by Leon H. Kircik, MD
Dr. Kircik is from Indiana University School of Medicine, Indianapolis, Indiana; Mount Sinai Medical Center, New York, New York; DermResearch, PLLC, Louisville, Kentucky
Disclosure: Dr. Kircik is a consultant, speaker, investigator, and advisory board member for Galderma.
Abstract
Biologically active agents generally are thought of either as acting synergistically (they work together) or antagonistically (they counteract each other). However, the notion of synergy has a more nuanced meaning in pharmacological discussions. Two agents may complement each other, usually by providing a cumulative or additive effect. Within pharmacological discourse, “synergy” indicates that the sum of two agents’ combined action is greater than the sum of the efficacy of the constituent parts. An example of synergy in dermatological therapy is a novel fixed combination formulation of adapalene 0.1% and benzoyl peroxide 2.5%. While the use of both topical benzoyl peroxide and a retinoid for the management of mild-to-moderate acne vulgaris has become the standard of care, data show that the two agents in the once-daily, fixed combination adapalene/benzoyl peroxide gel formulation confer a synergistic effect, suggesting that the formulation can enhance efficacy and improve patient convenience and adherence.
(J Clin Aesthet Dermatol. 2011;4(11):30–33.)
Multi-agent therapy is common across all medical specialties and diagnoses, based on the well-accepted premise that drugs used in combination can provide complementary effects. Within the field of dermatology, a majority of patients will be prescribed two or more agents to treat their specific condition. Conversely, all prescribers recognize that certain drug combinations can have detrimental effects. As such, biologically active agents are thought of either as acting synergistically or antagonistically or, simply, that they either work together or they work against each other.[1] However, the notion of “synergy” has been expanded within the literature and has a more nuanced, clearly defined meaning in pharmacological discussions. Synergistic combinations would be expected to provide improved therapeutic outcomes, better experiences for patients, and perhaps even improved adherence, as patients may see more rapid and significant benefits of treatment.
Defining Synergy
Even when two agents complement each other, such as by providing distinct mechanisms of action, their combined efficacy typically is equivalent to the sum of the efficacy of the constituents. Put another way, the two agents provide only cumulative efficacy. Certainly, combination therapy provides benefits over either monotherapy; however, there is no apparent increase in efficacy of the constituents by virtue of their combined use.
Rarely, greater than cumulative effect is seen when two or more agents are combined, which is true pharmacological synergy. Within pharmacological discourse, synergy indicates not only that agents are compatible, but that the product of their combined action is greater than the sum of the efficacy of the constituent parts. In basic terms, a simple summing up and comparison of similarly derived variables can be used to identify synergy.[1] Looking at comparable data, if agent A is shown to reduce transepidermal water loss (TEWL) by 12 percent, agent B reduces it by 15 percent, and the combination of agents A+B reduces TEWL by 27 percent, then their effect is cumulative. If the combination of A+B reduced TEWL by 32 percent, then the combination is said to be synergistic.
While this basic description of synergy is generally true, synergy technically is a function of the dose-response curves of the individual agents and their combination. There are several different approaches to describe synergy. One approach can be algebraic. Let us begin with the equation for zero interaction, where da and db are the doses of A and B, respectively, within the combination, which will be termed da,b. Da and Db are the doses of A and B, separately, that are isoeffective in combination. Algebraic function f(da,b) is the effect of combination. The equation for zero interaction line for two agents is: da/Da + db/Db=1.1 If, instead, the combination is synergistic, then the equation will be: da/Da+db/Db<1.
This demonstrates that, in order to achieve a level of efficacy, then the dose of A and/or B in the combination (da and/or db) are lower than the dose anticipated based on their dose-response curves. Thus A and/or B are more effective when used in combination.
