable educational interventions that can be feasibly implemented across dermatology training programs.
To address this content gap, we conducted a needs assessment and focused interviews with residents, dermatology faculty, and clinician-educator faculty in other departments at a large, Texas-based academic medical center. Based on these findings, we developed a curriculum of three 1-hour sessions focused on patient safety, QI, and adverse event disclosure and implemented this 3-hour curriculum across 3 ACGME-accredited dermatology residency programs affiliated with the medical center. The primary aim of this study was to evaluate whether the curriculum improved the residents’ competencies in process mapping, root-cause analysis, and adverse event disclosure. Secondary aims included assessing whether the curriculum increased knowledge of dermatology-specific error types and key components of adverse event disclosure and whether improvements varied by postgraduate year.
Methods
Study design and setting. We conducted a pre-post educational intervention study in 2025 across 3 ACGME-accredited dermatology residency programs affiliated with an academic medical center. The curriculum consisted of three 1-hour sessions delivered sequentially over 3 weeks. Participation was voluntary. The study received approval from the University of Texas Southwestern Medical Center Institutional Review Board (IRB# STU20251002).
Participants. A total of 35 dermatology residents (PGY-2 through PGY-4) across the 3 affiliated programs were eligible to participate. Twenty-seven residents completed the pre-intervention survey and 20 completed the post-intervention survey. Because surveys were anonymous and paired linkage was not required, the primary analyses were conducted using unpaired pre-post comparisons.
Curriculum development and objectives. The curriculum was designed by dermatology faculty with expertise in patient safety and QI, with input from clinician-educator faculty in dermatology and other departments across our institution. Development was informed by established frameworks, including the Institute for Healthcare Improvement (IHI),5 ACGME Milestones,6 the Agency for Healthcare Quality and Research (AHRQ) disclosure framework,7 and American Academy of Dermatology Quality Measures.8 The design emphasized practical application to outpatient dermatology, scalability across programs, and alignment with ACGME and specialty-specific educational priorities. Curriculum slides, scripts, and case questions are provided as Supplementary Materials.
Upon completion of the curriculum, learners were expected to demonstrate 3 key competencies: systems analysis via process mapping for a dermatology-specific workflow, root cause analysis using a cause-and-effect (fishbone or Ishikawa) diagram for a dermatology safety event, and structured adverse event disclosure communication (Table 1).
Secondary objectives included improving knowledge of common outpatient dermatology error types, identifying the components of adverse event disclosure, and examining differences in outcomes by resident training level.
Curriculum structure. The curriculum consisted of 3 sequential 1-hour sessions facilitated by a single faculty member (Table 2).
Session 1: Patient safety fundamentals in dermatology. This introductory session provided foundational knowledge of patient safety principles relevant to outpatient dermatology. This setting presents unique safety considerations distinct from hospital-based fields, including diagnostic delays in skin cancer, biopsy and surgical site errors, breakdowns in communication of results, procedural complications, and adverse outcomes associated with cosmetic interventions. Residents reviewed common outpatient dermatology error types and were introduced to QI tools, including process mapping and root cause analysis diagramming. Emphasis was placed on understanding the 2 most common types of errors in outpatient dermatology: assessment errors and intervention errors.9 Due to the heavy inpatient focus of undergraduate medical education, internships, and transitional year programs, residents in dermatology programs arrive with limited formal patient safety education applicable to outpatient practice. For this reason, the session was positioned early in the academic year to introduce these concepts to PGY-2 residents and allow senior residents to revisit them in the context of their new roles as clinical site leaders and educators. The session also reviewed institutional procedures for confidentially reporting medical errors or patient safety events.
Session 2: Flipped classroom: Application of QI tools and introduction of disclosure concepts. The second session focused on QI skills development and practice, again with an emphasis on outpatient dermatology. A flipped classroom approach was used so participants could transition from knowledge acquisition to hands-on skills practice. To optimize relevance to the types of errors encountered in the dermatology outpatient setting, the QI methodologies of process mapping and root cause analysis (also known as a fishbone or Ishikawa diagram) were introduced and practiced.
