Joshua A. Zeichner, MD
Mount Sinai Medical Center, New York, New York
Disclosure: Dr. Zeichner is a consultant for Promius Pharma.
Abstract
Psoriasis in some body parts can be challenging to treat. Psoriasis in the scalp, palms and soles, and intertriginous areas differ from disease on other body parts, and treatment regimens must be tailored to these areas. The presence of hair, along with the frequent, thick scale of psoriasis makes the scalp a challenge to treat. Skin in the body’s intertriginous areas is often thin, limiting treatment options for inverse psoriasis. Finally, palmoplantar psoriasis is often resistant to topical therapies because of the thickness of the skin. Moreover, cosmetic acceptibilty of a topical medicine is important when treating these areas. Coal tar has been used to treat psoriasis for hundreds of years. In a novel foam vehicle, coal tar 2% is versatile and may be used to treat psoriasis even in challenging areas of the body, such as the scalp, intertriginous areas, and palms and soles. (J Clin Aesthet Dermatol. 2010;3(9):37–40.)
Psoriasis is a chronic, immune-mediated, inflammatory disease affecting two percent of the population—approximately 125 million people worldwide.[1,2] Plaque-type psoriasis is the most common form, affecting 80 percent of psoriasis patients.[2] Treatment selection is determined by the severity and location of the psoriasis as well as medication side effects, patient preferences, and financial constraints.
Psoriasis in certain areas of the body may be a particular challenge to treat. The scalp, palms and soles, and intertriginous areas differ from skin on other body parts, and treatment regimens must be tailored to these areas. The presence of hair on the scalp, along with the frequent, thick scale of scalp psoriasis, interferes with absorption of medications. Also, cosmetic acceptability of topicals is often an issue for patients with scalp psoriasis, as many medications interfere with daily hair grooming.[3] Inverse, or intertriginous, psoriasis involves the body’s skin folds, such as axillary, inframammary, and genital skin. Thin skin and relative occlusion in these areas favor the use of some medications, but limit the use of others. For example, topical steroids must be used cautiously due to an increased risk of cutaneous adverse events.[4] Palmoplantar psoriasis is relatively resistant to even the most potent topical therapies, and patients with this type of psoriasis often suffer from physical disability and discomfort.[5]
Commonly used topical medications for psoriasis include corticosteroids, Vitamin D analog, keratolytics, anthralin, coal tar, and tazarotene. They may be used individually or in various combinations.[6] Careful selection of both class of medication and its vehicle is crucial in the treatment of psoriasis in difficult-to-treat areas. New vehicles provide improved penetration and cosmetic acceptability of medications that previously could not be used.
The following two cases demonstrate the use of topical coal tar 2% foam for the treatment of psoriasis in difficult-to-treat areas. Coal tar 2% foam was effective as monotherapy for both palmoplantar and intertriginous psoriasis and was effective in combination with topical clobetasol emollient foam for scalp psoriasis. Coal tar 2% foam is a versatile and promising treatment for challenging psoriasis cases.
