Roger I. Ceilley, MD
Dermatology PC, West Des Moines, Iowa
Disclosure: The author acknowledges the editorial assistance of Dr. Carl S. Hornfeldt, Apothekon, Inc., with funding provided by Ferndale Healthcare.
Abstract
Mature skin is prone to bruising, resulting in a condition known as actinic purpura, characterized by unsightly ecchymosis and purple patches. Similar to other skin conditions, the incidence of actinic purpura increases with advancing age and occurs with equal frequency among men and women. The unsightly appearance of actinic purpura may be a source of emotional distress among the elderly. A new product has been formulated specifically for the treatment of actinic purpura. This product contains retinol, ?-hydroxy acids, arnica oil, ceramides, niacinamide, and phytonadione, which effectively treat actinic purpura by improving local circulation, thickening the skin, and repairing the skin barrier. The objective of this paper is to review the beneficial properties of these ingredients and their respective roles in the treatment of actinic purpura. J Clin Aesthet Dermatol. 2017;10(6):44–50.
In recent years, the incidence of actinic purpura has increased substantially among the older patients in my dermatology practice. Although not a serious condition, its unsightly appearance is a significant cause of anxiety and the principle available treatment has been reassurance that the lesions will eventually resolve. The goal of this paper is to briefly review actinic purpura and describe a new product specifically developed for the treatment of actinic purpura and the prevention of future lesions.
Aging Skin and the Aging Population
Skin aging is a complex process associated with cumulative DNA damage[1] due to intrinsic factors, such as the action of reactive oxygen species,[2] and exogenous factors including exposure to ultraviolet light.[3] The skin becomes thinner and less elastic (solar elastosis),[4] and the barrier function of the skin decreases due to depletion of lipids in the stratum corneum.[5] This fragility syndrome has been termed dermatoporosis.6 Changes in normal skin physiology include increased susceptibility to infection, diminished superficial pain perception, and decreased immune and inflammatory responses.[7]
In addition, the incidence of skin disorders increases with age.8,9 Among patients 65 years of age or older in one study (N=198), all had one or more dermatologic conditions. These included solar lentigines, senile angiomas, xerosis, seborrheic keratoses, varicose veins, and pruritus.[10] Patients 75 years of age or older were more likely to suffer from solar lentigines, clavi, solar keratoses, and onychomycosis.[10] Unfortunately, the overall incidence of skin disorders is likely to increase as the world population continues to age. In the United States, it is estimated that the number of people 65 and older will double from 41 million in the year 2010 to 86 million by the year 2050.[11] Consequently, there will be a substantial increase in age-related dermatologic diseases and conditions in the future.
Actinic Purpura
Mature skin is often prone to significant bruising due to reduction in connective tissue, loss of subcutaneous fat to support the skin structure, flattening of the dermal junction, and effacement of the dermal papillae. The connective tissue of the dermis is no longer able to adequately support the microvasculature. Consequently, minor trauma can rupture blood vessels, leading to extravasation of blood. This age-related condition is called actinic purpura. Also known as senile purpura,[12] solar purpura,[13] traumatic purpura, and Bateman’s disease,[14] it is characterized by unsightly ecchymoses and purple patches on the arms or legs of elderly persons caused by blood extravasation following minor trauma.
Actinic purpura occurs almost exclusively among the elderly population, although it may occasionally occur in younger people. Similar to other skin conditions, the incidence of actinic purpura increases with advancing age and occurs with equal frequency among men and women. One source suggests actinic purpura affects approximately two percent of people 60 to 70 years old, increasing to as many as 25 percent of people in the 90- to 100-year age group. Another suggests actinic purpura affects less than 10 percent of people over 50 years old. It is closely associated with photoaged skin[15] and may be worse among people taking aspirin, nonsteroidal anti-inflammatory drugs, or anticoagulants. Treatment is usually unnecessary and complications are rarely reported.[16] Following extravasation, blood is typically resorbed in 10 to 14 days.[17] Delayed resorption for as long as three weeks may be due to the absence of a normal phagocytic response. Post-inflammatory hyperpigmentation may occur.
Actinic Purpura and Quality of Life
The consequences of photodamaged skin include increased rhytides, pigmentary changes, skin laxity and roughness, and telangiectasias, which may have a negative impact on overall quality of life including interpersonal interactions and self-esteem.[18] Similarly, actinic purpura is a cosmetic condition that can also be associated with significant psychological distress.[12] Its unattractive appearance may lead to aversion by others.[19] While not a dangerous condition, effective treatment of actinic purpura is of great clinical importance for the wellbeing of the elderly patient.