Antagonism results in the formula: da/Da+db/Db>1. Here, the required dose of A and/or B (da and/or db) is higher than predicted based on dose-response graphs, indicating a loss of efficacy when the drugs are combined.[1]
Although the equations presented demonstrate the proof of synergy based on dose-response data, other endpoint or evaluation comparisons can be made. For example, synergy could be shown through an analysis of data from a multi-arm study that involves a combination therapy and its constituents. Such comparison would be appropriate because the data were derived from the same study design and under the same investigational scrutiny.[2] Unfortunately, there is no uniform technique to measure synergy in pharmacology. Therefore, different calculation methods will end up in different results so that according to one method a combination may be synergistic, but by another method, it may be antagonistic.[1]
An example of synergy in dermatological therapy is seen with adapalene 1.0% plus benzoyl peroxide (BPO) 2.5% gel formulation (EpiDuo, Galderma, Ft. Worth, Texas), a combination acne therapy in which synergy has been reported. Analysis of the data for the adapalene 1.0%/BPO 2.5% combination gel suggests that the combination formulation works synergistically to reduce lesion counts and improve acne.[2]
Rationale for Combination Therapy
BPO, one of the first treatments marketed for acne vulgaris, remains an important component of the treatment regimen for mild-to-moderate acne.[3] The agent has received renewed interest because its use in combination with oral antibiotics is shown to reduce dependence on systemic agents and reduce the risk of development of Propionibacterium acnes resistance.[4,5] BPO has bactericidal activity against P. acnes.[3,4] It is also shown to confer some degree of comedolytic and anti-inflammatory effects.[6] One investigation confirmed that the keratolytic effects of BPO were similar to those of salicylic acid and tretinoin six hours after application to the skin of healthy volunteers.[7] In fact, at three hours, BPO actually demonstrated more disruption of stratum corneum adhesion than did salicylic acid or tretinoin. BPO was also found to affect deeper levels of the stratum corneum than did salicylic acid, suggesting a role for addressing deeper inflammatory lesions. Despite these findings, BPO is commonly prescribed by dermatologists[8] in combination with other topical therapies to address additional multifactorial aspects of the pathogenesis of acne.
Topical retinoids are anticomedolytic agents shown to regulate keratinization and provide strong efficacy in the management of both inflammatory and noninflammatory acne lesions.[9] Because they target the microcomedone, retinoids are shown to significantly reduce the formation of new acne lesions and can significantly interrupt disease progression.[9] Tretinoin, the first marketed retinoid, has been joined by a new generation of retinoids, such as adapalene and tazarotene.[10] Developed in response to concerns about the instability of tretinoin, the naphthoic acid derivative adapalene was found in vitro to be photostable and not degraded in the presence of BPO.[10]
Given its stability, adapalene has been used widely in combination with topical antimicrobials, including BPO. The agent has been shown to maintain its good tolerability when used in combination with other topical agents and to produce greater efficacy when used in combination with topical BPO, topical clindamycin, or oral antibiotics than any of these agents alone.[11]
Evidence for Synergy of Adapalene/BPO Gel
The fixed combination formulation of adapalene 0.1% and BPO 2.5% is relatively new to the market. The efficacy, safety, and tolerability of the fixed combination formulation has been established in multiple controlled trials. One of the smaller trials of adapalene/BPO gel involved 517 United States subjects randomized 2:2:2:1 to treatment with either adapalene/BPO gel, adapalene alone, BPO alone, or vehicle once daily for 12 weeks. Evaluation included success rate (“clear” or “almost clear” on the Investigator’s Global Assessment or IGA) and lesions counts. At the conclusion of the trial, the success rate for fixed combination therapy was 27.5 percent compared to 15.5 percent for adapelene alone, 15.4 percent for BPO alone, and 9.9 percent for vehicle.[12]
In a North American trial involving 1,429 evaluable subjects, adapalene/BPO gel showed a significantly higher success rate (P? 0.006) and a greater percentage reduction in all acne lesion counts (P? 0.017) compared to adapalene monotherapy, BPO monotherapy, or vehicle gel.[13] Subjects were randomized in 1:1:1:1 fashion to apply either agent once daily for 12 weeks. At conclusion of the trial, the success rate for adapalene/BPO gel was 30.1 percent compared to 19.8 percent with adapalene alone, 22.2 percent for BPO alone, and 11.3 percent for vehicle. By Week 1, adapalene/BPO gel showed a significant early effect for reduction of all lesions types compared with adapalene alone and vehicle. The reduction in inflammatory, noninflammatory, and total lesions was statistically significantly greater for adapalene/BPO than for either monotherapy or vehicle at study conclusion.