Case 1
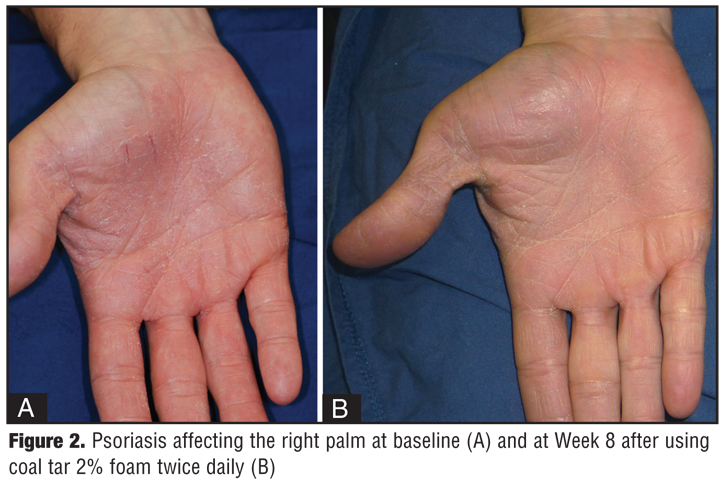
A 31-year-old Caucasian man presented to the clinic for the treatment of long-standing plaque-type psoriasis. On physical examination, he had moderate plaque-type psoriasis on the bilateral elbows, knees, palms, and axillae, affecting approximately six percent of his body surface area. In addition, he had pitting of the finger nails. The patient had no signs or symptoms of arthritis and was otherwise healthy, taking no medications. He had no known drug allergies. Past treatment for his psoriasis included topical steroids and vitamin D analogs. These were efficacious on the elbows and knees and temporarily efficacious on the palms. He stopped treating his palms because he disliked the ointment vehicles of the medications. His major complaint was psoriasis on the palms and axillae. He had used topical calcineurin inhibitors in the past in the axillae, but discontinued them because of burning at the application sites. He was given coal tar 2% foam to use twice daily on the palms and axillae. On follow-up visit at Week 8, the plaques were significantly improved (Figure 1 and Figure 2). The axillae were clear with residual hyperpigmentation, and the palms were almost clear. The patient had no complaints with the coal tar foam. The patient did not report staining of clothing or skin while using the tar foam.
{kind=link}
{kind=link}
Case 2
A 50-year-old Indian woman presented with a lifelong history of plaque-type psoriasis. On physical examination, she had erythematous plaques with silvery white scale on her bilateral extensor elbows and knees as well as the trunk. Similar plaques covered more than 10 percent of her scalp. She was most concerned about scalp involvement and was distressed by both the visibility and pruritus of the lesions. She had no associated arthritis and was otherwise healthy, taking no medications. She had no drug allergies. She was using a combination of betamethasone ointment with calcipotriene ointment with success for body lesions and wished to continue on that regimen. Her scalp disease, however, had been a challenge. For several years, she had been treated with a combination of intralesional corticosteroid injections, topical steroids, and salicylic acid gels and shampoos. The scalp lesions were overall resistant to therapy. She was given coal tar 2% foam to use twice daily in combination with clobetasol in an emollient foam vehicle for two weeks. After two weeks, she started to use the coal tar foam twice daily on weekdays and the steroid foam on weekends. On follow up after two weeks, the plaques were significantly improved with decreased erythema, scale, and plaque thickness. Improvement continued over the next four weeks, and there was no evidence of staining of the hair (Figure 3). The patient additionally reported improved pruritus on the scalp. She had no complaints with the use of the coal tar foam or clobetasol foam.
{kind=link}
Discussion
Tars are resins that have been used as a treatment for dermatological conditions for more than 2,000 years[7] and specifically for psoriasis for more than 100 years.[6] Three main forms of tar exist: wood, shale, and crude coal, the latter of which is most used medicinally. Crude coal tar is distilled from coal and comprises thousands of different compounds. The composition of one preparation may vary from the next depending on the type of coal used and the temperature at which it is heated.[8]
The mechanism of action of coal tar is not well understood. Postulated effects include a suppression of deoxyribonucleic acid (DNA) synthesis and subsequent inhibition of keratinocyte proliferation.[9] Coal tar is thought to help correct the defect of differentiation in keratinocytes of patients with psoriasis. Additionally, it may possess antimicrobial as well as anti-inflammatory and antipruritic effects.[8] Coal tar has been employed as monotherapy for psoriasis or in combination with other topical and systemic agents as well as phototherapy.[10] The use of coal was popularized by its effective use in combination with ultraviolet B (UVB) phototherapy, either as part of the original Goeckerman regimen[11] or in later modified regimens.[8,12,13] The Goeckerman regimen is performed on an inpatient basis and is safe and reliable, even in patients unresponsive to other conventional therapies. Additionally, it results in long-term remissions, as long as 12 months.[14]
Coal tar exists in various preparations including crude coal tar, coal tar ointment, and coal tar solution.[15] These products have been poorly tolerated by patients for several reasons. Cosmetic concerns include staining of the clothing as well as a malodorous tar smell. Medical side effects also occur, such as irritant contact dermatitis, folliculitis, and UVA photosensitivity.[6] While coal tar is not used commonly in the United States, in other parts of the world, such as the Netherlands, it is considered to be first-line therapy.[16]
Coal tar 2% foam (Scytera® Foam, Promius Pharma) is a novel coal tar formulation in a foam vehicle. It is a behind-the-counter product that may be obtained by the patient with a recommendation from the physician, but without a prescription. This formulation differs from previous forms of coal tar in that the emollient foam vehicle spreads easily and dries quickly, with minimal odor from coal tar. In addition, in a foam vehicle, it is versatile and can be used in even difficult-to-treat areas such as the scalp, where hair limits the use of medications in many other vehicles.
