Katherine Fening, MD; Mark Bechtel, MD; Sara Peters, MD; Matthew Zirwas, MD; and Kamruz Darabi, MD
The Ohio State University College of Medicine and Public Health, Division of Dermatology, and
Department of Pathology, Section of Dermatopathology, Columbus, Ohio
Disclosure: Dr. Bechtel is a speaker for and has received honoraria from Steifel. Dr. Zirwas is a speaker for and has received honoraria from Astellas. He is also a speaker and consultant for Coria Labs and receives honoraria from Coria Labs. Drs. Bechtel, Zirwas, Peters, and Darabi are employed by OSU Medical Center. Dr. Fening reports no relevant conflicts of interest.Abstract
Objective: Cutaneous Rosai-Dorfman disease is rare, and there is a lack of literature on clinical evidence for treatment options. The objective of this report is to illustrate that acitretin may be effective in treating cutaneous Rosai-Dorfman disease. Design: A patient with cutaneous Rosai-Dorfman disease refractory to antibiotics, steroids, and surgical excision was treated with acitretin for a period of four months and was closely monitored for improvement in the lesion. Setting: This was a patient in the authors’ medical dermatology clinic. Participants: A single patient was involved. Results: The patient had continuous improvement in her cutaneous Rosai-Dorfman disease throughout a four-month treatment course with softening of the plaque and decreased erythema. She chose to discontinue treatment after four months due to hair loss with acitretin. Conclusion: Cutaneous Rosai-Dorfman disease is a rare, benign, generally self-limited, lymphoproliferative disease of unknown etiology. It typically occurs as histiocyte-rich inflammatory infiltrates, manifesting as red papules and plaques in older women, without predilection for site. Treatment is usually unnecessary, unless the lesions persist and are bothersome to the patient or cause functional deficits. Treatments are based on case reports and include surgery, radiation, and medical options. Our experience with a patient with a case of cutaneous Rosai-Dorfman disease persisting after surgical excision demonstrates that acitretin may be an effective therapeutic option for cutaneous Rosai-Dorfman disease. (J Clin Aesthet Dermatol. 2010;3(9):34–36.)
Rosai-Dorfman disease (RDD) is very rare and exists in two main forms: One form that affects lymph nodes (sinus histiocytosis with massive lymphadenopathy) and rarely extranodal organs, and the other form that is purely cutaneous without systemic or nodal disease. The cutaneous form of RDD is rare and generally self limited. It presents as one or several deep red papules, plaques, or deep nodules that enlarge, persist, or regress and disappear over time. Skin lesions may deeply infiltrate into tissue and cause functional or aesthetic problems to the patient. Characteristic features on skin biopsy include the presence of a mixed superficial and deep inflammatory infiltrate with sheets of large S-100 positive histiocytes and emperipolesis, a process in which leukocytes transmigrate through the histiocyte. Based on case reports and anecdotes, some treatment options have been suggested for patients with persistent or symptomatic disease, with varying efficacy. The authors present a single patient in order to add their experience with acitretin treatment to the literature.
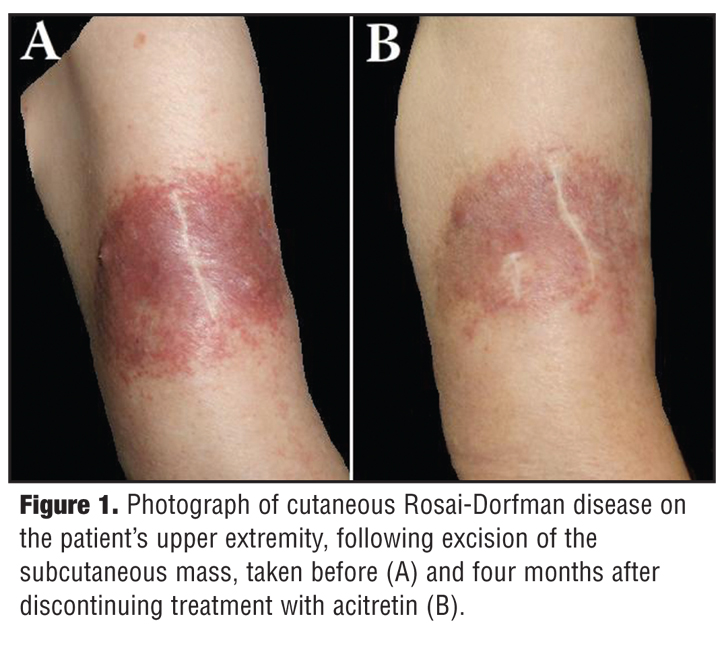
A healthy 82-year-old woman developed a dark red, painless plaque on the right upper extremity over a few months without any associated symptoms or lymphadenopathy (Figure 1A). It had not changed in size over two months, despite treatment with antibiotics and oral glucocorticoids. She had no signs or symptoms of systemic disease and her complete blood count (CBC) was within normal limits.