An international trial involving 1,670 subjects had a similar design, with patients randomized 1:1:1:1 to treatment with adapalene/BPO, adapalene alone, BPO alone, or vehicle.[14] Again, adapalene/BPO was rated as more successful with a significantly greater reduction in all lesions counts compared to any other therapy at the conclusion of the trial. A significant early treatment effect, as indicated by IGA scores, was identified at Week 2 for combination therapy versus any monotherapy and remained throughout the trial period. The tolerability profile for the fixed combination gel was similar to that for adapalene alone.
A subgroup analysis of 2,453 international subjects aged 12 to 17 confirmed previous favorable findings for adapalene/BPO.[14] The trial design mirrored that of the North American and international studies described above. By Week 8, success scores (IGA) favored adapalene/BPO over either monotherapy or vehicle and the trend continued through the 12 weeks of the study. Of note, by Week 12, the benefit or combination therapy relative to vehicle was 18.7 percent, which was greater than the sum of the benefit obtained with the individual components (adapalene: 5.7%, BPO: 9.2%). The reduction of inflammatory, noninflammatory, and total lesions was significantly greater for combination therapy at Week 12 compared to any other arm.
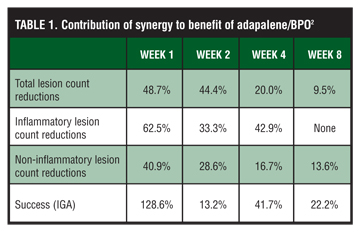
Pooled analysis from three double-blind, controlled trials of similar design including 3,855 subjects shows that adapalene/BPO gel was significantly more efficacious than its monotherapies in decreasing total lesion counts as early as Week 1 and throughout the study period (p<0.05) (Table 1). For up to eight weeks, the combination formulation produced a significantly greater synergistic reduction in median percent total lesion counts (Table 1).[2] For example, at Week 1, reduction in total lesion counts relative to vehicle for adapalene/BPO was 7.4 percent, compared to 1.4 percent for adapalene alone and 2.4 percent for BPO alone. At Week 1, synergy of adapalene/ BPO contributed 48.7 percent of the efficacy in reducing total lesion counts. When the net benefit of combination therapy is quantified, it is greater than the sum of the net benefits for each component. The contribution of synergy to total lesion count reductions was 44.4, 20, and 9.5 percent, respectively, at Weeks 2, 4, and 8.
{kind=link}
Synergy was also observed for reduction in inflammatory lesions through Week 4 and for noninflammatory lesions through Week 8. For reduction in inflammatory lesions, synergy contributed 62.5 percent to efficacy at Week 1, 33.3 percent at Week 2, and 42.9 percent at Week 4.2
IGA ratings showed that adapalene/BPO conferred synergistic success at Weeks 1, 4, 8, and 12. Contribution of synergy to IGA was 128.6, 13.2, 41.7, and 22.2 percent, respectively, at Weeks 1, 2, 4, and 8.2
Contribution of synergy to the efficacy of the combination of adapalene/BPO is most significant early on. For example, contribution of synergy is 48.7 percent in median percent total lesion reduction at Week 1 versus 9.5 percent at Week 8. Similarly, contribution of synergy to success rate at Week one is 128.6 percent versus 22.2 percent at Week 8. There is also no contribution of synergy to any parameters at Week 12 (end of study). It is apparent that early onset of action for efficacy of the fixed combination effect is attributable to synergy.
