Nathan S. Trookman, MD, FAAD; Ronald L. Rizer, PhD
Dr. Trookman is from Colorado Springs Dermatology Clinic, Colorado Springs, Colorado, and Dr. Rizer is from Thomas J. Stephens & Associates, Inc., Colorado Research Center, Colorado Springs, Colorado
Disclosure: The authors report no relevant conflicts of interest. Financial support for this study was provided by SkinMedica, Inc.
Abstract
Objective: Desonide hydrogel 0.05%, an effective treatment for mild-to-moderate atopic dermatitis, is United States Food and Drug Administration approved as a treatment for patients as young as three months of age. Previous studies have also demonstrated that this hydrogel formulation of desonide 0.05% improved moisturization and reduced transepidermal water loss. Increased skin hydration has been correlated with improved and sustained integrity of the epidermal barrier in patients with atopic dermatitis. The objective of this clinical noninferiority study was to compare the efficacy of desonide hydrogel 0.05% with desonide ointment 0.05%, the clinical standard for the treatment of mild-to-moderate atopic dermatitis. Design and setting: Randomized, investigator-blinded, parallel-group, noninferiority study in an outpatient setting. Participants: Individuals 12 years of age and older with atopic dermatitis. Measurements: Outcome measures included disease severity, body surface area involvement, subjective assessments of symptoms, corneometry, transepidermal water loss, and the patient’s preference for vehicle attributes. Patients were assessed at Baseline, Week 2, and Week 4. Results: Desonide hydrogel 0.05% was shown, through visual grading assessments and noninvasive instrumentation measurements, to be as effective as generic desonide ointment 0.05% in reducing the signs and symptoms of mild-to-moderate atopic dermatitis in patients aged 12 to 65 years during a four-week period. In addition, patients rated desonide hydrogel significantly better than desonide ointment for absorbability and (lack of) greasiness. Conclusion: Desonide hydrogel, which uses a hydrogel vehicle, was preferred by patients and shown to restore the skin barrier, thus offering an efficacious alternative to desonide ointment.
(J Clin Aesthet Dermatol. 2011;4(11):34–38.)
Atopic dermatitis (AD) is a common, chronic inflammatory skin disorder that most often begins in infancy or childhood.[1] In the United States, an estimated 10 to 20 percent of all infants and young children suffer from symptoms of AD; 65 percent of these patients develop AD in their first year of life, and 85 percent develop AD by age 5.1 More than half (60%) of children who are diagnosed with AD will continue to exhibit at least one symptom of AD into adulthood.[1] The prevalence of AD in adults is estimated at 1 to 3 percent.[2]
The discomfort caused by the symptoms of AD may erode the quality of life for young patients and their caregivers.[3] Children with AD often experience disturbed sleep patterns and sleep loss, which may lead to mood disturbances and behavioral issues and reduced concentration and impaired performance in school.[3] Older children with AD may also experience embarrassment about their appearance, possibly leading to loss of confidence, depression, and social isolation.[3] Thus, timely and effective treatment of AD is desirable.