In this hybrid session, 45 minutes were allocated for residents to construct process maps and root cause analyses for 2 dermatology-specific safety scenarios. To practice process mapping, a case involving an error in the skin biopsy pathway was used, specifically 2 biopsies that were placed in the incorrect specimen bottle. This pathway, characterized by multiple handoffs and high process complexity, was well suited for examination using process mapping.10 Root cause analysis was practiced for a wrong-site surgical procedure case. Wrong-site surgery is a leading cause of error in dermatologic surgery and can be influenced by a variety of factors, making it an ideal scenario for root cause analysis.11 Both cases were generated and reviewed through focus group discussions with practicing dermatologists to ensure alignment with real-world clinical practice.
The last 15 minutes of the session introduced core principles in adverse event disclosure, including preparation for disclosure conversation, appropriate body language and word choice, and logistical considerations. The session concluded with a review of an outpatient dermatology specific disclosure checklist adapted from the AHRQ.
Session 3: Peer-led adverse event disclosure simulation. The final session focused on developing communication skills for adverse event disclosure through peer-led simulation. Effective communication following an unanticipated outcome supports patient trust, aligns with ethical standards, and may reduce medicolegal risk.12–15 Empathetic communication has been shown to decline during undergraduate medical education and residency.16,17 Participation in simulation-based training improves residents’ graded performance, completion of key disclosure tasks, and confidence in adverse event disclosure.18,19 Peer-led simulation, in which learners rotate between the roles of physician, patient, and observer, allows for experiential learning and fosters empathy by allowing residents to assume the role of the patient and more deeply consider the ramifications of an adverse event.12,16 ,20
Due to the smaller size of dermatology programs, access to formal simulation centers and standardized patients may be limited by financial and time constraints. Some programs may have no access to these resources, and others may only have a limited number of simulation hours. Peer-led simulations and peer-led debriefs, which have been demonstrated to increase learners confidence in nontechnical tasks, can serve as an alternative or complement to formal simulation center experiences when access is limited or unavailable.21,22
Simulations were conducted in existing dermatology clinic space and used 2 dermatology-specific cases: delay of results communication and exuberant local reaction. These cases were similarly created using feedback from a focus group of practicing dermatologists to ensure generalizability to outpatient dermatology clinical practice. The session began with a large-group prebrief led by a single faculty facilitator. During the prebrief, simulation principles and psychological safety were reviewed, the 2 cases were introduced, and the disclosure checklist was discussed. Residents then rotated through the roles of physician, patient, and observer. After each case, residents engaged in brief peer-led feedback followed by a large-group debrief facilitated by faculty.
Evaluation framework. The evaluation approach was informed by the Kirkpatrick model.23 Primary outcomes aligned with Kirkpatrick Level 2 (Learning), assessing acquisition of skills related to systems analysis, root cause analysis, and disclosure communication. Additional goals included improving dermatology-specific patient safety knowledge (Level 2) and intention or perceived preparedness to apply skills in practice (Level 3). Exploratory analyses examined stratification of results by PGY level.
Outcome measures. The primary outcomes were improvement in 3 competencies, measured using self-reported confidence ratings on a 5-point Likert scale (1=not at all confident; 5=extremely confident). These competencies included (1) systems analysis: ability to design a process map for a dermatology workflow (performing a skin biopsy); (2) root cause analysis: ability to construct a fishbone diagram for a dermatology clinic error (wrong-site procedure); and (3) adverse event disclosure communication: ability to effectively disclose a medical error to a patient. Survey completion was voluntary and anonymous.
Secondary outcomes included knowledge of the 2 most common outpatient dermatology error types (multiple choice), knowledge of key components of an adverse event disclosure (multiple choice), and differences in outcomes by PGY level.
