 Shivani B. Kaushik, MD; Andrew F. Alexis, MD, MPH Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York
Shivani B. Kaushik, MD; Andrew F. Alexis, MD, MPH Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Background: Nonablative laser resurfacing represents one of the major advances in procedural dermatology over the past decade. However, its use in darker skin types is limited by safety concerns and a relative lack of available data. Aim: To provide evidence-based recommendations for the use of fractional lasers in darker skin types. Evidence review: A broad literature search of PubMed/Medline database was conducted in April 2016 using the term fractional lasers. A free text search of keywords including fractional resurfacing, nonablative lasers, skin type, skin of color, ethnic skin, Fitzpatrick skin type, Asian skin, African Americans, Afro-Caribbean, and Hispanics was also executed. An in-depth review of all the relevant articles fitting the authors’ inclusion/exclusion criteria was performed. Thereafter, each study was assigned levels of evidence per the Modified Criteria by Oxford Center of Evidence Based Medicine. A recommendation was made for a specific treatment based on the presence of at least one Level 1 study or more than three Level 2 or 3 studies that had concordant results. Findings: The available evidence strongly suggests that fractional lasers are a favorable treatment option for a variety of dermatological diseases in Fitzpatrick skin phototypes IV to VI. Level 1 evidence was found for the use of fractional lasers for treating acne, striae and skin rejuvenation. Level 2 evidence was found for their use in acne scars, melasma, and surgical/traumatic scars. Conclusion: Fractional resurfacing is a safe and efficacious treatment option for various dermatological disorders in darker skin types; however, there is a paucity of high-quality studies involving skin types V and VI. J Clin Aesthet Dermatol. 2017;10(6):51–67
Nonablative laser resurfacing represents one of the major advances in procedural dermatology over the past decade and has become the treatment of choice for a broad range of aesthetic indications. However, safety concerns related to their use in darker skin types remain. The vast majority of studies of fractional laser resurfacing in non-white patient populations involve Asian skin types or are limited to Fitzpatrick skin photo types (SPTs) IV. Published data related to the treatment SPTs V and VI are limited. Herein, the authors review studies involving nonablative fractional lasers in the treatment of skin of color (SPT IV–VI) and suggest optimal parameters that can be used safely in these patients.Nonablative laser resurfacing represents one of the major advances in procedural dermatology over the past decade and has become the treatment of choice for a broad range of aesthetic indications. However, safety concerns related to their use in darker skin types remain. The vast majority of studies of fractional laser resurfacing in non-white patient populations involve Asian skin types or are limited to Fitzpatrick skin photo types (SPTs) IV. Published data related to the treatment SPTs V and VI are limited. Herein, the authors review studies involving nonablative fractional lasers in the treatment of skin of color (SPT IV–VI) and suggest optimal parameters that can be used safely in these patients.
Fractional Lasers
The concept of fractional lasers was introduced by Manstein et al in 2004.[1] Since then, it has revolutionized the field of laser resurfacing. Fractional lasers create microscopic heat columns causing areas of thermal damage known as microscopic thermal zones (MTZs). These MTZs range from 100 to 400µm in width and approximately 300 to 700µm in depth.[2]
The MTZs are separated by areas of normal skin, which acts as a reservoir for tissue regeneration and remodeling. These zones comprise up to 15 to 25 percent of the skin surface area per treatment session.[3],[4]
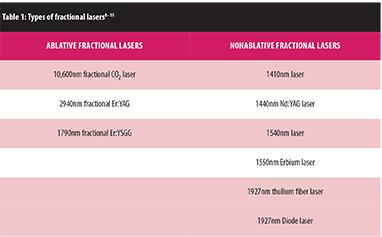
Fractional lasers can be further subdivided into ablative and nonablative depending on their impact on stratum corneum. Ablative fractional lasers have longer wavelengths in the range of 2940 to 10600nm and lead to full thickness destruction of skin. Whereas, nonablative fractional lasers have wavelengths ranging from 1320 to 1927nm and leave a functionally and histologically intact stratum corneum compared to nonablative fractional lasers. Ablative fractional lasers are usually associated with greater efficacy but longer recovery time and higher risk of complications in SPTs IV to VI.[4–7]