Prior Treatments for Actinic Purpura
Published work describing available treatments for actinic purpura are limited. In one small, double-blind study (N=14), healthy subjects 60 to 80 years old with at least two actinic purpura lesions of approximately equal size on each forearm were enrolled. Subjects were randomized to receive twice-daily treatment with 0.1% retinoic acid cream or non-medicated vehicle on each arm for 16 weeks.[17] After two weeks of treatment, there were fewer lesions on the retinoic acid-treated arm (p<0.05); however, there were no significant differences after that time.
More recently, a small open-label study assessed the effectiveness of human epidermal growth factor for the treatment of actinic purpura when applied twice daily for six weeks (N=6).[12] Ultrasound measurements indicated a mean (SEM) skin thickening of 195.2 (35.7) µm while the mean number of purpuric lesions decreased from 15 (4.6) to 2.3 (0.7) over the same time period.
New Moisturizing Bruise Formula
A new moisturizing bruise product (DerMend®, Ferndale Healthcare) has been formulated specifically for the treatment of actinic purpura. This product contains ingredients that effectively treat actinic purpura by improving local circulation, thickening the skin, and repairing the skin barrier. Each of these ingredients and their known beneficial effects are described in detail below.
Retinol. Numerous studies have demonstrated the beneficial effects of topical retinol, a precursor of retinoic acid. In one study, retinol 0.1% was applied to the skin of healthy women 35 to 55 years old (N=41) every other day for two weeks, then daily for 10 additional weeks. This treatment increased epidermal thickness, and upregulated genes for collagen type 1, and collagen type 3 with corresponding increases in procollagen I and procollagen 3 protein expression and a significant reduction in facial wrinkles.20 Similarly, the topical application of 0.1% retinol in another study increased keratinocyte proliferation and epidermal thickness and improved major signs of skin aging.[21]
A 52-week, double-blind, vehicle-controlled study demonstrated the ability of a retinol 0.1% formulation to significantly improve the appearance of photodamaged skin including a 44-percent improvement in lateral canthal fine lines and an 84-percent improvement in the appearance of mottled skin.[22] Histology studies demonstrated increased expression of type 1 procollagen, hyaluronan, and Ki67, a marker for cell proliferation. When combined with a vitamin C-containing moisturizer, the application of topical retinol 0.1% for 12 weeks improved the appearance of women with mild-to-moderate hyperpigmented and photodamaged facial skin.[23]
While no study has assessed the effects of retinol for the treatment of actinic purpura, the combination of topical 0.3% retinol and 1% vitamin K shortened the duration of laser-induced purpura when applied for two weeks prior and two weeks after undergoing treatment with a pulsed dye laser.[24]
Alpha hydroxy acids. DerMend contains glycolic compound 4.4, a combination of glycolic acid and ammonium glycolate. Products containing the ?-hydroxy acids glycolic acid and lactic acid and the b-hydroxy acid salicylic acid have been used for treating cosmetic skin conditions, such as seborrheic keratoses, melasma, actinic keratoses, and verrucae vulgares, and the rejuvenation of photoaged skin, for many years.[25],[26]
In vitro studies have shown that dermal fibroblasts grown in the presence of glycolic acid for 24 hours resulted in increased collagen production.[27] Clinically, measured improvements in skin quality include decreased skin roughness, skin dryness, discoloration, solar keratoses, and overall pigmentation, increased collagen I and procollagen I, and improved quality of elastic skin ?bers.[25],[28],[29] The long-term use of an a-hydroxy acid-containing product resulted in significant clinical improvements in facial skin tone and fine wrinkling, which were associated with psychosocial benefits.[30]
Arnica oil. Arnica oil is derived from the medicinal plant Arnica montana L. Extracts of A. montana are rich in flavonoids and phenolic acids and demonstrate antioxidant activity in vitro and protection against oxidative damage in fibroblast-like cells.31 The topical application of an A. montana-containing gel demonstrated beneficial effects on experimental wound healing in an animal model32 and an A. montana-containing ointment improved pulsed-dye laser-induced bruising in human volunteers.[33]
Ceramides. The barrier function of the stratum corneum is dependent on the presence of a lipid matrix that includes the epidermal sphingolipid ceramides.[34],[35] As a result of skin barrier defects, up to 75 percent of elderly patients are affected by xerosis.[36] Ceramides also play a role in the differentiation of keratinocytes and regulation of cell signaling.[37] DerMend contains a proprietary blend of specifically targeted ceramides (ceramide NP, ceramide NS, ceramide EOS, ceramide EOP, and ceramide AP), and several studies have demonstrated the beneficial effects of this combination of ceramides in mature skin.