{kind=link}
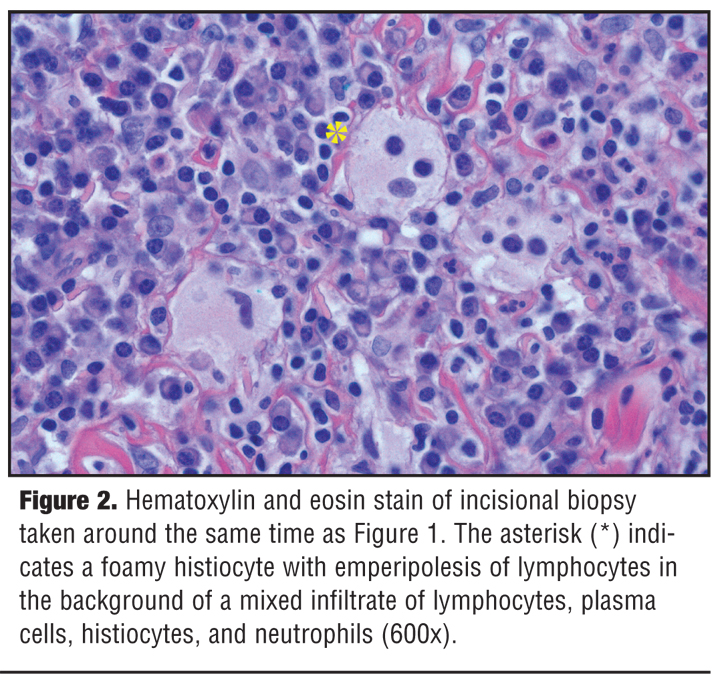
A magnetic resonance imaging (MRI) of the arm, neck, and chest showed edema in the subcutaneous fat and skin overlying the distal deltoid muscle, without lymph node enlargement. Excisional biopsy of the mass revealed a sheet-like proliferation of large, foamy histiocytes with emperipolesis and a pronounced mixed chronic inflammatory cell infiltrate. The histiocytes were S-100 positive by immunohistochemistry and a diagnosis of cutaneous Rosai-Dorfman was made.
She underwent complete excision of the lesion; however, local regrowth was noted over the next 6 to 7 months. A second incisional skin biopsy confirmed the diagnosis of localized cutaneous Rosai-Dorfman disease (CRDD) (Figure 2). After surgical treatment failed, the authors sought medical treatment options and found one case report of CRDD treated successfully with acitretin.[1] The patient was started on acitretin 10mg orally per day with ongoing monitoring of fasting lipids, CBC, and liver function tests. After one month of treatment with slight improvement, the dose was increased to 25mg daily.
{kind=link}
Over the next three months, there was further resolution of the lesion (Figure 1B). On follow-up exam, there was a significant decrease in plaque firmness and reduction of erythema and induration of the subcutaneous tissue. However, four months into treatment, the patient experienced hair loss and dry skin and she chose to discontinue treatment.