Data analysis. Due to the anonymous survey design and differing response counts, unpaired pre-post analyses were conducted. Medians and interquartile ranges were reported for the Likert-scale outcomes. Between-group comparisons were performed using the Mann-Whitney U test for ordinal variables and Fisher exact test for categorical knowledge outcomes. Statistical significance was defined as P<0.05. Data were analyzed using R software, version 4.3.3 (R Core Team).
Results
Participant characteristics. A total of 35 dermatology residents across 3 ACGME-accredited residency programs participated. Of these, 27 residents completed the pre-intervention survey and 20 completed the post-intervention survey. Pre-intervention respondents included 9 PGY-2, 9 PGY-3, and 9 PGY-4 residents; post-intervention respondents included 7 PGY-2, 8 PGY-3, and 5 PGY-4 residents.
Participants reported very limited prior experience in QI teaching, simulation activity participation, and low levels of awareness of institutional resources for reporting patient safety events (Table 3).
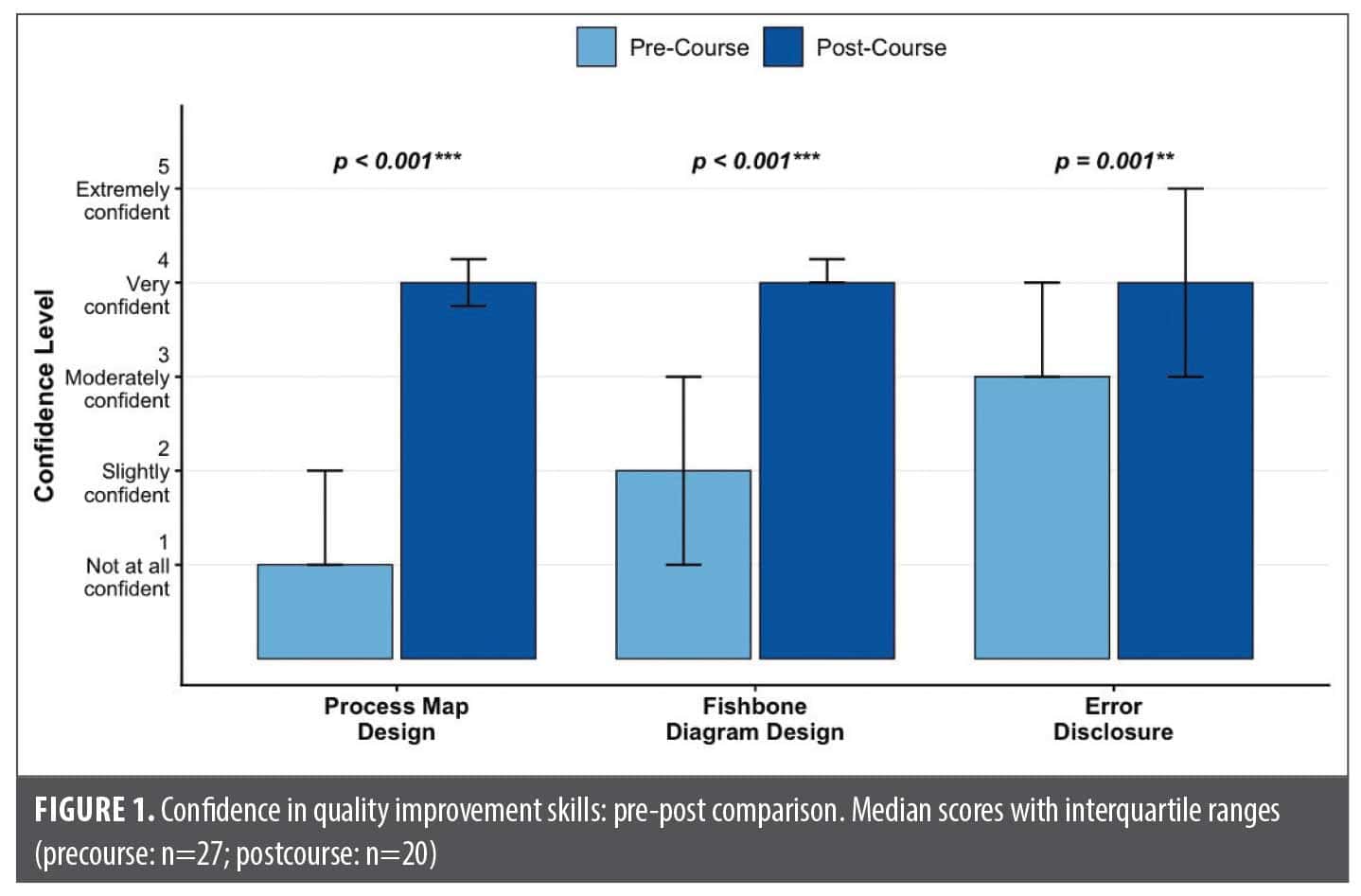
Primary outcomes. Our primary outcome was increasing competency through unpaired analysis of pre- and postintervention survey results (Figure 1).
