Marc A. Bjurlin, DO; Jens Carlsen, DO; Division of Urology, Department of Surgery, Cook County Health and Hospitals System, Cook County Hospital, Chicago, Illinois; Mark Grevious, MD, Division of Plastic Surgery, Department of Surgery, Cook County Health and Hospitals System, Cook County Hospital; Michael D. Jordan, DO, Division of Urology, Department of Surgery, Cook County Health and Hospitals System, Cook County Hospital, Chicago, Illinois; Aisha Taylor, MD, Northwestern University, Department of Urology, Chicago, Illinois; Naveen Divakaruni, DO, Division of Urology, Department of Surgery, Cook County Health and Hospitals System, Cook County Hospital, Chicago, Illinois; Courtney M. P. Hollowell, MD, Division of Urology, Department of Surgery, Cook County Health and Hospitals System, Cook County Hospital, Chicago, Illinois
Abstract
Sclerosing lipogranuloma of the penis results from injection of high viscosity fluid for the purpose of penile augmentation and may have devastating cosmetic and sexual function consequences. Although rare, sclerosing lipogranuloma should be considered in the differential diagnosis of subcutaneous induration or nodules of the male genitalia as it may mimic carcinoma and poses a diagnostic challenge in patients reluctant to admit to injection therapy. Surgical excision with penile reconstruction is the mainstay of treatment. The authors present a case of a 35-year-old Myanmarese man with a sclerosing lipogranuloma of the penis due to injection of mineral oil successfully managed with penile biopsy and excision with split-thickness skin graft phalloplasty and provide a review of the current literature.
(J Clin Aesthet Dermatol. 2010;3(9):41–44.)
Sclerosing lipogranulomas of the penis resulting from injection of high-viscosity, oil-based solutions have been sporadically reported in the international literature, most commonly in Asian, Russian, and Eastern European patients.[1–3] A variety of oils has been injected into the penis with the intent of penile augmentation.[3–5] Most commonly presenting with a gross deformity of the penis, sclerosing lipogranulomas of the penis, also commonly referred to as penile paraffinomas, are often associated with emotional distress, impotence, painful intercourse, or the inability to perform sexual activities.[2,4] Surgical treatment may be technically challenging, but excision of the foreign material with appropriate phalloplasty may give satisfactory long-term results.
In this report, the authors describe a case of sclerosing lipogranulomas of the penis secondary to injection of mineral oil managed by wide excision of the skin and subcutaneous tissue infiltrated by the foreign material along with skin graft phalloplasty as well as provide a review of the current literature.
Case Report
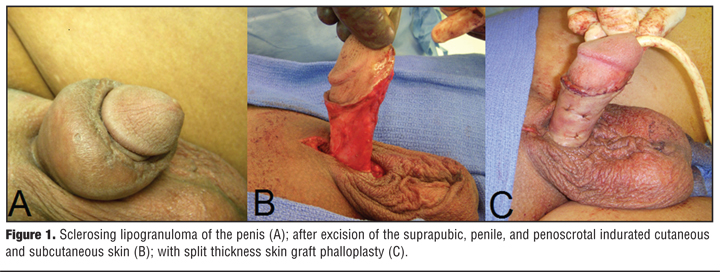
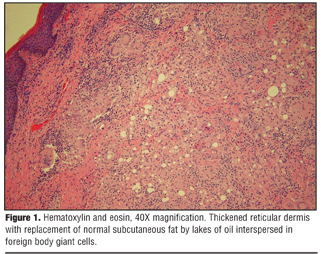
A 35-year-old Myanmarese man presented with a history of repeated injections of mineral oil into the skin and subcutaneous tissue of his penis for the purpose of augmentation one year prior by nonmedical personnel in a Myanmarese coffee house. On presentation, the patient reported a gross deformity of the base of his penis with painful erections and an inability to penetrate during intercourse. His past medical history and surgical history was otherwise unremarkable. The patient had never had any previous penile disease. Physical examination revealed a circumferential subcutaneous ring of indurated tissue at the penile base that extended the entire ventral length of his penis and caused severe deformity (Figure 1A). Induration extended cephalad to the suprapubic fat pad and caudad to the penoscrotal junction, but did not involve the glans penis. The overlying penile skin was fixed and painless on palpation. There was no ulceration, meatal discharge, or inguinal adenopathy, and he denied any lower urinary tract symptoms. Complete blood counts, serum chemistries, urinalysis, and the erythrocyte sedimentation rate were within normal limits. Laboratory tests for sexually transmitted diseases were negative. Cystoscopy demonstrated a normal and patent urethra. Histopathological analysis of a penile biopsy showed thickening of the reticular dermis and replacement of normal subcutaneous fat by lakes of oil interspersed in foreign body giant cells confirming sclerosing lipogranuloma consistent with a paraffinoma Figure 2). Acid fast bacilli and mycology cultures were without growth. An excision of the suprapubic, penile, and penoscrotal paraffinoma (Figure 1B) with split-thickness skin graft phalloplasty was performed (Figure 1C). Postoperatively the patient has a cosmetically acceptable penis with normal erections sufficient for intercourse without pain.
