J Clin Aesthet Dermatol. 2025;18(12):30–33.
by Daniel P. Friedmann, MD, FAAD; Isabella Martingano, BA; Nabeel Ahmad, MSEd; Michelle B. Tarbox, MD, FAAD; and Kritin K. Verma, MBA
Dr. Friedmann is with the Westlake Dermatology Clinical Research Center at Westlake Dermatology and Cosmetic Surgery in Austin, Texas. Ms. Martingano and Mr. Ahmad are with the Tilman J. Fertitta Family College of Medicine at the University of Houston in Houston, Texas. Dr. Tarbox is with the Department of Dermatology at Texas Tech University Health Sciences Center in Lubbock, Texas. Mr. Verma is with the Texas Tech University Health Sciences Center School of Medicine in Lubbock, Texas.
FUNDING: No funding was provided for this article.
DISCLOSURES: Dr. Friedmann is a consultant and clinical research investigator for Lumenis Ltd. Ms. Martingano, Mr. Ahmad, Dr. Tarbox, and Mr. Verma have no disclosures to declare.
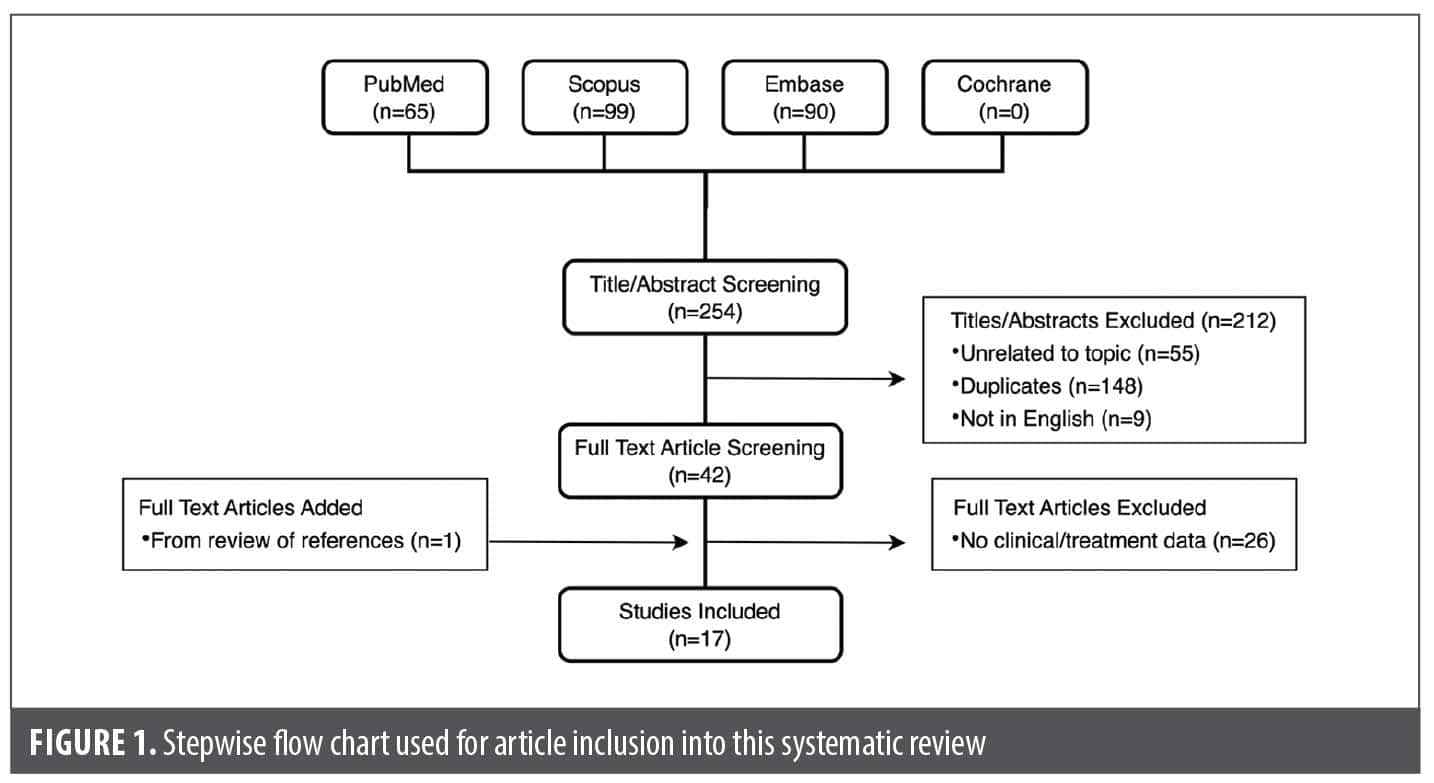
ABSTRACT: Objective: Because pearly penile papules (PPP) are common, asymptomatic, and benign lesions that are often cosmetically bothersome to patients, we sought to systematically review all available treatment options for PPP. Methods: PubMed, Scopus, Embase, and Cochrane databases were queried with relevant terms, with all articles describing treatment modalities for PPP included in this review. Articles related to PPP but lacking treatment information or without novel clinical or patient data, unrelated to PPP, or not available in English were excluded. Results: The database query yielded 254 unique articles. After screening and evaluation for duplicates and inclusion and exclusion criteria, 17 publications, all of which were retrospective case reports or case series, with 142 patients were included and analyzed. The most common modality used was ablative laser (10 articles), eight of which involved carbon dioxide laser, as well as erbium yttrium-aluminum-garnet (YAG) and holmium:YAG lasers. Liquid nitrogen (3 articles) and single reports of pulsed dye laser, nonablative 1550nm fractional laser resurfacing, and electrocoagulation with or without 30% trichloroacetic acid peel were also found. Most articles reported complete lesion removal and high patient satisfaction with no reports of infection or scarring. Limitations: This review is primarily limited by publication bias, with variable or limited methods of reporting efficacy/response and adverse event data. Conclusion: Multiple modalities can achieve safe and effective treatment of PPP with high patient and provider satisfaction. Keywords: Pearly penile papules, angiofibromas, corona of glans penis, CO2 laser, erbium:YAG laser