Systems-analysis competency (process mapping). Residents’ confidence in their ability to design a process map for a dermatology workflow improved significantly following the curriculum. Median confidence increased from 1 (not confident at all) pre-intervention to 4 (very confident) post-intervention (P<0.001), demonstrating a substantial increase in systems-analysis competency.
Root cause analysis competency (fishbone/Ishikawa diagramming). Confidence in constructing a cause-and-effect (fishbone) diagram also significantly increased, from a median of 2 (slightly confident) pre-intervention to 4 (very confident) post-intervention (P<0.001). This reflects a marked improvement in residents’ root cause analysis competency.
Adverse event disclosure communication competency. Residents reported significantly greater confidence in disclosing a medical error to a patient following the curriculum. Median confidence improved from 3 (moderately confident) pre-intervention to 4 (very confident) post-intervention (P=0.001), indicating increased preparedness to engage in patient-centered disclosure conversations.
Secondary outcomes. Knowledge of outpatient dermatology common error types. Knowledge of the 2 most common outpatient dermatology error types (assessment errors and intervention errors) significantly improved following the curriculum. Correct responses increased from 7.4% (2/27 residents) pre-intervention to 60% (12/20 residents) post-intervention (P=0.00019). This represents a substantial knowledge gain in identifying dermatology-specific patient safety risks.
Knowledge of adverse event disclosure components. Knowledge of essential components of adverse event disclosure remained high at baseline and did not significantly change, with 74.1% (20/27) correct responses pre-intervention and 75% (15/20) post-intervention (P=1.0). This suggests strong baseline familiarity with disclosure principles among residents.
Exploratory analysis: PGY subgroup differences. No significant differences were observed across PGY levels at baseline or following the intervention. Kruskal-Wallis testing demonstrated that PGY-2, PGY-3, and PGY-4 residents began the curriculum with similar confidence levels in systems thinking (process mapping; P=0.20), root cause analysis (fishbone diagramming; P=0.52), and adverse event disclosure (P=0.96). Post-intervention scores likewise did not differ significantly by PGY level for process mapping (P=0.36), fishbone diagramming (P=0.40), or disclosure (P=0.34), indicating that residents across all training stages achieved comparable competency levels. These results suggest that the curriculum was uniformly effective and accessible regardless of prior clinical experience or level of training.
Within-group effect size analyses further demonstrated meaningful gains across all PGY cohorts. Each PGY level showed large and statistically significant improvements in systems thinking and root cause analysis competencies, with effect sizes ranging from r=–0.84 to –1.00 for fishbone diagramming and r=–0.96 to –1.00 for process mapping. Improvements in disclosure confidence were most pronounced among PGY-3 and PGY-4 residents; PGY-3 residents demonstrated a statistically significant increase (P=0.020; r=–0.64), while PGY-4 residents showed a large effect size (r=–0.60) that did not reach statistical significance, likely due to smaller sample size. PGY-2 residents showed a modest, nonsignificant increase (r=–0.27). Taken together, these findings indicate robust gains in QI-related competencies across all training levels and highlight a trend toward stronger disclosure skill development as residents progress through training.