Table 1 delineates the types of fractional devices currently used in practice.[8–15]
{kind=link}
Melanin-rich skin types are more susceptible to pigmentary alterations post laser resurfacing due to direct (e.g., melanosome disruption) and indirect (e.g., postinflammatory) effects of treatment. A higher risk of keloid or hypertrophic scarring in patients of African or Asian ancestry is also a safety consideration in laser resurfacing involving dermal injury. Nonablative fractional lasers are mid infra-red lasers that target water instead of melanin and hence these lasers are safe for use in darker skin types.[8],[16]
Methods
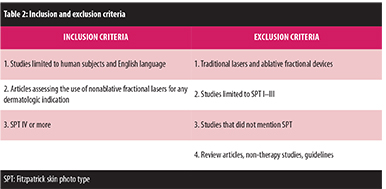
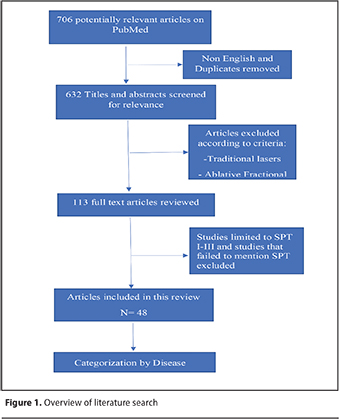
The primary objective of this comprehensive review is to provide evidence-based recommendations for the use of nonablative fractional lasers in SPTs IV–VI. The authors sought to obtain all the published articles that studied nonablative fractional lasers in skin of color patients. A broad literature search of PubMed/Medline database was conducted in April 2016 using the term fractional lasers. An extensive PubMed search was conducted using the following search combinations: fractional lasers and acne vulgaris, fractional lasers and acne scars, fractional lasers and melasma, fractional lasers and skin rejuvenation, fractional lasers and photodamage, fractional lasers and striae, fractional lasers and traumatic/surgical scars. The term fractional lasers was also combined with skin type search: fractional lasers and dark skin, fractional laser and ethnic skin, fractional laser and Fitzpatrick skin photo types, fractional lasers and skin of color and fractional lasers with Asian skin. A free text search of keywords, including fractional resurfacing, nonablative lasers, Fitzpatrick skin type, skin of color, ethnic skin, Asian skin, African Americans, Afro-Caribbean, and Hispanics was also executed. Appropriate filters were used to limit the search to only English language and studies involving human subjects. All the titles and abstracts were screened for relevance to our topic. Thereafter, full texts of all the relevant articles were reviewed to fit their inclusion/exclusion criteria (Table 2).
{kind=link}
The inclusion criteria required articles to assess the use of nonablative fractional lasers for any dermatological indication in skin of color subjects. Where applicable, studies comparing nonablative fractional lasers with other treatment modalities were also included.
Articles limiting themselves to traditional lasers and ablative fractional lasers were excluded. The authors also excluded studies that were limited to SPTs I to III or failed to mention the SPT of their target population. Review articles, commentaries, letters, and posters were also excluded. References of all the included articles were reviewed to ensure completeness. An overview of the literature search is outlined in Figure 1.
{kind=link}
Data Extraction and Analysis
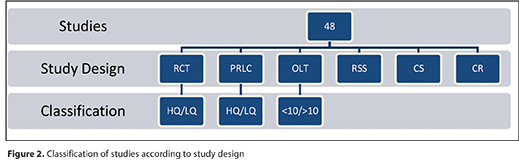
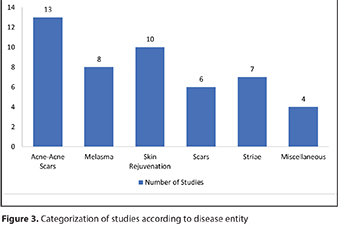
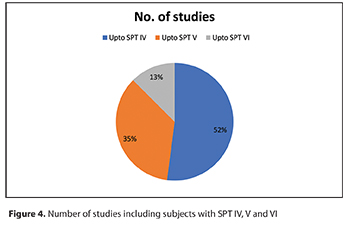
Forty-eight articles that met the authors’ inclusion/exclusion criteria were identified. These were classified according to their study design, dermatologic indication and SPTs included (Figure 2, Figure 3, Figure 4).
{kind=link}
{kind=link}
{kind=link}
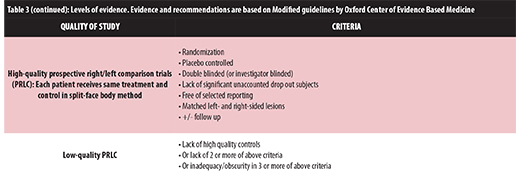
Randomized controlled trials (RCTs) and prospective right/left comparison studies (PRLCs) were further determined to be either high quality or low quality depending on whether they were placebo controlled and double blinded. Open-label trials (OLTs) were classified based on the number of patients involved in the study.
Thereafter, each study was assigned levels of evidence according to the Modified Criteria published by Oxford Center of Evidence Based Medicine (Table 3, Table 3 Continued). A recommendation was made for a disease based on the presence of at least one Level 1 study or more than three Level 2 or 3 studies that had concordant results.