Introduction
Pearly penile papules (PPP) are small, 1-3mm monomorphous papules that are dome-shaped to papilliform in appearance and typically found circumferentially in rows along the corona of the glans penis.1 They are histologically consistent with acral angiofibromas.1 PPP lesions are common, with a prevalence of 17.2% in a recent cross-sectional study of 2613 men at a dermatology clinic,2 but prevalence may be as high as 48% in the genitourinary clinic setting.3 Commonly developing during or after puberty and with decreasing prevalence and incidence with age, PPP prevalence may also be higher in uncircumcised men compared to uncircumcised counterparts (22.7% vs. 14.3%).4,5 Asymptomatic and benign, they may nevertheless cause psychological distress and embarrassment, prompting some patients to seek treatment.6 Moreover, patients (and rarely healthcare providers) may confuse them with sexually transmitted infections (STI); in fact, 25% of patients seen at a Nepalese dermatology clinic with concern of an active STI had PPP.7
Although a prior systematic review of laser therapy for PPP has been reported,8 no systematic review of all available treatment options for this common condition has yet to be performed.
Methods
This was a retrospective systematic review of published literature. On April 23, 2024, the first author (D.P.F.) conducted an online query of PubMed, Scopus, Embase, and Cochrane databases. The respective searches were performed using the following combination of keywords and Boolean search operators: “penile pearly papules” OR “pearly penile papule” OR “pearly penile papules”. All articles published before the search date were evaluated for inclusion. Studies related to PPP were selected based on their titles and abstracts and subsequently obtained and read for pertinence by the first 2 authors. Deduplication was performed with software (EndNote, Clarivate) and manual assessment.
All articles describing treatment modalities for PPP were included in this review. Excluded studies were those unrelated to PPP, related to PPP but lacking treatment information, without novel clinical or patient data (reviews, commentaries, consensus papers, techniques, anatomical studies, or corrections), or not available in English. The first 2 authors unanimously agreed on the final selection of studies included in this review.