Treatment of AD focuses on restoring the skin barrier and reducing flares. Developing skin care routines, making lifestyle changes, and avoiding immune system triggers, allergens, and irritants help reduce the itch-scratch cycle of AD.[1] Topical corticosteroids, which have anti-inflammatory and antipruritic properties, have been used for many years to treat the symptoms of AD.[1,4]
Adverse effects of topical corticosteroids, which include atrophy, striae, telangiectasia, burning, and dryness, are correlated with their potency.[5] A possible systemic side effect of repeated use of topical steroids is reversible suppression of the hypothalamic-pituitary-adrenal (HPA) axis.[5] Because drug penetration is greater and more rapid in infants who have thinner strata cornea and increased surface area to body mass ratios, the potential for adverse effects is greatest in younger patients, the same group most likely to have AD.[6,7] To avoid the potential of adverse effects, especially in infants and young children, the least potent topical steroid needed to control the AD should be used.[6]
Desonide is a low-potency (class 6), nonfluorinated corticosteroid with well-established efficacy and safety in the treatment of AD.[5] Available in cream, lotion, foam, ointment, and hydrogel formulations, desonide is the most commonly prescribed low-potency topical corticosteroid by dermatologists in the United States.[7]
The formulation of a topical agent may affect the medication’s delivery by altering its release rate and bioavailability.[6] Vehicle selection has been shown to affect patient acceptance and adherence, thereby influencing treatment outcome.[7] An ideal formulation would be easy to apply and remove, nonirritating, and cosmetically acceptable to the patient.[7]
Desonide hydrogel 0.05% (Desonate® Gel, Intendis, Inc., Morristown, New Jersey), in an aqueous hydrogel vehicle for the treatment of mild-to-moderate AD in patients three months of age and older, provides the established efficacy of desonide in a cosmetically elegant hydrogel vehicle that spreads and is absorbed into the skin easily on application without creating a greasy or tactile residue or leaving a shiny film. It is alcohol-, surfactant-, and fragrance-free.[4,7] Numerous clinical studies have shown the hydrogel 0.05% formulation to be efficacious, well tolerated, and safe.[4,5,8] The hydrogel vehicle has moisturizing properties previously shown to have therapeutic effects, such as improving and sustaining the integrity of the epidermal barrier.[9–12]
This clinical noninferiority study was conducted to compare the efficacy of desonide hydrogel 0.05% with desonide ointment 0.05%, the clinical standard for the treatment of mild-to-moderate AD.
METHODS
A single-center, randomized, evaluator-blinded, parallel-comparison, noninferiority study was conducted between November 2008 and February 2009 to evaluate the relative efficacies of desonide gel 0.05% and generic desonide ointment 0.05% (Fougera & Co., Melville, New York) for the treatment of mild-to-moderate AD. Enrolled patients had clinically verified AD and at least one mild-to-moderate atopic lesion at the start of the four-week trial.
Patients were randomly assigned to desonide hydrogel 0.05% or to desonide ointment 0.05% according to a stratified-randomization scheme. The investigator was blinded to the assignment of test materials; a trial coordinator was responsible for dispensing the test medication and collecting any adverse event information.
The protocol and informed consent agreement for this study was reviewed and approved by an institutional review board (IRB) prior to subject enrollment. Written informed consent was obtained from each subject prior to study enrollment. For patients aged 12 to 17 years, the subject signed an assent form, and the subject’s parent or guardian signed the informed consent.
Patients were instructed to cleanse the affected area and pat dry with a soft towel prior to applying the provided medication. A thin layer of medication was to be rubbed into the affected areas twice daily, in the morning and evening.
The following parameters were assessed at Baseline (Visit 1), Week 2 (Visit 2), and Week 4 (Visit 3):
• Eczema Area and Severity Index (EASI) for each body area affected by AD (head and neck, upper limbs, torso, and lower limbs)—erythema; edema, induration, and papulation; excoriations; and lichenification were assessed at each site and scored on a scale from 0 (absent) to 3 (severe). EASI scores were tallied to obtain a single composite score, which ranged from 0 (no disease anywhere on the body) to 72 (severest disease on all body areas).
• Body surface area (BSA) involvement was assessed as estimated by the clinician.
• Atopic Dermatitis Severity Index (ADSI) for the target lesion—ADSI consisted of a composite score of the signs and symptoms of the target lesion, including erythema, pruritus, exudation, excoriation, and lichenification. Each of these signs and symptoms was scored in half-point increments on a 4-point scale (0=absent; 3=severe). These scores were summed to generate a total ADSI score.
• Target lesion assessment—the severity of the target lesion was scored on a 5-point scale (0=clear; 4=severe AD).
• Subjective irritation symptoms, including burning/stinging, dryness, and itching, were ranked on a 4-point scale (0=absent; 3=severe).
• Corneometry—a CM 825 Corneometer (Courage + Khazaka, Germany) measured the moisture content in the stratum corneum of the target lesions.
• Transepidermal water loss (TEWL) was assessed at the target lesion using a DermaLab (Cortex Technology, Denmark).
• At Weeks 2 and 4, participants also completed a Vehicle Preference Questionnaire.