Using an in vitro model, the effects of the ceramides phytosphingosine, sphingosine, sphinganine and their hexanoyl-, stearoyl- and salicyl-derivatives were assessed using human keratinocytes.[37] Most of these substances were found to be potent promoters of keratinocyte differentiation. Improvements in skin barrier function have been demonstrated following the topical application of physiologic amounts of the ceramides sphingosine, phytosphingosine, esterified fatty acids, omega hydroxy fatty acids, normal fatty acids, and alpha-hydroxy fatty acid in human volunteers.[38]
A controlled clinical trial assessed the beneficial effects of a ceramide 3-containing emollient using an experimental skin barrier dysfunction model in healthy volunteers.[39] Skin barrier dysfunction was caused by tape stripping, which resulted in erythema and increased transepidermal water loss associated with up-regulation of cycling cells, involucrin, and expression of cytokeratin-16. Half the injured areas were treated once daily with the test product for five days. On Day 4, the ceramide-containing emollient significantly decreased erythema, transepidermal water loss, and cycling cells vs. the untreated site.
Niacinamide. Niacinamide (or niacin) is a form of vitamin B3 with antioxidant properties that help improve skin appearance. It regulates poly-ADP ribose-polymerase 1, an enzyme with important roles in DNA repair and the expression of inflammatory cytokines.[40] Niacinamide has been shown to increase the beneficial effects of moisturizers for treating xerosis by improving the integrity of the stratum corneum41 and increasing corneal hydration.[42–44]
The application of niacinamide can also improve the appearance of fine lines and wrinkles[45],[46] hyperpigmentation spots, texture, red blotchiness, and sallowness.46 In one randomized clinical trial, female subjects (N=50) with signs of facial photoaging including fine lines and wrinkles, poor texture, and hyperpigmented spots applied 5% niacinamide to half of the face and its vehicle control to the other half twice daily for 12 weeks.[47] Facial images and instrumental measures were obtained at baseline and at four-week intervals. Significant improvements in skin appearance included reduction in fine lines and wrinkles, hyperpigmented spots, red blotchiness, sallowness, and skin elasticity. Interestingly, oral nicotinamide has recently been shown to be effective for reducing nonmelanoma skin cancers and actinic keratoses in high-risk patients.[48]
Phytonadione. Topically applied phytonadione, or vitamin K1, has been shown to have beneficial effects on injured skin. Using an animal model, a topical vitamin K cream increased experimental wound healing.[49] Clinically, topical vitamin K enhanced the healing of bruises caused by laser treatment. In one randomized, double-blind, placebo-controlled study (N=22), subjects applied vitamin K cream to one side of their face for two weeks before and/or two weeks after laser treatment for facial telangiectases using a 585nm pulsed dye laser.[50] There was no difference in the extent of bruising on the topical vitamin K-treated sides; however, the severity of bruising was significantly less on the vitamin K-treated sides. In a similar randomized, controlled study, the application of vitamin K gel following pulsed dye laser treatment shortened the time for resolution of facial bruising.[51]
Recommendations for the Treatment of Actinic Purpura
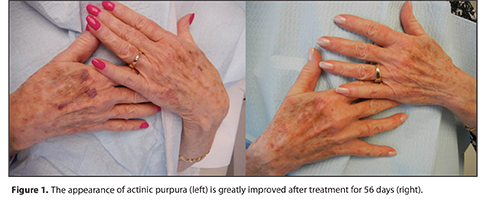
My personal observation is that DerMend is very effective for the treatment of actinic purpura. My patients are exceedingly pleased with the results they have achieved as shown in Figure 1 and Figure 2. I recommend that patients treat their hands and forearms where sun damage is more pronounced and where the skin is thinner and skin injury is more likely to occur. For some patients, this may also include the lower legs. The product should be applied to all areas twice daily to improve skin quality and prevent or minimize future lesions and three times daily on bruised areas to improve healing. Sunscreens that provide both UVA and UVB protection should be applied daily, especially to affected areas.
{kind=link}
{kind=link}
References
1. Yaar M, Gilchrest BA. Skin aging: postulated mechanisms and consequent changes in structure and function. Clin Geriatr Med. 2001;17:617–630.
2. Poljšak B, Dahmane RG, Godi? A. Intrinsic skin aging: the role of oxidative stress. Acta Dermatovenerol Alp Pannonica Adriat. 2012;21:33–36.
3. Panich U, Sittithumcharee G, Rathviboon N, et al. Ultraviolet radiation-induced skin aging: the role of DNA damage and oxidative stress in epidermal stem cell damage-mediated skin aging. Stem Cells Int. 2016;2016:7370642.