Results
Our searches of the PubMed, Scopus, Embase, and Cochrane databases yielded 254 unique articles (Figure 1). Of those, 42 were retained upon assessment of their titles and abstracts, and following full-text review, 17 publications were ultimately selected for inclusion in this systematic review, including one publication3 added from a review of references (Table 1). All included articles were retrospective (case reports or case series), single-center studies published between 1989 and 2021.
Patient demographics. A total of 142 male patients were reported, with a mean age of 27.1 years (SD: 5.7 years; range: 18-52). Four studies3,9,21,24 did not report age-related data. No publication had a comparative control arm. Nearly all involved classic lesions along the corona (94.1%), while 1 publication20 reported therapy of ectopic lesions of the shaft. The majority (82.4%) did not report circumcision status, but of the 3 studies10,11,15 where this was reported, 90.9% (20 of 22) were uncircumcised prior to lesion development. Fitzpatrick skin type was explicitly reported in only 4 publications12,13,17,24 with 8 patients. Time of lesion onset was listed as “since puberty” in 4 studies9-11,21 and between ages 9 to 23 years in 3 studies,13,19,22 albeit not reported in 10 articles.
Pretreatment protocol. The use of a pre-treatment disinfectant was discussed in only 1 report,14 with the use of a 0.1% octenidine/2% phenoxyethanol topical applied immediately prior to laser therapy.
Pre-treatment local anesthesia was described in 13 publications (76.5%), including topical anesthetic agents (7 of 13; 53.8%),12,14-16,18,19,23 1% to 2% lidocaine injection infiltration without epinephrine (6 of 10; 60.0%),3,9,11,13,17,23 2% lidocaine ring block at the penile base (1 of 10; 10.0%),10 and ice application (1 of 10; 10.0%).13 Lidocaine injection was combined with ice13 or topical anesthetic ointment23 in one publication each. The type of topical anesthetic varied significantly, including lidocaine/tetracaine cream (7%/7%, 6%/6%, or 23%/7%),15,18,19 lidocaine/prilocaine cream (2.5%/2.5%),16 lidocaine cream (9%),14 lidocaine gel (30%),12 or undetailed lidocaine ointment.23 Only 2 publications12,19 reported applying topical anesthetic under occlusion. Only 1 report17 performed treatment under intravenous sedation (propofol), albeit in combination with local lidocaine infiltration. No topical anesthetic was used in 4 publications.20-22,24
Treatment modalities and efficacy. The weighted mean number of treatments across all modalities was 1.74 years (SD: 0.54 years; range: 1-6), with 6 studies3,9-11,13,24 having only one treatment session. Weighted mean interval between treatments for studies with multiple sessions was 4.34 weeks (SD: 3.95 weeks; range: 2-24) weeks apart, although one study23 did not report the treatment interval. Complete response was seen in 125 of 142 patients (88.02%), with partial and no response in 16 (11.27%) and 1 (0.70%), respectively.
The most common modality was ablative laser (10 articles), of which carbon dioxide (CO2) laser was the most often used (8 of 10; 80%) in either pulsed (7 of 8; 87.5%)3,9,10,12-15 or continuous wave modes (2 of 8; 25%).10,11 Weighted mean number of CO2 treatment sessions was 1.82±0.53 (range: 1-3). Treatment settings varied widely and are described in detail in Table 1. Erbium:YAG 2940-nm laser was used in the largest number of patients (n=45) in a single case series,16 while holmium:YAG 2100-nm laser use was also reported in a case series.17 Eight publications with ablative laser demonstrated complete lesion removal, with only 2 (both with pulsed CO2) reporting a partial or incomplete response.13,14
The use of nonablative 1550-nm fractional resurfacing (NAFR) in 1 publication18 produced a complete response, albeit after 5 sessions, the largest number of sessions in any publication. A case series of 595-nm pulsed-dye laser (PDL) described complete response in 3 out of 4 patients.19 Case series of electrocoagulation and electrocoagulation combined with 30% trichloroacetic acid (TCA) application demonstrated complete response after a weighted mean of 1.24±0.05 (range: 1-2) sessions. Three reports of liquid nitrogen (6 patients) demonstrated partial21 or complete22 response (with 1 case of treatment failure)20 after a weighted mean of 2.33±0.82 (range: 2-4) sessions.