Limitations of and Basis for Synergy
The data above indicate that the efficacy of fixed combination adapalene/BPO gel provides greater efficacy than the sum of the efficacy scores for its constituents.[2,14] These studies are limited in that the comparison arms each used monotherapy rather than applying separate formulations of BPO and adapalene in combination. However, it does not appear based on these data that synergistic effects would be seen if patients applied separate formulations of BPO and adapalene in combination. Such use could lead to variability in the ratio of drugs applied with each application. Furthermore, the two-step regimen may contribute to decreased adherence.
While it is difficult to ascertain definitively why adapalene/BPO combination gel confers better efficacy than its constituent parts, several possible contributing factors have been identified. A synergistic anti-inflammatory effect of the combination may be attributed to the anti-P. acnes effects of BPO as well as the down-regulation of toll-like receptor 2 by adapalene.[2,14] In addition to its effects on toll-like receptor 2, adapalene is also shown to alter the expression of CD1d (cluster of differentiation) and IL-10 (interleukin), which indicates that it augments the body’s innate immunity.[2]
Furthermore, it is suggested that the effects of adapalene, which alters the follicular microclimate, potentially enhances penetration of BPO.[2,14] Conversely, since BPO is also keratolytic, it may enhance penetration of adapalene.[2]
The comedolytic effects of BPO continue to intrigue researchers and clinicians. Although BPO has long been considered mildly comedolytic, in recent studies of BPO monotherapy, 12-week reductions in noninflammatory lesions of around 40 percent have been reported. Some speculate that the apparently increased comedolytic action of BPO may be due to features of novel formulations that enhance the bioavailability of BPO and its follicular penetration.[2]
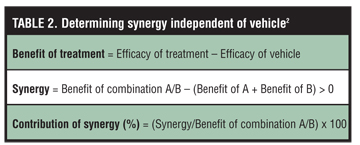
There is some evidence to suggest that characteristics of the vehicle contribute to enhanced efficacy of adapalene 0.1%/BPO 2.5% gel. Of note, in Tan et al’s analysis, they showed that vehicle treatment provided a median 33-percent reduction in total lesions and a median 38-percent reduction in inflammatory lesions at 12 weeks. Therefore, their data analysis on synergy controlled for vehicle effect (Table 2).[2] As such, synergy is adjusted as the net benefit of the combination as well as its components after deducting the vehicle effect from each treatment arm.
{kind=link}
The vehicle, which is shown not to be sensitive to variations in pH, contains a proprietary gelling agent (Simulgel 600 PHA) that does not interfere with the pharmacokinetic properties of adapalene. This copolymer facilitates a homogenous dispersion of adapalene and BPO in the water-based gel. The vehicle also contains humectants, such as glycerol and propylene glycol. Additional stabilizing excipients include disodium edetate, docusate sodium, and poloxamer.
It is suspected but not proven that the formulation’s stability, that is its nonsusceptibility to fluctuations in pH, may further protect the active constituents from degradation and preserve their efficacy even though adapalene is the only retinoid shown to be stable when combined with BPO.
Summary
Many drugs have complementary actions, but very few work synergistically.1 True pharmacological synergy exists when the benefits of combination therapy exceed the sum of the anticipated benefits of the constituent parts. In dermatology, the fixed combination gel formulation of adapalene 0.1% and BPO 2.5% is a combination acne therapy to have synergy.
Given current guidelines[3] and prescribing trends,[15] the use of topical BPO—with or without clindamycin—in combination with a topical retinoid represents the standard of care for patients with mild-to-moderate acne vulgaris. Topical combination regimens are also appropriate and widely used in conjunction with oral acne therapy, which should always be administered with adjunctive topical BPO to prevent bacterial resistance. Studies confirm that adapalene/BPO gel provides therapeutic benefits when used with oral antibiotics.[16]
The optimized formulation of adapalene 0.1% and BPO 2.5% represents a worthwhile option in the topical management of acne, providing synergistic benefits early on for the reduction of inflammatory, noninflammatory, and total acne lesions. By combining two agents into one once-daily formulation, the novel fixed combination gel reduces the number of product applications. The simplicity and convenience of therapy is expected to improve patient adherence. The rapid onset of efficacy made possible by the synergistic effects of the combination gel formulation may further promote adherence.