{kind=link}
{kind=link}
Discussion
The practice of injecting high-viscosity, oil-based solutions into the penis resulting in a sclerosing lipogranuloma (paraffinoma) has been sporadically reported in the international literature most commonly in Asian, Russian, and Eastern European patients.[1–3] The first reported case of using paraffin injection in the male genitalia was described by Gersuny in 1899 who injected paraffin for testicular prostheses in a boy who had undergone bilateral orchiectomy for genital tuberculosis.[6]
A wide variety of oils, including paraffin, mineral, silicone, vaseline, motor transmission fluid, cod liver oil, and autologous fat, as well as nandrolone decanoate and mercury, have been injected into the penis with the intent of augmentation.[3–5,7,8] Adverse effects from the injection of oils were reported as early as 1906 when Heidingsfeld described disfiguring subcutaneous nodules in two patients who had received paraffin injections for facial wrinkles.[9] Injections of oil into the genitals (penile or scrotal paraffinoma) have resulted in penile and scrotal deformity, phimosis, skin necrosis, limited erectile function or permanent erectile dysfunction, the inability to have intercourse, abscess formation, and Fournier’s gangrene.[2–4] Despite the long history of these adverse events, oil injections into the penis continue to be performed but are only periodically reported in the dermatology, urology, and plastic surgery literature.[3,4,10]
Paraffinomas result from an injection of a foreign substance containing straight-chain saturated hydrocarbons, such as mineral oil or paraffin. The body lacks the enzymes to metabolize interstitial exogenous oils and consequently a foreign body reaction occurs.[1] Patients commonly present with penile deformity as the oil and subsequent granuloma have the unrestricted ability to spread beyond normal anatomical planes of the genitals.[11] The foreign body reaction manifests in the form of inflammation and induration, edema, scarring, necrosis, deformity, ulceration, painful erections, and, eventually, the inability to achieve sexual activities.[1–3,10] Reactive region lymphadenopthy and gross deformity may lead to clinical confusion with a misdiagnosis of neoplasia and often warrants biopsy.[12,13] These clinical changes may be gradual as paraffinomas can occur several months to years after the injections.[4] In patients who are reluctant to admit they have undergone penile injections, the diagnosis may be clinically challenging. Sclerosing lipogranuloma is used to describe histopathological features including the substitution of normal subcutaneous tissue by cystic spaces of oil. These spaces appear as empty cysts when stained by hematoxylin and eosin. Dense fibrous tissue and granulomatous chronic inflammatory cells, including foreign-body giant cells, encircle these lakes of oil.[4]
Although the use of varying materials for penile augmentation with the aim of restoring and improving body image has been reported, there is little medical literature documenting a safe and efficacious injection material for purely cosmetic genital augmentation.[14] Both Steffens et al and Nyirady et al evaluated the treatment and outcome of a small series of vaseline-induced sclerosing lipogranulomas of the penis and reported pain, phimosis, swelling, and deformity as a common chief complaint.[3,15] All patients in their series warranted surgical excision of the foreign material with penile reconstruction. Liquid silicone has also been used for body restoration and contour with varying success. Although its approved United States Food and Drug Administration indication is only for ophthalmological injections and does not include genital augmentation, silicone injections into the penis and scrotum have been reported with debilitating results.[16,17] Migration of silicone with its disfiguring effects has occurred with augmentation of the breast, face, and penis.[16] In addition to the short-term reactions after subcutaneous silicone injection, including pain, ecchymosis, and pigment alternation, life-threatening adverse events, such as embolism or pneumonitis, have been reported if the silicone is injected directly into the vascular system.[18,19] Recently, Al-Ansari et al reported on the subcutaneous injection of cod liver oil for penile augmentation and determined that the genital complications were more severe with larger amounts of injected oil and with a longer interval period between injection and presentation.[7] In a rare instance, metallic mercury has been injected into the penis, which required total phallectomy and perineal urethrostomy in conjunction with chelation therapy to avoid systemic toxicity.[8]