{kind=link}
{kind=link}
Acne and Acne Scars
Acne scars are a result of destruction of collagen secondary to inflammation. It is a potentially disfiguring condition and can be difficult to treat in skin of color patients owing to a higher risk of scarring and pigmentary abnormalities.[40]
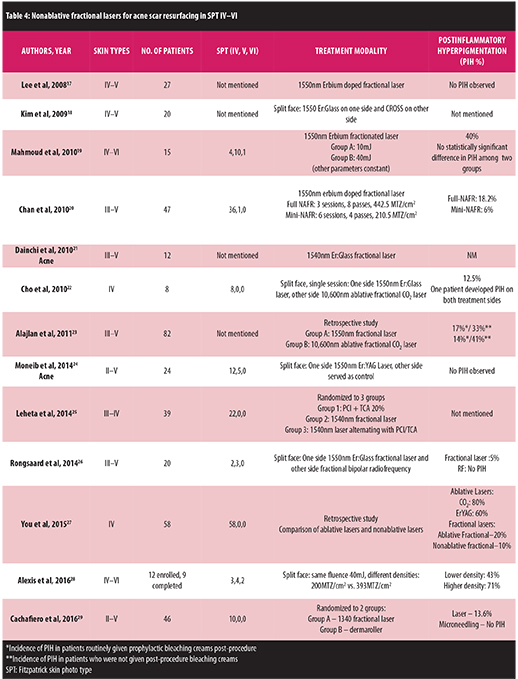
A large number of studies have demonstrated the safety and efficacy of fractional lasers in treating acne scars in lighter skin types. Only a limited number of studies have included skin types IV to VI. Table 4 depicts the relevant details of these studies.[17–29]
{kind=link}
Based on the studies mentioned in Table 4, fractional nonablative lasers are a safe and effective treatment option for acne scars in skin type IV to VI. Kim et al[18] reported that nonablative fractional laser is superior to chemical reconstruction of skin scars (CROSS) in treating rolling type acne scars and recommended that type of scars should be kept in mind when choosing between treatment options. Mahmoud et al19 reported a statistically significant improvement in acne scars from baseline following treatment with nonablative fractional laser but improvement was not statistically significant between the 10mJ and 40mJ groups. No difference in incidence of postinflammatory pigmentation was observed among the two groups but pain was significantly higher in 40mJ group. Patients with skin type V and VI reported higher average pain scores than skin type IV patients. Chan et al[20] compared full nonablative fractional resurfacing (NAFR) (3 sessions/8 passes/ 442.5 MTZ/cm2) with mini-NAFR (6 sessions/4 passes/210.5 MTZ/cm2) in Asian acne scar patients. There was no difference in clinical efficacy between three sessions of full-NAFR and six sessions of mini-NAFR at the end of follow up; however, the incidence of postinflammatory hyperpigmentation (PIH) was statistically lower in the mini-NAFR group as compared to the full-NAFR group. A recent split-face study performed by Alexis et al[28] compared the effect of different treatment densities (220MTZ/cm2 vs 393 MTZs/cm2) on acne scars while keeping the fluence constant at 40mJ. There was no statistically significant difference between different density groups in regards to acne scar improvement and incidence of PIH.
A few studies have demonstrated the efficacy of nonablative fractional laser in treating active acne vulgaris in darker skin types. Moneib et al[24] studied the use of fractional lasers as a treatment of active acne vulgaris in 24 patients (SPT II–V) in a randomized controlled split-face study. Each patient received four treatment sessions at two-week intervals and were followed up every three months for a total duration of one year. This study noted a complete clearance of acne during treatment which was maintained during the yearlong follow-up period. Histological analysis was also performed which showed a significant decrease in size of sebaceous glands along with improvement in skin texture and sebum production. Another split-face study by Dainichi et al[21] studied the effect of fractional lasers in 12 Asian patients and reported a significant improvement in acne and skin tightening effect after two sessions.
In conclusion, nonablative fractional laser is an effective modality to treat acne vulgaris (Level 1b evidence) and acne scars (Level 2b evidence) in skin of color. The risk of developing PIH depends on numerous factors including SPT, laser device, and energy and density settings. However, treatment density is a stronger factor than energy in determining PIH development. More studies and experience are needed to determine the optimum settings to maximize the risk-benefit ratio, especially in skin type V to VI.
Melasma
Melasma is a challenging condition for both patient and doctors alike. Quality-of-life studies have shown significant negative impact of melasma on emotional wellbeing, social life, and leisure activities.[30]
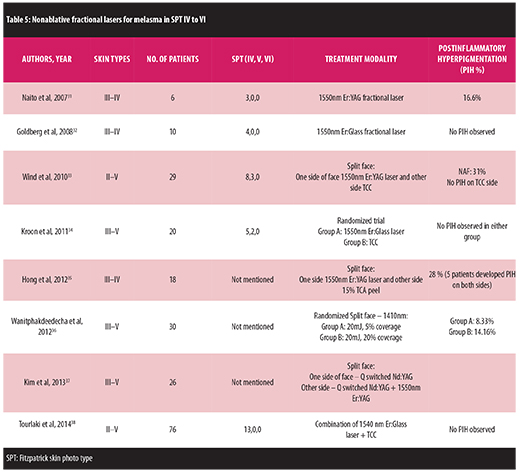
Sun protection, bleaching creams, and chemical peels remain the first-line treatment modalities. Combination therapies are generally needed to tackle melasma owing to its chronic relapsing nature. Limited numbers of studies in the past have assessed the use of fractional laser in skin of color melasma patients (Table 5).[31–38]
{kind=link}
Goldberg et al[32] performed a histological and clinical analysis of the effect of nonablative fractional laser in melasma. They noted a relative decrease in the number of melanocytes in the and clinical improvement post treatment. Wind et al33 performed a split-face study comparing 1550 nonablative laser with triple combination cream (TCC). Worsening of hyperpigmentation was reported in nine (31%) patients on the laser treatment side. Overall patient satisfaction was significantly lower on laser side as compared to TCC side. At the end of the study, most patients preferred TCC over laser. Another study by Kroon et al[34] compared nonablative fractional laser with triple combination cream in a randomized trial. Both fractional laser and TCC were reported to have similar efficacy and recurrence rates at six-month follow up. Hong et al[35] compared nonablative fractional laser with 15% trichloroacetic acid (TCA) peel in a split-face study. They concluded that they are equal in terms of clinical efficacy and neither of them is long lasting. Wanitphakdeedecha et al[36] reported a significantly higher incidence of PIH on the side treated with 20mJ/20% coverage as compared to 20mJ/5% coverage side. Tourlaki et al[38] assessed the efficacy of combination therapy, nonablative fractional laser and TCC in resistant melasma cases. They observed marked (>75%) and moderate improvement (51–75%) in melasma area sensitivity index (MASI) scores in 67 and 21 percent of patients, respectively.