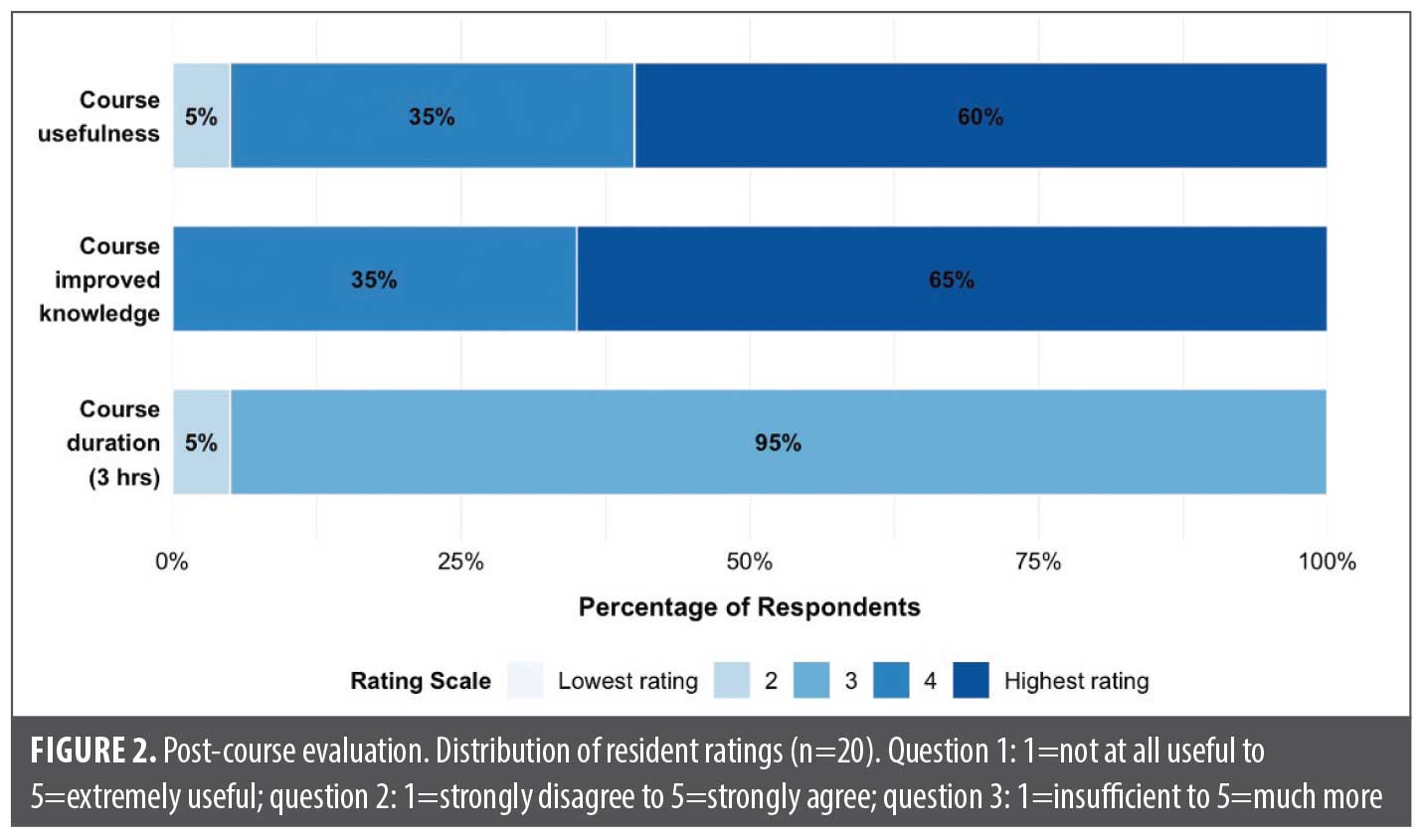
Postcourse evaluation and implementation observations. Postcourse evaluations demonstrated strong resident endorsement of the curriculum (Figure 2). Of respondents, 95% rated the 3-hour duration as appropriate, and all residents rated the course as useful, with 60% selecting “extremely useful.” Similarly, 100% of participants reported that the curriculum improved their knowledge, with 65% marking “strongly agree.” An unintended benefit observed during implementation was that structured reminder emails increased post-intervention survey completion, improving data capture compared to initial projections. However, 7 responses remained incomplete, highlighting the need for strategies to enhance engagement and response rates in future iterations.