Motivation to undergo penile augmentation by means of oil injection ranges from the desire to increase penile girth or length, to a perceived increased sense of sexual pleasure, to penis dysmorphic disorder. In a survey of Korean men with penile paraffinomas, Moon et al found that motivation for the penile injection was most commonly driven by recommendations from patient acquaintances.[2] The vast majority of patients in their study (78%) had the procedure performed by nonmedical personnel and nearly 85 percent experienced side effects. Most of the respondents (91%) were not satisfied with their penis after injection and 74 percent replied that they wanted to remove the injected material. Though most men are dissatisfied with the result, those that seek treatment are often embarrassed and hesitant to reveal that they have had penile injections for augmentation.[4]
Definitive treatment of penile paraffinomas includes the aggressive wide excision of skin and subcutaneous tissue infiltrated by the foreign material with appropriate phalloplasty. These operations are complex plastic and reconstructive procedures, time consuming, and, in some cases, difficult to fully treat the first time. A follow-up operation for two-stage repair or because of the development of a complication may be required. Split-thickness skin graft phalloplasty with or without mesh has resulted in a cosmetically acceptable and sexually functional repair.[1,4] Split-thickness skin graft in conjunction with an artificial dermal regeneration plate has also resulted in a robust reconstruction with good aesthetic results.[20] Penile coverage by means of inguinal flaps, free flaps, or native penile skin can result in a successful erectile and functional reconstruction.[21] There commonly exists a plane between the indurated inflammatory tissue and the corporal structures, which often allows for completed excision of affected tissue.[11] While excision of the subcutaneous tissue alone preserves the superficial skin layers, it inevitably leads to necrosis of the epidermis.[3] Patients in whom complete removal of the foreign material may not be possible or those with residual foreign body granuloma may benefit from reconstruction phalloplasty with bilateral scrotal flaps.10 A two-stage procedure may also be employed where the denuded penis is buried in the scrotum in the first stage and penile reconstruction is performed three months later.[3] Treatment with intralesional corticosteroids have also resulted in acceptable outcomes in a few select cases.[12] Failure to fully excise the foreign body may result in recurrence mimicking progressive carcinoma.[13]
Both physicians and their patients need to be made aware of new modalities being used by medical professionals for cosmetic purposes. With respect to penile augmentation, injections of autologous fat or hyaluronic acid gel, grafts of dermal-fat strips, and allograft dermal matrix grafts, as well as the release of suspensory ligaments, are methods currently being investigated. However, this is not the standard urologic practice.[14,22,23]
Conclusion
Sclerosing lipogranuloma of the penis results from injection of high viscosity fluid for the purpose of penile augmentation and may have devastating cosmetic and sexual function consequences. Although rare, sclerosing lipogranuloma should be considered in the differential diagnosis of subcutaneous induration or nodules of the male genitalia as it may mimic carcinoma. Patients should be informed about the disfiguring effects of oil injections into the genitals as they are often injected by untrained persons, do not result in improved satisfaction of the penis, and result in significant side effects, which often leave patients wanting the injection material removed. Management is based on complete excision of the foreign material with organ-preserving phalloplasty, which gives satisfactory long-term results. Physicians caring for patients with genital sclerosing lipogranulomas should be aware of the treatment options and complications of penile augmentation.