Posttreatment. A variety of posttreatment wound care regimens were reported. Topical petrolatum ointment was recommended in 4 publications after CO212,13,15 and NAFR.18 Topical antibiotic cream or ointment was used in 3 case series of erbium:YAG, holmium:YAG, and PDL, while a topical antibiotic combined with hydrogen peroxide (H2O2) solution applied twice daily was used in 3 publications after CO29,10 and liquid nitrogen.21 Four publications did not report any form of posttreatment wound care after CO2,3,11 electrocoagulation/30% TCA, or liquid nitrogen.20 Other publications described the combined topical use of betadine solution/depithelializing cream,23 potassium permanganate soak/silver sulfadiazine,16 antibiotic/antiviral creams,14 and steroid/antibiotic/antifungal creams.22 No article described the use of oral antibiotics or antivirals periprocedurally.
Healing times varied significantly, ranging from 3 to 10 days after CO2,12-15 2 weeks after erbium:YAG, and 2-3 weeks after holmium:YAG, as well as 10 days after electrocoagulation/30% TCA and 8 to 10 days after liquid nitrogen.21 Healing times were not reported in 7 publications and were not significant after NAFR or PDL. Only 2 publications14,15 reported explicitly recommending no sexual activity during the healing period.
Safety
There were no reports of post-treatment secondary infection, herpetic reactivation, abnormal sensation, erosion/ulceration, or scarring. Minimal purpura and discomfort were described after PDL, and self-limited capillary bleeding was seen with erbium:YAG laser, CO2,15 and electrocoagulation. One publication also reported minor discomfort and transient hypopigmentation following CO2.15
Discussion
Often causing psychological stress and embarrassment to patients, PPP lesions are often confused with sexually transmitted lesions such as molluscum contagiosum and condyloma acuminata.8 Not surprisingly, 7 patients in 1 article16 had failed prior treatment with liquid nitrogen and topical agents before being treated successfully with erbium:YAG laser. PPP development may be more likely in uncircumcised men, with the vast majority of men (whose circumcision status was reported) being uncircumcised in this review.
The most common modalities for PPP treatment were CO2 laser (8 case studies, 39 patients), erbium:YAG laser (1 case study, 45 patients), and electrocoagulation (1 case study, 44 patients), of which 117 of 128 patients (91.4%) had complete lesion eradication after a weighted mean of 1.70±0.42 sessions. Ablative lasers can produce small spot sizes, leading to pinpoint ablation that preserves intervening unaffected tissue columns, potentially decreasing the risk of complications and shortening healing time compared to wide-field ablation.14 Nevertheless, electrocoagulation, cryoablation (liquid nitrogen), and chemical ablation (TCA peel) also may produce excellent results with low risks. Multiple rounds of selective photothermolysis of hemoglobin within the minute vessels of these angiofibromas using PDL or water within their collagenous structure using NAFR can do the same with extremely low downtime. The lack of scarring in any study is at least in part influenced by the excellent healing capacity of the coronal mucosa, imparting a higher degree of safety for ablative procedures in this region.
This systematic review is limited by publication bias, with variable or limited methods of reporting efficacy/response and adverse event data, particularly because of the included publications being case reports or series without standardized data collection. The variability in approach toward antimicrobial prophylaxis and postcare routine limits the ability to make broad conclusions, but the lack of reports of bacterial or viral infection despite an absence of oral therapy implies that the risk of secondary infection is low.
Conclusion
We present the first systematic review of all available treatment modalities for PPP, highlighting that multiple therapeutic options can achieve safe and effective eradication of PPP lesions with high patient and clinician satisfaction. Randomized prospective studies are necessary to determine optimal treatment modality, device settings, and technique.