Discussion
This 3-part dermatology curriculum significantly improved residents’ competencies across systems analysis, root cause analysis, and adverse event disclosure. Participation led to marked increases in residents’ ability to apply QI methodologies and enhanced preparedness to communicate medical errors to patients—skills essential for safe, transparent, and patient-centered dermatology practice.
The strongest gains were observed in systems analysis and root cause analysis competencies, suggesting that early exposure to practical QI tools fills an important gap in dermatology training. While confidence in disclosure also improved, baseline familiarity with disclosure concepts may have influenced the degree of measurable change. Notably, the curriculum demonstrated benefit across all PGY levels, with no significant differences in post-training competency, supporting its applicability across stages of residency training. Participants felt the course was highly useful and improved their knowledge and felt the 3-hour course structure was ideal.
The curriculum’s effectiveness may be attributed to several key design elements. First, its specialty-specific focus likely increased relevance and engagement to the adult learners. Dermatology-focused cases reflecting common outpatient safety risks—biopsy site labeling errors, wrong-site surgery, breakdowns in result communication and treatment-related adverse events—allowed residents to directly translate learning to their clinical setting. Second, hands-on practice using QI tools in the flipped classroom supported active learning over didactic instruction alone. Finally, the peer-led simulation model enabled residents to practice disclosure conversations in a psychologically safe, realistic environment while offering a scalable approach for programs with limited faculty or standardized patient resources.
These findings fill the ACGME Common Program Requirements and Dermatology Milestones goals of providing education and practice in patient safety, QI, and adverse event disclosure. The selection of instructional strategies for each content area balanced content delivery, hands-on application, and skills practice while using 1 faculty member and resources available to all programs. This curriculum, therefore, fills a key gap and introduces a feasible model for broader dissemination. Final feedback from the learners indicated they felt the course was very useful, improved their knowledge in these content areas, and the time spent was ideal.
Strengths and Limitations
Strengths of this curriculum include its dermatology-specific design; integration of patient safety, QI, and disclosure communication skills; and multiprogram evaluation. Use of the Kirkpatrick model strengthened the evaluation framework, linking outcomes to learner knowledge acquisition and behavioral intention. The peer-led simulation model also supports scalability for resource-limited programs.
Limitations include reliance on self-reported measures, modest sample size, and lower post-intervention response rates, which may reflect the voluntary nature of participation, competing clinical responsibilities, and absence of incentives for survey completion, introducing potential volunteer and nonresponse bias. The anonymous survey design precluded paired pre-post analysis and assessment of long-term impact. To mitigate these limitations, we implemented structured reminder emails to support post-intervention survey completion and stratified analyses by PGY level to reduce potential confounding by training level.
Future Directions
Next steps include incorporating annual refreshers or longitudinal reinforcement, expanding to additional institutions, reviewing longitudinal error reporting data, and piloting the curriculum with interprofessional participants.
Conclusion
This 3-part dermatology-specific patient safety, QI, and adverse event disclosure curriculum significantly improved resident competencies in systems analysis, root cause analysis, and adverse event disclosure. The curriculum’s specialty-focused design and scalable peer-led simulation model make it a practical approach for adoption to other dermatology residency programs.
References
- ACGME Common Program Requirements (Residency). 3 Sep 2025. Accessed 8 Nov 2025. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/cprresidency_2025_reformatted.pdf
- Swary JH, Stratman EJ. Practice gaps in patient safety among dermatology residents and their teachers: a survey study of dermatology residents. JAMA Dermatol. 2014;150(7):738–742.