Sinus histiocytosis with massive lymphadenopathy, or RDD, is a rare, benign, self-limiting disorder of unknown etiology. It exists in an indolent cutaneous form without systemic symptoms and, a nodal form, which is characterized by massive lymphadenopathy, frequently affecting the cervical lymph nodes with or without systemic symptoms of fever and leukocytosis. Both forms typically follow a benign course and resolve spontaneously. Periodic exacerbations may occur.[2,3]
The purely cutaneous form of the disease, as in our patient, is very rare.[3] While classic RDD is more commonly seen in young adult males, those with CRDD are typically female and older.[1,3] CRDD presents as erythematous to brown papules, plaques, or nodules. There is no predilection for site and patients with CRDD are free from systemic manifestations.[3]
The rarity of CRDD makes randomized clinical treatment trials or large case series impossible and most of our knowledge about treatment is based on single case reports. Various treatments have been described for CRDD. Due to its benign course and spontaneous resolution in most cases, it is suggested that less aggressive options are employed when possible. Though many treatments have been described, no single option is successful in all cases. Surgical excision of the lesions has been shown to be effective in many cases.[4,5] Improvement has also been observed with topical and systemic steroids,[6–8] cryotherapy, local radiation,9 and acitretin.[9] Treatment with dapsone resulted in improvement in a patient refractory to steroids.10 Similarly, thalidomide has also been effective in patients refractory to other treatments.[4,11] Mixed results have been seen with isotretinoin.[4,12,13] Though imatinib mesylate was effective in a case of systemic RDD,[14] it was ineffective in treating CRDD.[15]
The authors’ patient had been treated with oral glucocorticoids without improvement, followed by surgical excision of her bulky subcutaneous disease. After excision, her localized cutaneous disease persisted. The authors treated the patient’s residual disease with acitretin, with significant improvement. Unfortunately, the patient decided to discontinue treatment due to medication side effects, making it impossible to assess whether complete resolution could have been achieved with this regimen. To the authors’ knowledge, there has been only one previous report[1] on the potential effectiveness of acitretin treating CRDD. Acitretin is relatively safe when compared to other treatments and is useful for cutaneous involvement.
Though CRDD is benign and self limited in most patients, it does persist in some patients and may become symptomatic in skin overlying joints or in cosmetically sensitive areas. This case corroborates the only report to date of acitretin in the treatment of CRDD.
References
1. Mebazaa A, Trabelsi S, Denguezli M, et al. Extensively purely cutaneous Rosai-Dorfman disease responsive to acitretin. Int J Dermatol. 2007;46:1208–1210.
2. Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy: a pseudolymphomatous benign disorder: analysis of 34 cases. Cancer. 1972;30:1143–1188.
3. Brenn T, Calonje E, Granter SR, et al. Cutaneous Rosai-Dorfman disease is a distinct clinical entity. Am J Dermatopathol. 2002;24:385–391.
4. Lu CI, Kuo TT, Wong WR, Hong HS. Clinical and histopathologic spectrum of cutaneous Rosai-Dorfman disease in Taiwan. J Am Acad Dermatol. 2004;51(6):931–939.
5. Potts CA, Bozeman AP, Walker AN, Floyd WE. Cutaneous Rosai-Dorfman disease of the forearm: case report. J Hand Surg Am. 2008;33(8):1409–1413.
6. Ohnishi A, Yoshida Y, Yamamoto O. Cutaneous Rosai-Dorfman disease. J Dermatol. 2008;35(9):604–605.
7. Satter EK, Graham BS, Steger JW. Response of cutaneous Rosai-Dorfman disease to topical and intralesional steroids. Br J Dermatol. 2003;149(3):672–674.
8. Rubenstein MA, Farnsworth NN, Pielop JA, et al. Cutaneous Rosai-Dorfman Disease. Dermatol Online J. 2006;12(1):8.
9. Wang KH, Chen WY, Liu HN, et al. Cutaneous Rosai-Dorfman disease: clinicopathological profiles, spectrum and evolution of 21 lesions in six patients. Br J Dermatol. 2006;154(2):277–286.
10. Chan CC, Chu CY. Dapsone as a potential treatment for cutaneous Rosai-Dorfman disease with neutrophilic predominance. Arch Dermatol. 2006;142(4):428–430.
11. Tjiu JW, Hsiao CH, Tsai TF. Cutaneous Rosai-Dorfman disease: remission with thalidomide treatment. Br J Dermatol. 2003;148(5):1060–1061.
12. Chuang YH, Chan HL, Kuo T. Cutaneous Rosai-Dorfman disease: report of a case treated with isotretinoin. Dermatol Sinica. 1997;15:186–193.
13. Chang LY, Kuo TT, Chan HL. Extranodal Rosai-Dorfman disease with cutaneous, ophthalmic and laryngeal involvement: report of a case treated with isotretinoin. Int J Dermatol. 2002;41:888–891.
14. Utikal J, Ugurel S, Kurzen H, et al. Imatinib as a treatment option for systemic non-Langerhans cell histiocytoses. Arch Dermatol. 2007;143(6):736–740.
15. Gebhardt C, Averbeck M, Paasch U, et al. A case of cutaneous Rosai-Dorfman disease refractory to imatinib therapy. Arch Dermatol. 2009;145(5):571–574.