Scalp psoriasis affects an estimated 50 to 80 percent of psoriasis patients.17 Severity ranges from mild erythema to thick, scaly plaques covering the entire scalp, and patients commonly complain of pruritus. In addition, lesions may be visible, as they frequently extend beyond the hairline to the forehead, neck, or ears. Scalp psoriasis has a significant impact on quality of life of patients and impacts their social and psychological functions.[5,18] Topical medications are the most frequently used therapies for scalp psoriasis,[19] yet patients are highly dissatisfied overall with these treatments because of their inconvenience and perceived ineffectiveness.[20] Cream and ointment vehicles, for example, are often messy and difficult to apply to the hair-bearing scalp.[20,21] Therefore, medications have been developed in vehicles more appropriate for the scalp, such as shampoos, sprays, and foams. Coal tar has been incorporated in various shampoos and solutions for use on the scalp, which have been used alone or in combination with salicylic acid or a topical corticosteroid, although evidence-based data on their efficacy are lacking.[17]
Intertriginous psoriasis involves the skin folds, such as the axillary, inframammary, and skin. Psoriasis in these areas is common, and symptoms may be exacerbated by friction and perspiration. The mainstay of treatment is the use of low-to-mid potency topical steroids for no longer than 2 to 4 weeks. Caution should be taken as there is a greater potential for local cutaneous side effects of atrophy, striae, and telangiectasias in the skin folds. Additionally, topical vitamin D analogs and calcineurin inhibitors are efficacious in these areas and may be used for longer periods of time.[4] A recent consensus statement from the National Psoriasis Foundation recommends topical tar preparations as second-line therapy, either alone or in combination with a low-potency topical steroid.[4]
Patients with palmoplantar psoriasis often suffer from difficulty and discomfort using their hands and feet for daily activities. While the palms and soles represent a relatively small body surface area, their involvement may lead to severe disease. Palmoplantar psoriasis is often resistant to even potent topical treatment, likely due in part to the thickness of the skin in these areas. Palm and sole disease frequently requires the use of systemic therapies such as acitretin. In addition to traditional systemic agents and biologicals, many medications have been used off label, including colchicine.[5,22] Tars have been used for palmoplantar psoriasis, and 6% crude coal tar ointment under occlusion has been reported to be efficacious.[23] Large clinical studies evaluating tars for palmoplantar disease do not exist.
In conclusion, palmoplantar, intertriginous, and scalp psoriasis are historically difficult-to-treat forms of psoriasis. In the described cases, coal tar 2% foam was used effectively either as monotherapy or in combination with a topical steroid for these areas. Previous tar-containing products have not been widely accepted due to their unpleasant odor and staining of hair, skin, and clothing.[24] However, in these cases coal tar 2% foam did not result in any adverse events. Further investigation is warranted to fully evaluate the efficacy of this new coal tar formulation, but coal tar 2% foam may be a promising addition to the armamentarium of medications available for these challenging patients.
Acknowledgment
The author would like to acknowledge Dan Aversa for his help in preparing this manuscript.
References
1. van de Kerkhof PCM, Franssen MEJ. Psoriasis of the scalp. Diagnosis and management. Am J Clin Dermatol. 2001;2(3): 159–165.