- Nayudu K, Xiang D, Watson AJ, Nambudiri VE, Shi CR. Patient safety and quality improvement education in dermatology residency programs: a nationwide survey of program directors. Arch Dermatol Res. 2024;316(10):719.
- Data Resource Book, Academic Year 2023–2024. Accreditation Council for Graduate Medical Education; 2024. Accessed 8 Nov 2025. https://www.acgme.org/globalassets/pfassets/publicationsbooks/dataresourcebook2023-2024.pdf
- Institute for Healthcare Improvement. Model for improvement. Accessed 9 Nov 2025. https://www.ihi.org/library/model-for-improvement
- Dermatology Milestones. 2nd rev. Accreditation Council for Graduate Medical Education; 2020. Accessed 9 Nov 2025. https://www.acgme.org/globalassets/pdfs/milestones/dermatologymilestones.pdf
- Disclosure checklist. Agency for Healthcare Research and Quality. Updated Aug 2022. Accessed 9 Nov 2025. https://www.ahrq.gov/patient-safety/settings/hospital/candor/modules/checklist5.html
- Quality measures. American Academy of Dermatology. Accessed 10 Nov 025. https://www.aad.org/member/clinical-quality/measures
- Watson AJ, Redbord K, Taylor JS, Shippy A, Kostecki J, Swerlick Rl. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68(5):729–737.
- Stratman EJ, Elston DM, Miller SJ. Skin biopsy: identifying and overcoming errors in the skin biopsy pathway. J Am Acad Dermatol. 2016;74(1):19–25.
- Strickler AG, Shah P, Bajaj S, et al. Preventing complications in dermatologic surgery: presurgical concerns. J Am Acad Dermatol. 2021;84(4):883–892.
- Wu Q, Jin Z, Wang P. The relationship between the physician-patient relationship, physician empathy, and patient trust. J Gen Intern Med. 2022;37(6):1388–1393.
- Han JL, Pappas TN. A review of empathy, its importance, and its teaching in surgical training. J Surg Educ. 2018;75(1):88–94.
- Hannan J, Sanchez G, Musser ED, et al. Role of empathy in the perception of medical errors in patient encounters: a preliminary study. BMC Res Notes. 2019;12(1):327.
- Shouhed D, Beni C, Manguso N, IsHak WW, Gewertz BL. Association of emotional intelligence with malpractice claims: a review. JAMA Surg. 2019;154(3):250–256.
- Neumann M, Edelhäuser F, Tauschel D, et al. Empathy decline and its reasons: a systematic review of studies with medical students and residents. Acad Med. 2011;86(8):996–1009.
- Hojat M, Vergare MJ, Maxwell K, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med. 2009;84(9):1182–1191.
- Aubin J, Rivolet O, Taunay AL, Ragot S, Ghazali DA, Oriot D. Benefit of simulation-based training in medical adverse events disclosure in pediatrics. Pediatr Emerg Care. 2022;38(2):e622–e627.
- Newcomb AB, Liu C, Trickey AW, Dort J. Tell me straight: teaching residents to disclose adverse events in surgery. J Surg Educ. 2018;75(6):e178–e191.
- Rasasingam D, Kerry G, Gokani S, Zargaran A, Ash J, Mittal A. Being a patient: a medical student’s perspective. Adv Med Educ Pract. 2017;8:163–165.
- He X, Rong X, Shi L, et al. Peer-led versus instructor-led structured debriefing in high-fidelity simulation: a mixed-methods study on teaching effectiveness. BMC Med Educ. 2024;24(1):1290.
- Jaffrelot M, Boet S, Floch Y, et al. Learning with our peers: peer-led versus instructor-led debriefing for simulated crises, a randomized controlled trial. Korean J Anesthesiol. 2024;77(2):265–272.
- Kirkpatrick DL. Evaluating Training Programs: The Four Levels. Berrett-Koehler Publishers; 1994.