4. Al-Nuaimi Y, Sherratt MJ, Griffiths CE. Skin health in older age. Maturitas. 2014;79:256–264.
5. Sahle FF, Gebre-Mariam T, Dobner B, et al. Skin diseases associated with the depletion of stratum corneum lipids and stratum corneum lipid substitution therapy. Skin Pharmacol Physiol. 2015;28:42–55.
6. Kaya G, Saurat JH. Dermatoporosis: a chronic cutaneous insufficiency/fragility syndrome. Clinicopathological features, mechanisms, prevention and potential treatments. Dermatology. 2007;215:284–294.
7. Farage MA, Miller KW, Elsner P, et al. Functional and physiological characteristics of the aging skin. Aging Clin Exp Res. 2008;20:195–200.
8. Beauregard S, Gilchrest BA. A survey of skin problems and skin care regimens in the elderly. Arch Dermatol. 1987;123:1638–1643.
9. Kurban RS, Kurban AK. Common skin disorders of aging: diagnosis and treatment. Geriatrics. 1993;48:30–42.
10. Reszke R, Pe?ka D, Walasek A, et al. Skin disorders in elderly subjects. Int J Dermatol. 2015;54:e332–e338.
11. Kochhar R. Ten projections for the global population in 2050. PEW Research Center, February 3, 2014. http://www.pewresearch.org/fact-tank/2014/02/03/10-projections-for-the-global-population-in-2050/. Accessed October 2016.
12. McKnight B, Seidel R, Moy R. Topical human epidermal growth factor in the treatment of senile purpura and the prevention of dermatoporosis. J Drugs Dermatol. 2015;14:1147–1150.
13. Kalivas L, Kalivas J. Solar purpura. Arch Dermatol. 1988;124:24–25.
14. Menditto V, Borrelli L. Bateman’s disease. Pathologica. 1994;86:645–648.
15. Durai PC, Thappa DM, Kumari R, et al. Aging in elderly: chronological versus photoaging. Indian J Dermatol. 2012;57:343–352.
16. Kaya G, Jacobs F, Prins C, et al. Deep dissecting hematoma: an emerging severe complication of dermatoporosis. Arch Dermatol. 2008;144:1303–1308.
17. Rallis TM, Bakhtian S, Pershing LK, et al. Effects of 0.1% retinoic acid on Bateman’s actinic purpura. Arch Dermatol. 1995;131:493–495.
18. Gupta M, Gupta A. Photodamaged skin and quality of life: reasons for therapy. J Dermatolog Treat. 1996;7:261–264.
19. Kligman AM. Psychological aspects of skin disorders in the elderly. Cutis. 1989;43:498–501.
20. Kong R, Cui Y, Fisher GJ, et al. A comparative study of the effects of retinol and retinoic acid on histological, molecular, and clinical properties of human skin. J Cosmet Dermatol. 2016;15:49–57.
21. Bellemère G, Stamatas GN, Bruère V, et al. Antiaging action of retinol: from molecular to clinical. Skin Pharmacol Physiol. 2009;22:200–209.
22. Randhawa M, Rossetti D, Leyden JJ, et al. One-year topical stabilized retinol treatment improves photodamaged skin in a double-blind, vehicle-controlled trial. J Drugs Dermatol. 2015;14:271–280.
23. Herndon JH Jr, Jiang LI, Kononov T, et al. An open label clinical trial to evaluate the efficacy and tolerance of a retinol and vitamin C facial regimen in women with mild-to-moderate hyperpigmentation and photodamaged facial skin. J Drugs Dermatol. 2016;15:476–482.
24. Lou WW, Quintana AT, Geronemus RG, et al. Effects of topical vitamin K and retinol on laser-induced purpura on nonlesional skin. Dermatol Surg. 1999;25:942–944.
25. Van Scott EJ, Yu RJ. Alpha hydroxy acids: procedures for use in clinical practice. Cutis. 1989;43:222–228.
26. Tung RC, Bergfeld WF, Vidimos AT, et al. alpha-Hydroxy acid-based cosmetic procedures. Guidelines for patient management. Am J Clin Dermatol. 2000;1:81–88.
27. Moy LS, Howe K, Moy RL. Glycolic acid modulation of collagen production in human skin fibroblast cultures in vitro. Dermatol Surg. 1996;22:439–441.
28. Kornhauser A, Coelho SG, Hearing VJ. Applications of hydroxy acids: classification, mechanisms, and photoactivity. Clin Cosmet Investig Dermatol. 2010;3:135–142.