References
1. Hohaus K, Bley B, Köstler E, et al. Mineral oil granuloma of the penis. J Eur Acad Dermatol Venereol. 2003;17:585–587.
2. Moon DG, Yoo JW, Bae JH, et al. Sexual function and psychological characteristics of penile paraffinoma. Asian J Andro. 2003;5:191–194.
3. Steffens J, Kosharskyy B, Hiebl R, et al. Paraffinoma of the external genitalia after autoinjection of vaseline. Eur Urol. 2000;38:778–781.
4. Cohen JL, Keoleian CM, Krull EA. Penile paraffinoma: self-injection with mineral oil. J Am Acad Dermatol. 2002; 47:S251–S253.
5. Santos P, Chaveiro A, Nunes G, et al. Penile paraffinoma. J Eur Acad Dermatol Venereol. 2003;17:583–584.
6. Gersuny R. Harte und weiche paraffinprothesen. Zentralbl Chir. 1903;30:1.
7. Al-Ansari AA, Shamsodini A, Talib RA, et al. Subcutaneous cod liver oil injection for penile augmentation: review of literature and report of eight cases. Urology. 2010;75:1181–1184.
8. Oh KH, Park K, Kang TW, et al. Subcutaneous metallic mercury injection for penile augmentation. Urology. 2007;69:e3–e4.
9. Heidingsfeld ML. Histopathology of paraffin prosthesis. J Cutan Dis. 1906;24:513–521.
10. Jeong JH, Shin HJ, Woo SH, et al. A new repair technique for penile paraffinoma: bilateral scrotal flaps. Ann Plast Surg. 1996;37:386–389.
11. O’Rourke MG. Lipogranulomata of male genitalia. J Urol. 1967;39:426–430.
12. Lawrentschuk N, Angus D, Bolton DM. Sclerosing lipogranuloma of the genitalia treated with corticosteroids. Int Urol Nephrol. 2006;38:97–99.
13. Sahin A, Tekgül S, Ergen A, et al. Sclerosing lipogranuloma of the penis. A case report. Int Urol Nephrol. 1991;23:595–598.
14. Kwak TI, Oh M, Kim JJ, et al. The effects of penile girth enhancement using injectable hyaluronic acid gel, a filler. J Sex Med. Epub 2010 Mar 11.
15. Nyirády P, Kelemen Z, Kiss A, et al. Treatment and outcome of vaseline-induced sclerosing lipogranuloma of the penis. Urology. 2008;71:1132–1137.
16. Arthaud JB. Silicone-induced penile sclerosing lipogranuloma. J Urol. 1973;110:210.
17. Wassermann RJ, Greenwald DP. Debilitating silicone granuloma of the penis and scrotum. Ann Plast Surg. 1995;35:505–509.
18. Rodriguezz MA, Matinez MC, Lopez-Artiguezz M, et al. Lung embolism with liquid silicone. J Forensic Sci. 1989;34:504–510.
19. Gurvitus GE. Silicone pneumonitis after a cosmetic augmentation procedure. N Engl J Med. 2006; 357:211–212.
20. Choudhury N, Frame JD, Lewi HJE. Penile paraffinoma and a novel treatment. BJU Int. 2003;92:e14.
21. Santucci RA, Zehring RD, McClure D. Petroleum jelly lipogranuloma of the penis treated with excision and native skin coverage. Urology. 2000;56:331.
22. Caso JR, Myers MD, Wiegand L, et al. Phalloplasty and penile implant surgery. Curr Urol Rep. 2009;10:475–477.
23. Alter GJ. Augmentation phalloplasty. Urol Clin North Am. 1995;22:887–902.