In summary, available evidence supports that nonablative fractional lasers are comparable in efficacy to triple combination creams in the treatment of melasma. The ideal fractional laser settings for melasma treatment largely depends on the skin phototype and the type of melasma being treated. Higher treatment densities and SPT are associated with a greater risk of hyperpigmentation post procedure.[39] Patients with melasma should be counseled about the potential risk of worsening of their pigmentation post resurfacing.[40]
Skin Rejuvenation
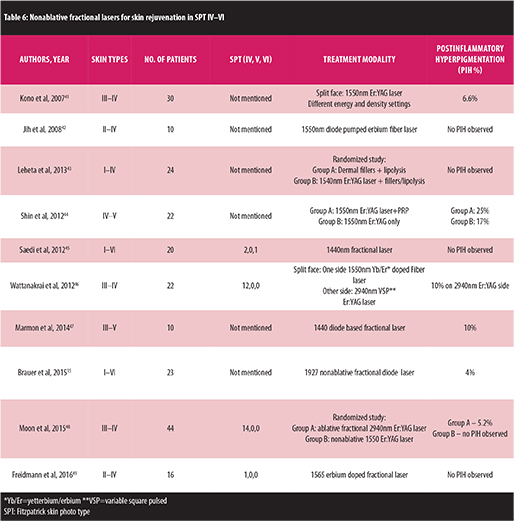
Aging presents with different features in different skin types and ethnicities. Age along with cumulative ultraviolet (UV) damage over the years leads to development of rhytids, skin laxity, textural changes, wrinkles and abnormal pigmentation. Due to the photoprotective effects of melanin, the appearance of wrinkles is usually delayed in ethnic skin and pigmentary changes tend to present earlier.16 Nonablative fractional lasers are widely used for skin rejuvenation but only a few studies have been done to assess their impact in skin type IV to VI (Table 6 ).[41–49]
{kind=link}
Kono et al[41] assessed the efficacy and complications of different energy and density settings of nonablative fractional laser. Pain, edema and erythema were more common in patients treated with higher energy and density settings. Patient satisfaction was reported to be significantly higher in groups treated with higher fluence but not with higher density. Shin et al[44] performed a randomized blinded study where patients were either treated with fractional laser and platelet rich plasma (PRP) or fractional laser alone. The group treated with fractional laser and PRP reported higher patient satisfaction when compared to laser alone. Saedi et al[45] performed a single center non-randomized study and determined that 1440nm fractional laser was safe and efficacious in improving visible facial pores and skin texture. Wattanakrai et al[46] compared non ablative fractional laser with variable square pulsed 2940nm Er:YAG laser in a randomized open label trial. Although no difference was noted in efficacy, less downtime with fractional laser correlated positively with higher patient satisfaction.
In conclusion, there is strong evidence that nonablative fractional laser is a safe and effective modality for skin rejuvenation in skin of color.
Scar resurfacing
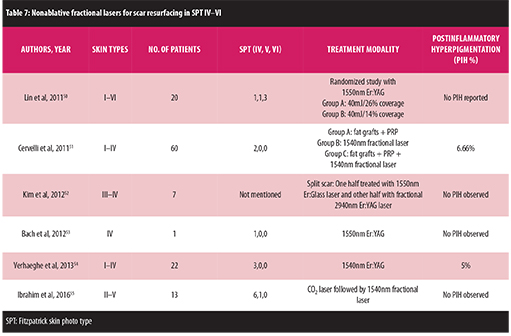
Keloids and hypertrophic scars are more prevalent in racial/ethnic populations with SPT IV–VI. Multiple treatment modalities such as intralesional steroid injections, silicone sheets, cryotherapy, excision and laser surgery are currently used to treat scars or improve their appearance. However, the response to these treatments is often unsatisfactory and unpredictable. The following studies assess the effectiveness of nonablative fractional laser for treating keloids, hypertrophic and surgical scars (Table 7).[50–55]
{kind=link}
A randomized blinded study was performed by Lin et al50 wherein linear surgical hypertrophic scars were divided into halves. One half of the scar was further randomized to receive either high density (40mJ/26% coverage) or low density (40mJ/14% coverage) treatment whereas the other half served as control. No significant difference was observed in the efficacy of high density and low density groups. Moreover, high density group reported high incidence of side effects such as erythema, pain, swelling and scabbing. This study also emphasized the importance of treating scars at an earlier stage as younger scars respond better to treatment. Cervelli et al[51] performed a randomized blinded study analyzing the combined effects of fractional resurfacing, fat grafting and use of PRP in treating traumatic scars. They suggest that combining fractional lasers with platelet rich plasma yields better results as compared to a solitary approach.