References
1. Berenbaum MC. What is synergy? Pharmacol Rev. 1989;41(2): 93–41.
2. Tan J, Gollnick HP, Loesche C, Ma YM, Gold LS. Synergistic efficacy of adapalene 0.1%-benzoyl peroxide 2.5% in the treatment of 3,855 acne vulgaris patients. J Dermatolog Treat. 2011;22(4):197–205. Epub 2010 Jul 28.
3. Thiboutot D, Gollnick H, Bettoli V, et al; Global Alliance to Improve Outcomes in Acne. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009;60(5 Suppl):S1–S50.
4. Tanghetti E. The evolution of benzoyl peroxide therapy. Cutis. 2008;82(5 Suppl):5–11.
5. Del Rosso JQ, Kim G. Optimizing use of oral antibiotics in acne vulgaris. Dermatol Clin. 2009;27(1):33–42.
6. Dutil M. Benzoyl peroxide: enhancing antibiotic efficacy in acne management. Skin Therapy Lett. 2010;15(10):5–7.
7. Waller JM, Dreher F, Behnam S, et al. “Keratolytic” properties of benzoyl peroxide and retinoic acid resemble salicylic acid in man. Skin Pharmacol Physiol. 2006;19(5):283–289.
8. Kinney MA, Yentzer BA, Fleischer AB Jr, Feldman SR. Trends in the treatment of acne vulgaris: are measures being taken to avoid antimicrobial resistance? J Drugs Dermatol. 2010;9(5):519–524.
9. Shalita A. The integral role of topical and oral retinoids in the early treatment of acne. J Eur Acad Dermatol Venereol. 2001;15(Suppl 3):43–49.
10. Czernielewski J, Michel S, Bouclier M, Baker M, Hensby JC. Adapalene biochemistry and the evolution of a new topical retinoid for treatment of acne. J Eur Acad Dermatol Venereol. 2001;15(Suppl 3):5–12.
11. Thiboutot DM, Gollnick HP. Treatment considerations for inflammatory acne: clinical evidence for adapalene 0.1% in combination therapies. J Drugs Dermatol. 2006;5(8):785–794.
12. Thiboutot DM, Weiss J, Bucko A, et al; Adapalene-BPO Study Group. Adapalene-benzoyl peroxide, a fixed-dose combination for the treatment of acne vulgaris: results of a multicenter, randomized double-blind, controlled study. J Am Acad Dermatol. 2007;57(5):791–799.
13. Gold LS, Tan J, Cruz-Santana A, et al; Adapalene-BPO Study Group. A North American study of adapalene-benzoyl peroxide combination gel in the treatment of acne. Cutis. 2009;84(2): 110–116.
14. Gollnick HP, Draelos Z, Glenn MJ, et al; Adapalene-BPO Study Group. Adapalene-benzoyl peroxide, a unique fixed-dose combination topical gel for the treatment of acne vulgaris: a transatlantic, randomized, double-blind, controlled study in 1,670 patients. Br J Dermatol. 2009;161(5):1180–1189.
15. Balkrishnan R, Bhosle MJ, Camacho F, Fleischer AB, Feldman SR. Prescribing patterns for topical retinoids: analyses of 15 years of data from the national ambulatory medical care survey. J Dermatolog Treat. 2010;21(3):193–200.
16. Gold LS, Cruz A, Eichenfield L, et al. Effective and safe combination therapy for severe acne vulgaris: a randomized, vehicle-controlled, double-blind study of adapalene 0.1%-benzoyl peroxide 2.5% fixed-dose combination gel with doxycycline hyclate 100mg. Cutis. 2010;85(2):94–104.