 Dear Editor:
Dear Editor:
 Dear Editor:
Dear Editor:Tooth discoloration associated with dental hygiene products is commonplace in the field of dentistry; in dermatology, tetracycline is a known cause of tooth discoloration in children.1 We present a case of a 40-year-old Caucasian woman who developed sudden-onset tooth discoloration during her rosacea treatment, which included oral doxycycline. Intrinsic and extrinsic causes of tooth discoloration are briefly reviewed. As physicians, we should consider oral hygiene status in our global antiaging aesthetics plan.
Case presentation. A 40-year-old Caucasian woman presented to our dermatology clinic with rosacea. She was prescribed oral doxycycline 50mg once daily and metronidazole lotion at bedtime. Seven weeks after starting this regimen without complaint, she contacted the office stating her teeth had become discolored “overnight.”
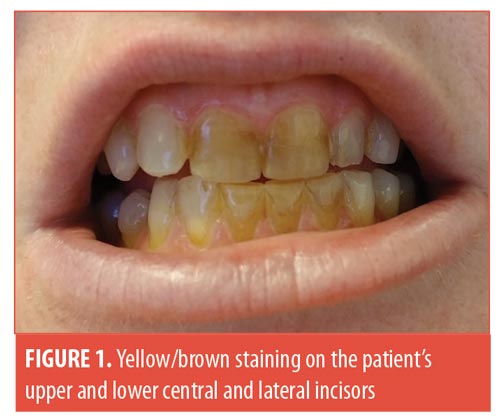
On examination, yellow/brown staining was noted on her upper and lower central and lateral incisors (Figure 1) The patient denied use of tobacco or methamphetamines. Because of her familial history of poor dentition, she self-prescribed Listerine Smart Rinse® (Johnson & Johnson, New Brunswick, New Jersey). Upon further questioning, she revealed changing her mouthwash to Listerine Sensitivity Alcohol-Free Mouthwash® (Johnson & Johnson, New Brunswick, New Jersey) several days prior to the onset of tooth discoloration. We advised her to discontinue her mouthwash and undergo a professional dental cleaning.
Two days after discontinuing the Listerine Sensitivity Alcohol-Free Mouthwash® while still on her rosacea regimen, she observed that the discoloration was less noticeable. The remaining discoloration was removed with a professional dental cleaning. Her dentist confirmed that the mouthwash was most likely the cause of the tooth discoloration.
Discussion. Drug-associated tooth discoloration is well documented in the medical literature.1 Staining of teeth is classified as either intrinsic or extrinsic (Table 1).2 Intrinsic staining is the result of structural changes to dental hard tissues during tooth development and is associated with certain metabolic diseases or systemic medications.3 Tetracyclines (TCNs) can cause intrinsic staining when ingested by children eight years of age or younger due to pediatric odontogenesis.1 TCN-associated tooth discoloration is dose dependent, varies in color between gray, brown, blue, and yellow, and darkens with sun exposure due to photo-oxidation. Intrinsic staining caused by TCNs is permanent. Interventions include veneers, composite resins, or full-coverage crowns.4 Although the literature supports a causative relationship between TCN and intrinsic tooth discoloration in children eight years of age or younger, no such relationship is known to exist with doxycycline.5,6 This is thought to be due to the lower binding affinity of doxycycline with calcium compared to TCNs.6

Extrinsic staining is discoloration that presents on the surface of the tooth that can be corrected with a professional dental cleaning.1 Dental hygiene products have been previously associated with extrinsic tooth staining.1 Cetylpyridium chloride, found in Listerine Smart Rinse®, is an antiseptic that can cause yellow-brown staining through precipitation caused by interactions with negatively charged chromogens in food and beverages.1 Other dental hygiene ingredients capable of leading to tooth discoloration include copper salts, stannous fluoride, and chlorhexidine.1
Conclusion. Tooth discoloration associated with dental hygiene products is well documented in the literature.1 We present a case of a 40-year-old old patient with rosacea who experienced a sudden onset of extrinsic tooth staining caused by her oral hygiene regimen. This case allows for the review of agents resulting in dental staining and differentiation between extrinsic and intrinsic staining. As physicians, we should include oral hygiene status in our global antiaging aesthetic plan. This provides an opportunity to question patients about their oral hygiene regimen and develop cooperative relationships with our dental colleagues.
With regard,
Brooke A. Jackson, MD, FAAD, and Cierra D. Taylor, BA
Affiliations. Dr. Jackson and Ms. Taylor are with Skin Wellness Dermatology Associates in Durham, North Carolina.
Disclosures. The author has no conflicts of interest relevant to the content of this article.
Correspondence. Brooke A. Jackson, MD, FAAD; Email: bajacksonmd@gmail.com
References
- Thomas MS, Denny C. Medication-related tooth discoloration: a review. Dent Update. 2014;41(5): 440–447.
- Kadam A, Ganachari M, Mahendra Kumar B, Gurunath S. Drug induced tooth discolouration. Internet J Dent Sci. 2008:7.
- Watts A, Addy M. Tooth discolouration and staining: a review of the literature. Br Dent J. 2001;190(6): 309–316.
- Sánchez AR, Rogers RS 3rd, Sheridan PJ. Tetracycline and other tetracycline-derivative staining of the teeth and oral cavity. Int J Dermatol. 2004;43(10):709–715.
- Pöyhönen H, Nurmi M, Peltola V, et al. Dental staining after doxycycline use in children. J Antimicrob Chemother. 2017;72(10):2887–2890.
- Volovitz B, Shkap R, Amir J, et al. Absence of tooth staining with doxycycline treatment in young children. Clin Pediatr (Phila). 2007;46(2):121–126.