In conclusion, there is moderate level evidence that nonablative fractional lasers are a safe and effective treatment option for scars with improvement in both texture and appearance of scars.
Striae distensae
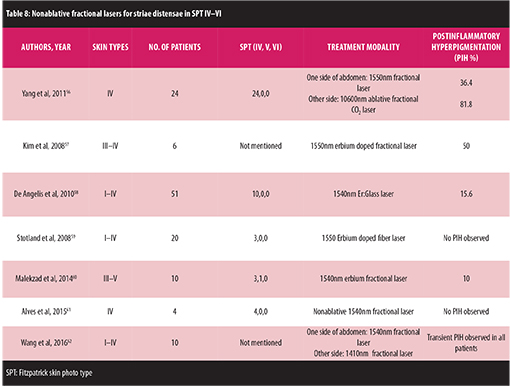
Striae distensae or stretch marks are a result of rapid stretching of the dermis usually due to sudden changes in weight, use of corticosteroids, pregnancy and adolescent growth spurts. Striae develop through three stages: initial inflammatory stage when they are red in color known as Striae rubra, progressing to next stage of purple coloration and last stage of white atrophic striae referred to as striae alba (Table 8).[56–62]
{kind=link}
Striae distensae are a challenging condition to treat. Fractional lasers lead to clinical as well as histopathological improvement in striae by promoting collagen regeneration.[58]
Yang et al[56] conducted a randomized blinded split study comparing nonablative and ablative fractional laser for the treatment of striae distensae on abdomen. No significant difference was seen between the two groups. Kim et al57 performed a prospective right left comparison study with ErYAG laser treatment on one side and other side serving as control. They suggested ErYAG nonablative fractional laser is an safe and effective treatment for striae distensae. Another prospective open label trial by De Angelis et al[58] also confirmed the efficacy of nonablative fractional lasers in reducing striae distensae.
There is moderate evidence (2a) suggesting the efficacy of nonablative lasers for treating striae in skin of color. To the best of the authors’ knowledge, none of the studies so far have included skin types VI and only one study treated skin type V patient. Therefore, more high quality studies are needed to establish the efficacy of nonablative fractional lasers for treating striae in darker skin types.
Complications
Fractional lasers represent a better standard of safety than the traditional lasers but they are not without side effects. Post-treatment side effects, such as transient erythema, edema and hyperpigmentation, have been well documented in almost all the studies. Graber et al9 reported the incidence of complications from1550nm erbium doped laser treatments. They performed 961 consecutive treatments in 422 patients of SPT I to V. The most common complications were acneiform eruptions (1.87%), outbreaks of herpes simplex virus (HSV) (1.77%) and erosions (1.35%). Other less frequent side effects were prolonged erythema (0.83%), PIH (0.73%), prolonged edema (0.62%) and dermatitis (0.21%). Single cases of impetigo and purpura were also reported. Most of the side effects listed above were seen equally in all skin types except PIH, which was reported to be more common in skin of color patients.[2],[9]
Recognition of the potential complications of fractional laser use is important owing to its growing popularity. Table 9 summarizes the commonly encountered side effects according to their degree of severity.[9],[10],[63],[64]
{kind=link}
Recommendation
Levels of evidence and strength of recommendation is summarized in Table 10.