29. Yamamoto Y, Uede K, Yonei N, et al. Effects of alpha-hydroxy acids on the human skin of Japanese subjects: the rationale for chemical peeling. J Dermatol. 2006;33:16–22.
30. Fried RG, Cash TF. Cutaneous and psychosocial benefits of alpha hydroxy acid use. Percept Mot Skills. 1998;86:137–138.
31. Craciunescu O, Constantin D, Gaspar A, et al. Evaluation of antioxidant and cytoprotective activities of Arnica montana L. and Artemisia absinthium L. ethanolic extracts. Chem Cent J. 2012;6:97.
32. Castro FC, Magre A, Cherpinski R, et al. Effects of microcurrent application alone or in combination with topical Hypericum perforatum L. and Arnica montana L. on surgically induced wound healing in Wistar rats. Homeopathy. 2012;101:147–153.
33. Leu S, Havey J, White LE, et al. Accelerated resolution of laser-induced bruising with topical 20% arnica: a rater-blinded randomized controlled trial. Br J Dermatol. 2010;163:557–563.
34. Tfayli A, Guillard E, Manfait M, et al. Raman spectroscopy: feasibility of in vivo survey of stratum corneum lipids, effect of natural aging. Eur J Dermatol. 2012;22:36–41.
35. Meckfessel MH, Brandt S. The structure, function, and importance of ceramides in skin and their use as therapeutic agents in skin-care products. J Am Acad Dermatol. 2014;71:177–184.
36. Danby SG, Brown K, Higgs-Bayliss T, et al. The effect of an emollient containing urea, ceramide NP, and lactate on skin barrier structure and function in older people with dry skin. Skin Pharmacol Physiol 2016;29:135–147.
37. Paragh G, Schling P, Ugocsai P, et al. Novel sphingolipid derivatives promote keratinocyte differentiation. Exp Dermatol. 2008;17:1004–1016.
38. Farwick M, Santonnat B, Lersch P, et al. An aquaporin-inspired lipid concentrate for mature skin. Cosmetics & Toiletries. 2008;123:69–74.
39. Kucharekova M, Schalkwijk J, Van De Kerkhof PC, et al. Effect of a lipid-rich emollient containing ceramide 3 in experimentally induced skin barrier dysfunction. Contact Dermatitis. 2002;46:331–338.
40. Chen AC, Damian DL. Nicotinamide and the skin. Australas J Dermatol. 2014;55:169–175.
41. Christman JC, Fix DK, Lucus SC, et al. Two randomized, controlled, comparative studies of the stratum corneum integrity benefits of two cosmetic niacinamide/glycerin body moisturizers vs. conventional body moisturizers. J Drugs Dermatol. 2012;11:22–29.
42. Chiu PC, Chan CC, Lin HM, et al. The clinical anti-aging effects of topical kinetin and niacinamide in Asians: a randomized, double-blind, placebo-controlled, split-face comparative trial. J Cosmet Dermatol. 2007;6:243–249.
43. Draelos ZD, Ertel K, Berge C. Niacinamide-containing facial moisturizer improves skin barrier and benefits subjects with rosacea. Cutis. 2005;76:135–141.
44. Soma Y, Kashima M, Imaizumi A, et al. Moisturizing effects of topical nicotinamide on atopic dry skin. Int J Dermatol. 2005;44:197–202.
45. Kawada A, Konishi N, Oiso N, et al. Evaluation of anti-wrinkle effects of a novel cosmetic containing niacinamide. J Dermatol. 2008;35:637–642.
46. Bissett DL, Miyamoto K, Sun P, et al. Topical niacinamide reduces yellowing, wrinkling, red blotchiness, and hyperpigmented spots in aging facial skin. Int J Cosmet Sci. 2004;26:231–238.
47. Bissett DL, Oblong JE, Berge CA. Niacinamide: a B vitamin that improves aging facial skin appearance. Dermatol Surg. 2005;31:860–865.
48. Chen AC, Martin AJ, Choy B, et al. A phase 3 randomized trial of nicotinamide for skin-cancer chemoprevention. N Engl J Med. 2015;373:1618–1626.
49. Hemmati AA, Houshmand G, Ghorbanzadeh B, et al. Topical vitamin K1 promotes repair of full thickness wound in rat. Indian J Pharmacol. 2014;46:409–412.
50. Shah NS, Lazarus MC, Bugdodel R, et al. The effects of topical vitamin K on bruising after laser treatment. J Am Acad Dermatol. 2002;47:241–244.
51. Cohen JL, Bhatia AC. The role of topical vitamin K oxide gel in the resolution of post-procedural purpura. J Drugs Dermatol. 2009;8:1020–1024.