Statistical Analysis
Visual grading scores and instrumentation measurements at Week 2 (Visit 2) and Week 4 (Visit 3) were statistically compared with Baseline scores using a paired t-test, with changes considered significant at the P<0.05 level. ADSI scores for erythema, pruritus, and lichenification were also individually compared, with mean percentage change from Baseline and incidence of positive responders calculated for all attributes. Analysis of variance (ANOVA) with paired t-tests was conducted to determine whether there were any significant differences between test materials at the P<0.05 level for comparisons based on the average change from Baseline.
RESULTS
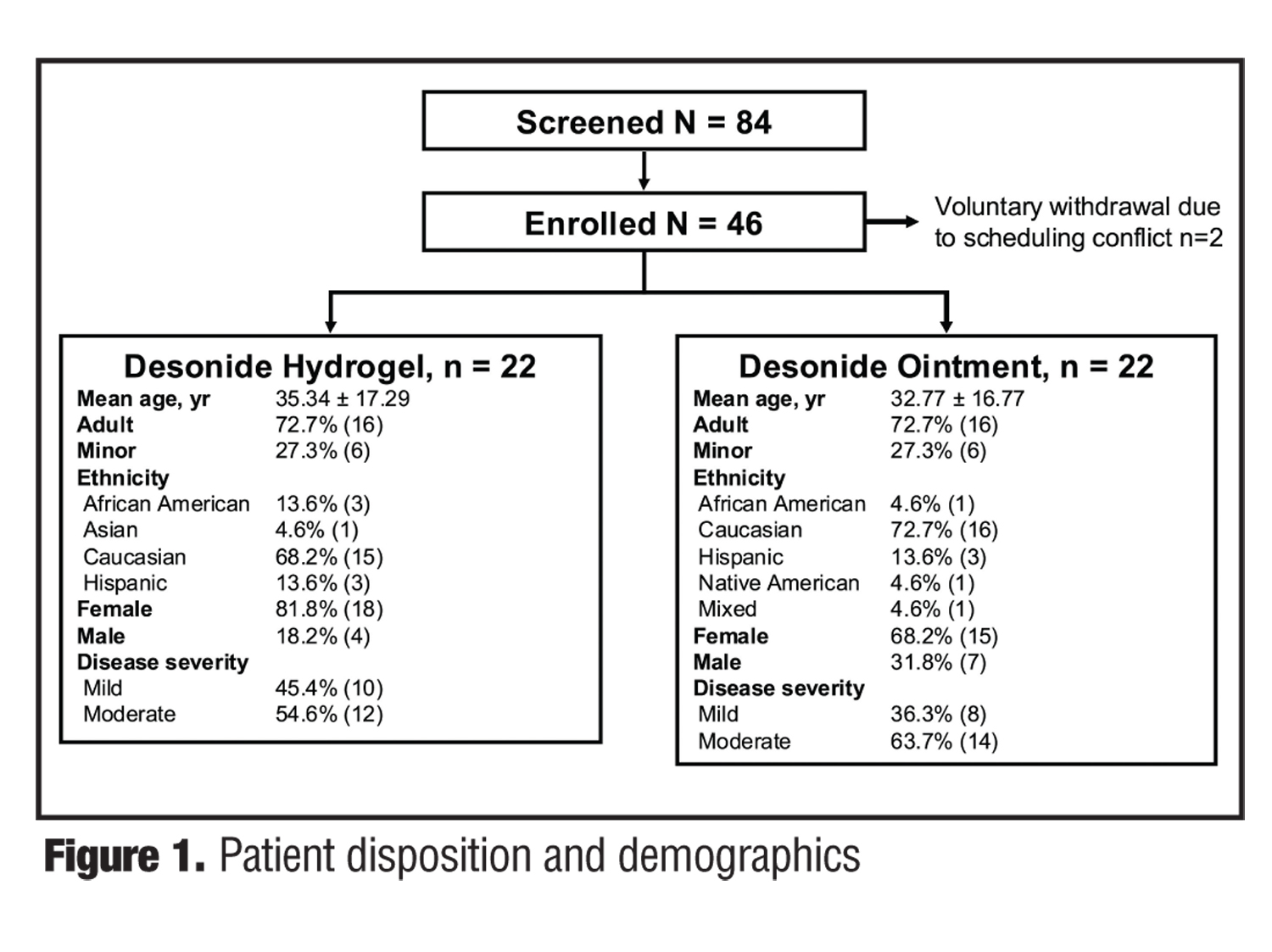
Patient disposition and demographics. Of the 46 patients enrolled, 44 patients completed the study; two patients voluntarily withdrew due to scheduling conflicts. Patient disposition and demographics are detailed in Figure 1. There were five minor protocol deviations, which did not impact trial efficacy results.