{kind=link}
Careful patient selection and setting realistic expectations prior to starting treatment are the most important preliminary steps to ensure a favorable outcome. The importance of post-procedure skin care cannot be overemphasized. Patients should be counseled and strongly encouraged to use broad spectrum sunscreen during the course of treatment. The use of pre-and post-procedure hydroquinone to prevent PIH has been advocated my several authors, but studies confirming the efficacy of hydroquinone in preventing resurfacing laser-induced PIH are currently lacking.[28]
Patients should be made aware that clinical improvement and side effects largely depend on what laser settings are used which are further determined based on the skin type and indication for treatment. Both energy and density are key parameters that determine the safety and efficacy of fractional resurfacing in skin of color patients although treatment density plays a more important role in determining the risk of PIH; the higher the treatment density (MTZ/cm2), the higher the risk of PIH. Other parameters which can be modified to decrease the incidence of side effects are number of passes per treatment session, increasing treatment intervals and providing additional cooling between passes to reduce bulk heating. It is advisable to increase the duration between two treatment sessions if PIH occurs between two laser treatment sessions.[40]
Conclusion
In conclusion, the available evidence strongly suggests that fractional lasers are a favorable treatment option for a variety of dermatological diseases in skin of color. As the patient population seeking laser procedures becomes more diverse, it is increasingly important to understand racial, ethnic and phototype variations in safety and overall treatment outcomes. Key strategies should include careful patient selection, appropriate device selection, use of conservative treatment settings and sunscreens. Fractional resurfacing has opened the door to laser treatment of numerous dermatologic concerns in darker skin types that were previously contraindicated due to safety concerns. While considerable data exists for using fractional lasers in SPT I to IV, more studies that include SPT V to VI are sorely needed to further elucidate optimal treatment parameters for patients with skin of color.
REFERENCES
1. Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004;34(5):426–438.
2. Fisher GH, Geronemus RG. Short-term side effects of fractional photothermolysis. Dermatol Surg. 2005;31(9 Pt 2):1245–1249; discussion 9.
3. Hsiao FC, Bock GN, Eisen DB. Recent advances in fractional laser resurfacing: new paradigm in optimal parameters and post-treatment wound care. Adv Wound Care. 2012;1(5):207–212.
4. Alexiades-Armenakas MR, Dover JS, Arndt KA. The spectrum of laser skin resurfacing: nonablative, fractional, and ablative laser resurfacing. J Am Acad Dermatol. 2008;58(5):719–737; quiz 738–740.
5. Saedi N, Petelin A, Zachary C. Fractionation: a new era in laser resurfacing. Clin Plast Surg. 2011;38(3):449–461, vii.
6. Tajirian AL, Goldberg DJ. Fractional ablative laser skin resurfacing: a review. J Cosmet Laser Ther. 2011;13(6):262–264.
7. Stewart N, Lim AC, Lowe PM, Goodman G. Lasers and laser-like devices: part one. Australas J Dermatol. 2013;54(3):173–183.
8. Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013;169(Suppl 3):91–97.
9. Graber EM, Tanzi EL, Alster TS. Side effects and complications of fractional laser photothermolysis: experience with 961 treatments. Dermatol Surg. 2008;34(3): 301–305; discussion 305–307.
10. Metelitsa AI, Alster TS. Fractionated laser skin resurfacing treatment complications: a review. Dermatol Surg. 2010;36(3): 299–306.
11. Rossi AM, Perez MI. Laser therapy in Latino skin. Facial Plast Surg Clin North Am. 2011;19(2): 389–403.
12. Preissig J, Hamilton K, Markus R. Current laser resurfacing technologies: a review that delves beneath the surface. Semin Plast Surg. 2012;26(3):109–116.
13. Doherty SD, Doherty CB, Markus JS, Markus RF. A paradigm for facial skin rejuvenation. Facial Plast Surg. 2009;25(4):245–251.
14. Carniol PJ, Woolery-Lloyd H, Zhao AS, Murray K. Laser treatment for ethnic skin. Facial Plast Surg Clin North Am. 2010;18(1):105–110.
15. Brauer JA, Alabdulrazzaq H, Bae YS, Geronemus RG. Evaluation of a low energy, low density, non-ablative fractional 1927 nm wavelength laser for facial skin resurfacing. J Drugs Dermatol. 2015;14(11):1262–1267.
16. Woolery-Lloyd H, Viera MH, Valins W. Laser therapy in black skin. Facial Plast Surg Clin North Am. 2011;19(2):405–416.
17. Lee HS, Lee JH, Ahn GY, et al. Fractional photothermolysis for the treatment of acne scars: a report of 27 Korean patients. J Dermatolog Treat. 2008;19(1):45–49.
18. Kim HJ, Kim TG, Kwon YS, et al. Comparison of a 1,550nm Erbium: glass fractional laser and a chemical reconstruction of skin scars (CROSS) method in the treatment of acne scars: a simultaneous split-face trial. Lasers Surg Med. 2009;41(8):545–549.
19. Mahmoud BH, Srivastava D, Janiga JJ, et al. Safety and efficacy of erbium-doped yttrium aluminum garnet fractionated laser for treatment of acne scars in type IV to VI skin. Dermatol Surg. 2010;36(5):602–609.
20. Chan NP, Ho SG, Yeung CK, et al. The use of non-ablative fractional resurfacing in Asian acne scar patients. Lasers Surg Med. 2010;42(10):710–715.
21. Dainichi T, Kawaguchi A, Ueda S, et al. Skin tightening effect using fractional laser treatment: I. A randomized half-side pilot study on faces of patients with acne. Dermatol Surg. 2010;36(1):66–70.
22. Cho SB, Lee SJ, Cho S, et al. Non-ablative 1550-nm erbium-glass and ablative 10 600-nm carbon dioxide fractional lasers for acne scars: a randomized split-face study with blinded response evaluation. J Eur Acad Dermatol Venereol. 2010;24(8):921–925.