References
- Honigman AD, Dubin DP, Chu J, Lin MJ. Management of pearly penile papules: a review of the literature. J Cutan Med Surg. 2020;24:79-85.
- Yildiz H, Demirer Z, Ozmen I. The prevalence of penile pearly papules among young men. Acta Dermatovenerol Croat. 2017;25:46-49.
- Sonnex C, Dockerty WG. Pearly penile papules: a common cause of concern. Int J STD AIDS. 1999;10:726-727.
- Agha K, Alderson S, Samraj S, et al. Pearly penile papules regress in older patients and with circumcision. Int J STD AIDS. 2009;20:768-770.
- Neinstein LS, Goldenring J. Pink pearly papules: an epidemiologic study. J Pediatr. 1984;105:594-595.
- Michajłowski I, Sobjanek M, Michajłowski J, et al. Normal variants in patients consulted in the Dermatology Clinic for lesions of the male external genitalia. Cent European J Urol. 2012;65:17-20.
- Kc S, Adhikary M, Karn D. Clinical scenario of venerophobia in patients presenting in outpatient department. J Nepal Health Res Counc. 2020;18:483-487.
- Maranda EL, Akintilo L, Hundley K, et al. Laser therapy for the treatment of pearly penile papules. Lasers Med Sci. 2017;32:243-248.
- Magid M, Garden JM. Pearly penile papules: treatment with the carbon dioxide laser. J Dermatol Surg Oncol. 1989;15:552-554.
- McKinlay JR, Graham BS, Ross EV. The clinical superiority of continuous exposure versus short-pulsed carbon dioxide laser exposures for the treatment of pearly penile papules. Dermatol Surg. 1999;25:124-126.
- Lane JE, Peterson CM, Ratz JL. Treatment of pearly penile papules with CO2 laser. Dermatol Surg. 2002;28:617-618.
- Gan SD, Graber EM. Treatment of pearly penile papules with fractionated CO2 laser. J Clin Aesthet Dermatol. 2015;8:50-52.
- Krakowski AC, Feldstein S, Shumaker PR. Successful treatment of pearly penile papules with carbon dioxide laser resurfacing after local anesthesia in an adolescent patient. Pediatr Dermatol. 2015;32:433-435.
- Deda A, Lipka-Trawińska A, Wilczyński S, Błońska-Fajfrowska B. CO2 laser treatment for pearly penile papules – personal experience. J Cosmet Laser Ther. 2019;21:152-157.
- Pérez Rivera F. Fractionated CO2 laser treatment for pearly penile papules: evaluation of clinical results and sexual health quality of life improvements. Eur J Plast Surg. 2021;44: 123-128.
- Baumgartner J. Erbium: yttrium-aluminium-garnet (Er:YAG) laser treatment of penile pearly papules. J Cosmet Laser Ther. 2012;14:155-158.
- Lee JA, Larson JS, Kava BR. Preliminary experience in the treatment of pearly penile papules with holmium: YAG laser. JSM Clin Case Rep. 2016;4:1119.
- Rokhsar CK, Ilyas H. Fractional resurfacing for the treatment of pearly penile papules. Dermatol Surg. 2008;34:1420-1422.
- Sapra P, Sapra S, Singh A. Pearly penile papules: effective therapy with pulsed dye laser. JAMA Dermatol. 2013;149:748-750.
- O’Neil CA, Hansen RC. Pearly penile papules on the shaft. Arch Dermatol. 1995;131:491-492.
- Ocampo-Candiani J, Cueva-Rodriguez JA. Cryosurgical treatment of pearly penile papules. J Am Acad Dermatol. 1996;35:486-487.
- Porter WM, Bunker CB. Treatment of pearly penile papules with cryotherapy. Br J Dermatol. 2000;142:847-848.
- Fekete F. Needle electrode coagulation of pronounced pearly penile papules. J Sex Med. 2011;8:466.
- Grada A, Obagi Z. Treatment of pearly penile papules with the use of electrocoagulation followed by 30% trichloroacetic acid localized chemical peel. J Am Acad Dermatol. 2018;79:AB302.