{kind=link}
Twenty-two patients received desonide hydrogel 0.05% and 22 patients received desonide ointment 0.05%. The mean usage amount for desonide hydrogel 0.05% was 37.82g, whereas that for desonide ointment 0.05% was 23.59g. The cohorts were ethnically mixed and similar in ratio of adults to minors and in disease severity (Figure 1).
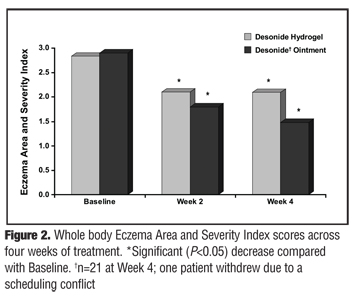
Study outcomes. EASI. Whole body EASI decreased significantly from baseline at Weeks 2 and 4 for desonide hydrogel and desonide ointment (Figure 2), as did overall erythema, excoriation, and lichenification (P<0.05). Erythema, excoriation, lichenification, and edema also showed significant improvements for hydrogel and ointment in the upper limbs; results were not consistently significant in other body regions, likely owing to low baseline severity. Overall, results of the visual grading for upper limbs, lower limbs, head and neck, and torso areas were similar for desonide hydrogel and ointment.
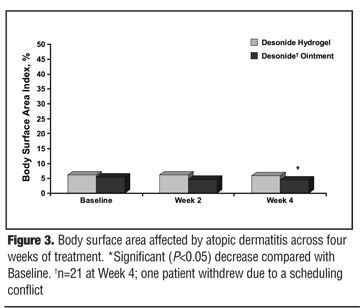
BSA. Overall BSA declined in the treatment groups; this decline from baseline achieved significance for desonide ointment at Week 4 (P<0.05). There was no significant difference in BSA between the desonide hydrogel and ointment groups (Figure 3).
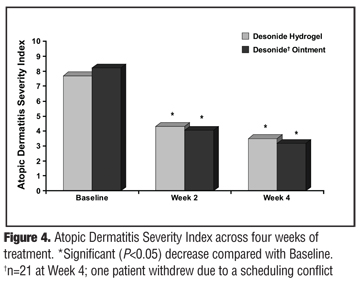
ADSI. Overall ADSI decreased significantly from Baseline at Weeks 2 and 4 for desonide hydrogel and ointment (P<0.05) (Figure 4).
{kind=link}
{kind=link}
{kind=link}
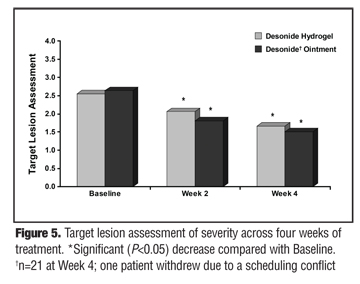
Target lesion assessment. Overall target lesion assessment of severity decreased significantly from Baseline at Weeks 2 and 4 for desonide hydrogel and ointment (P<0.05) (Figure 5).
{kind=link}
Subjective irritation symptoms. Measures of subjective irritation, including burning/stinging, dryness, and itching, declined significantly from baseline at Weeks 2 and 4 for patients receiving both desonide hydrogel and ointment (P<0.05).
Corneometry. There was no significant change from baseline in skin hydration at Weeks 2 or 4 among patients receiving desonide hydrogel or ointment.
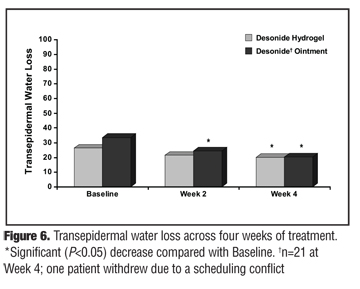
TEWL. TEWL was significantly reduced from Baseline at Week 4 for patients receiving desonide hydrogel and ointment (P<0.05) (Figure 6).