2. National Psoriasis Foundation. About psoriasis: statistics. http://www.psoriasis.org/netcommunity/learn_statistics. Accessed on 1/14/10.
3. Chan CS, Van Vorhees AS, Lebwohl MG, et al. Treatment of severe scalp psoriasis: from the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2009;60(6): 962–971.
4. Kalb RE, Bagel J, Korman NJ, et al. Treatment of intertriginous psoriasis: from the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2009;60(1):120–124.
5. Kragballe K. Management of difficult to treat locations of psoriasis: scalp, face, flexures, palm/soles and nails. Management of Psoriasis, Current Problems Dermatology. 2009;38:166–167.
6. Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 3. Guidelines of care for the management and treatment of psoriasis with topical therapies. J Am Acad Dermatol. 2009.60(4):643–659.
7. Arnold WP. Tar. Clin Dermatol. 1997;15:739–744.
8. Paghdal KV, Schwartz RA. Topical tar: back to the future. J Am Acad Dermatol. 2009;61:294–302.
9. Smith CH, Jackson K, Chinn S, et al. A double-blind, randomized, controlled clinical trial to assess the efficacy of a new coal tar preparation (Exorex) in the treatment of chronic, plaque type psoriasis. Clin Exp Dermatol. 2000;25: 580–583.
10. Pardasani AG, Feldman SR, Clark AR. Treatment of psoriasis: an algorithm-based approach for primary care physicians. Am Fam Physician. 2000;61(3):725–733,736.
11. Goeckerman WH. The treatment of psoriasis. Northwest Med. 1925;24:229–231.
12. Silverman A, Menter A, Hairston JL. Tars and anthralins. Dermatol Clin. 1995;13:817–833.
13. de Rie MA, Out TA, Bos JD. Low-dose narrow-band UVB phototherapy combined with topical therapy is effective in psoriasis and does not inhibit systemic T-cell activation. Dermatology. 1998;196:412–417.
14. Thawornchaisit P. Topical coal tar preparations in the treatment of chronic plaque psoriasis: a review. Clin Dermatol. 2008. Retrieved March 18, 2010 from The Free Library. http://www.thefreelibrary.com/Topical coal tar preparations in the treatment of chronic plaque…-a0190942209.
15. United States Pharmacopeial Convention. The Pharmacopeia of the United States. 17th Revision. New York: Mach Publishing Company; 1965:137–138.
16. Roelofzen J, Aben K, Khawar A, et al. Treatment policy for psoriasis and eczema: a survery among dermatologists in the Netherlands and Belgian Flanders. Eur J Dermatol. 2007;17:416–421.
17. Wozel G. Psoriasis treatment in difficult locations: scalp, nails, and intertriginous areas. Clin Dermatol. 2008;26:448–459.
18. Tan J, Thomas R, Wang B, et al. Short-contact clobetasol proprionate shampoo 0.05% improves quality of life in patients with scalp psoriasis. Cutis. 2009;83:157–164.
19. Papp K, Berth-Jones J, Kragballe K, et al. Scalp psoriasis: a review of current topical treatment options. J Eur Acad Dermatol Venereol. 2007;21:1151–1160.
20. Dubertret L, Mrowietz U, Ranki A, et al. European patient perspectives on the impact of psoriasis: the EUROPSO patient membership survey. Br J Dermatol. 2006;155: 729–736.
21. Feldman SR, Housman TS. Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol. 2003;4:221–224.
22. Halverstam CP, Lebwohl M. Nonstandard and off-label therapies for psoriasis. Clin Dermatol. 2008;26(5):546–553.
23. Kumar B, Kumar R, Kaur I. Coal tar therapy in palmoplantar psoriasis: old wine in an old bottle? Int J Dermatol. 1997;36:309–312.
24. Lebwohl M. A clinician’s paradigm in the treatment of psoriasis. J Am Acad Dermatol. 2005;53(Suppl 1):S59–S69.