23. Alajlan AM, Alsuwaidan SN. Acne scars in ethnic skin treated with both non-ablative fractional 1,550 nm and ablative fractional CO2 lasers: comparative retrospective analysis with recommended guidelines. Lasers Surg Med. 2011;43(8):787–791.
24. Moneib H, Tawfik AA, Youssef SS, Fawzy MM. Randomized split-face controlled study to evaluate 1550-nm fractionated erbium glass laser for treatment of acne vulgaris–an image analysis evaluation. Dermatol Surg. 2014;40(11):1191–1200.
25. Leheta TM, Abdel Hay RM, Hegazy RA, El Garem YF. Do combined alternating sessions of 1540 nm nonablative fractional laser and percutaneous collagen induction with trichloroacetic acid 20% show better results than each individual modality in the treatment of atrophic acne scars? A randomized controlled trial. J Dermatolog Treat. 2014;25(2):137–141.
26. Rongsaard N, Rummaneethorn P. Comparison of a fractional bipolar radiofrequency device and a fractional erbium-doped glass 1,550-nm device for the treatment of atrophic acne scars: a randomized split-face clinical study. Dermatol Surg. 2014;40(1):14–21.
27. You HJ, Kim DW, Yoon ES, Park SH. Comparison of four different lasers for acne scars: Resurfacing and fractional lasers. J Plast Reconstr Aesthet Surg. 2016;69(4):e87–95.
28. Alexis AF, Coley MK, Nijhawan RI, et al. Nonablative fractional laser resurfacing for acne scarring in patients with Fitzpatrick skin phototypes IV–VI. Dermatol Surg. 2016;42(3):392–402.
29. Cachafeiro T, Escobar G, Maldonado G, et al. Comparison of nonablative fractional erbium laser 1,340 nm and microneedling for the treatment of atrophic acne scars: a randomized clinical trial. Dermatol Surg. 2016;42(2):232–241.
30. Lieu TJ, Pandya AG. Melasma quality of life measures. Dermatol Clin. 2012;30(2):269–280, viii.
31. Naito SK. Fractional photothermolysis treatment for resistant melasma in Chinese females. J Cosmet Laser Ther. 2007;9(3):161–163.
32. Goldberg DJ, Berlin AL, Phelps R. Histologic and ultrastructural analysis of melasma after fractional resurfacing. Lasers Surg Med. 2008;40(2):134–138.
33. Wind BS, Kroon MW, Meesters AA, et al. Non-ablative 1,550 nm fractional laser therapy versus triple topical therapy for the treatment of melasma: a randomized controlled split-face study. Lasers Surg Med. 2010;42(7):607–612.
34. Kroon MW, Wind BS, Beek JF, et al. Nonablative 1550-nm fractional laser therapy versus triple topical therapy for the treatment of melasma: a randomized controlled pilot study. J Am Acad Dermatol. 2011;64(3):516–523.
35. Hong SP, Han SS, Choi SJ, et al. Split-face comparative study of 1550 nm fractional photothermolysis and trichloroacetic acid 15% chemical peeling for facial melasma in Asian skin. J Cosmet Laser Ther. 2012;14(2):81–86.
36. Wanitphakdeedecha R, Keoprasom N, Eimpunth S, Manuskiatti W. The efficacy in melasma treatment using a 1410 nm fractional photothermolysis laser. J Eur Acad Dermatol Venereol. 2014;28(3):293–297.
37. Kim HS, Kim EK, Jung KE, et al. A split-face comparison of low-fluence Q-switched Nd: YAG laser plus 1550 nm fractional photothermolysis vs. Q-switched Nd: YAG monotherapy for facial melasma in Asian skin. J Cosmet Laser Ther. 2013;15(3):143–149.
38. Tourlaki A, Galimberti MG, Pellacani G, Bencini PL. Combination of fractional erbium-glass laser and topical therapy in melasma resistant to triple-combination cream. J Dermatolog Treat. 2014;25(3):218–222.
39. Sherling M, Friedman PM, Adrian R, et al. Consensus recommendations on the use of an erbium-doped 1,550-nm fractionated laser and its applications in dermatologic laser surgery. Dermatol Surg. 2010;36(4):461–469.
40. Alexis AF. Laser resurfacing for treatment of acne scarring in Fitzpatrick skin types V to VI: practical approaches to maximizing safety. Cutis. 2013;92(6):272–273.
41. Kono T, Chan HH, Groff WF, et al. Prospective direct comparison study of fractional resurfacing using different fluences and densities for skin rejuvenation in Asians. Lasers Surg Med. 2007;39(4):311–314.
42. Jih MH, Goldberg LH, Kimyai-Asadi A. Fractional photothermolysis for photoaging of hands. Dermatol Surg. 2008;34(1):73–78.
43. Leheta T, El Garem Y, Hegazy R, et al. Non-ablative 1540 fractional laser: how far could it help injection lipolysis and dermal fillers in lower-face rejuvenation? A randomized controlled trial. J Cosmet Laser Ther. 2013;15(1):13–20.
44. Shin MK, Lee JH, Lee SJ, Kim NI. Platelet-rich plasma combined with fractional laser therapy for skin rejuvenation. Dermatol Surg. 2012;38(4):623–630.
45. Saedi N, Petrell K, Arndt K, Dover J. Evaluating facial pores and skin texture after low-energy nonablative fractional 1440-nm laser treatments. J Am Acad Dermatol. 2013;68(1):113–118.
46. Wattanakrai P, Pootongkam S, Rojhirunsakool S. Periorbital rejuvenation with fractional 1,550-nm ytterbium/erbium fiber laser and variable square pulse 2,940-nm erbium:YAG laser in Asians: a comparison study. Dermatol Surg. 2012;38(4):610–622.
47. Marmon S, Shek SY, Yeung CK, et al. Evaluating the safety and efficacy of the 1,440-nm laser in the treatment of photodamage in Asian skin. Lasers Surg Med. 2014;46(5):375–379.
48. Moon HR, Yun WJ, Lee YJ, et al. A prospective, randomized, double-blind comparison of an ablative fractional 2940-nm erbium-doped yttrium aluminum garnet laser with a nonablative fractional 1550-nm erbium-doped glass laser for the treatment of photoaged Asian skin. J Dermatolog Treat. 2015;26(6):551–557.
49. Friedmann DP, Tzu JE, Kauvar AN, Goldman MP. Treatment of facial photodamage and rhytides using a novel 1,565 nm non-ablative fractional erbium-doped fiber laser. Lasers Surg Med. 2016;48(2):174–180.
50. Lin JY, Warger WC, Izikson L, et al. A prospective, randomized controlled trial on the efficacy of fractional photothermolysis on scar remodeling. Lasers Surg Med. 2011;43(4):265–272.
51. Cervelli V, Nicoli F, Spallone D, et al. Treatment of traumatic scars using fat grafts mixed with platelet-rich plasma, and resurfacing of skin with the 1540 nm nonablative laser. Clin Exp Dermatol. 2012;37(1):55–61.
52. Kim HS, Lee JH, Park YM, Lee JY. Comparison of the effectiveness of nonablative fractional laser versus ablative fractional laser in thyroidectomy scar prevention: a pilot study. J Cosmet Laser Ther. 2012;14(2):89–93.
53. Bach DQ, Garcia MS, Eisen DB. Hyperpigmented burn scar improved with a fractionated 1550 nm non-ablative laser. Dermatol Online J. 2012;18(7):12.
54. Verhaeghe E, Ongenae K, Bostoen J, Lambert J. Nonablative fractional laser resurfacing for the treatment of hypertrophic scars: a randomized controlled trial. Dermatol Surg. 2013;39(3 Pt 1):426–434.
55. Ibrahim SM, Elsaie ML, Kamel MI, Mohammed EE. Successful treatment of traumatic scars with combined nonablative fractional laser and pinpoint technique of standard CO2 laser. Dermatol Ther. 2016;29(1):52–57.
56. Yang YJ, Lee GY. Treatment of striae distensae with nonablative fractional laser versus ablative CO2 fractional laser: a randomized controlled trial. Ann Dermatol. 2011;23(4):481–489.
57. Kim BJ, Lee DH, Kim MN, et al. Fractional photothermolysis for the treatment of striae distensae in Asian skin. Am J Clin Dermatol. 2008;9(1):33–37.
58. de Angelis F, Kolesnikova L, Renato F, Liguori G. Fractional nonablative 1540-nm laser treatment of striae distensae in Fitzpatrick skin types II to IV: clinical and histological results. Aesthet Surg J. 2011;31(4):411–419.
59. Stotland M, Chapas AM, Brightman L, et al. The safety and efficacy of fractional photothermolysis for the correction of striae distensae. J Drugs Dermatol. 2008;7(9):857–861.
60. Malekzad F, Shakoei S, Ayatollahi A, Hejazi S. The safety and efficacy of the 1540nm non-ablative fractional XD probe of Star Lux 500 Device in the treatment of striae alba: before-after study. J Lasers Med Sci. 2014;5(4):194–198.
61. Alves RO, Boin MF, Crocco EI. Striae after topical corticosteroid: treatment with nonablative fractional laser 1540nm. J Cosmet Laser Ther. 2015;17(3):143–147.
62. Wang K, Ross N, Osley K, et al. Evaluation of a 1540-nm and a 1410-nm nonablative fractionated laser for the treatment of striae. Dermatol Surg. 2016;42(2):225–231
.63. Marra DE, Yip D, Fincher EF, Moy RL. Systemic toxicity from topically applied lidocaine in conjunction with fractional photothermolysis. Arch Dermatol. 2006;142(8):1024–1026.
64. Mamelak AJ, Goldberg LH, Marquez D, et al. Eruptive keratoacanthomas on the legs after fractional photothermolysis: report of two cases. Dermatol Surg. 2009;35(3):513–518.