{kind=link}
Patient preference. Patients were generally pleased with the attributes and efficacy of desonide hydrogel and ointment. Desonide hydrogel was rated significantly better than desonide ointment (P<0.05) on both absorption (Week 4) and the (lack of) greasiness of the formulation (Week 2). There were no other significant differences in patient preference.
Adverse events. No adverse events were reported for either group.
DISCUSSION
This single-center, randomized, evaluator-blinded, parallel-comparison, noninferiority study was conducted to compare the efficacy of desonide hydrogel 0.05% versus a generic desonide ointment 0.05% in the treatment of mild-to-moderate AD. Forty-four patients with clinically verified AD and at least one mild-to-moderate atopic lesion at the time of study enrollment were randomly assigned to the desonide hydrogel 0.05% cohort or the generic desonide ointment 0.05% cohort following a stratified randomization scheme. Desonide hydrogel 0.05% and desonide ointment 0.05% successfully treated the symptoms of mild-to-moderate AD. Both formulations were significantly effective in improving EASI scores, ADSI scores, all target lesion parameters, and subjective irritation symptoms. Thus, desonide hydrogel provides relief for the signs and symptoms of AD comparable with desonide ointment 0.05%. This is as expected, given that both formulations contain the same concentration of the active ingredient, desonide, the chief difference between the two medications being the vehicle.
Skin hydration changes were not observed for either formulation during this study; corneometer measurements did not detect significant differences in either the desonide hydrogel 0.05% or desonide ointment 0.05% cohorts at Week 2 or Week 4 compared with Baseline. This finding was surprising given that previous clinical studies demonstrated significant moisturizing and stratum corneum-repairing benefits for desonide hydrogel compared with baseline and active comparators. Trookman et al[10] found that administration of desonide hydrogel twice daily for four weeks significantly improved hydration as early as Week 1, an improvement that lasted until the end of the study (all P<0.002). In a separate study of 10 patients with AD, Trookman et al[9] also found that the hydrogel vehicle provided moisturizing benefits similar to dry skin therapy lotion after two weeks of treatment. Dry, cold weather conditions experienced during the winter months of this study may account for the atypical results seen here.
In contrast with the lack of effect on skin hydration, desonide hydrogel 0.05% and desonide ointment 0.05% demonstrated significantly improved stratum corneum barrier integrity at Week 4. Previous studies also demonstrated a TEWL-reducing effect for desonide hydrogel and its vehicle. Desonide hydrogel 0.05%–treated lesions further displayed significant improvements in stratum corneum barrier function, with TEWL measurements significantly decreased after as little as one week of treatment.11 In the Trookman study of the hydrogel vehicle, two weeks of treatment with hydrogel resulted in a significant reduction in TEWL similar to that seen with dry skin therapy lotion.[9]
In the Vehicle Preference Questionnaire, desonide hydrogel was also rated significantly more favorably than desonide ointment for absorbability and (lack of) greasiness. In addition, several previous studies suggest that when asked to consider a hydrogel relative to other vehicle options, patients with AD prefer the hydrogel vehicle. In one study, adult patients with mild-to-moderate AD (N=51) who applied a small sample of the hydrogel vehicle rated it very favorably, with the majority stating that the hydrogel vehicle was substantially superior or superior to other corticosteroid vehicle formulations they had used in the past.[11] In a larger survey of patients using desonide hydrogel for the treatment of AD (N=1025), patients who had previously used a prescription medication for AD (n=692) similarly reported significantly higher treatment satisfaction with desonide hydrogel than with prior medications.[13]
In a separate study, patients (or parents of patients) with mild-to-moderate AD (N=41) who were treated with desonide hydrogel were given samples of different vehicles and asked to rate them relative to each other. These patients reported similarly positive appraisals, significantly preferring hydrogel versus ointment (P<0.001), cream (P<0.01), foam (P<0.01), and oil (P<0.001) vehicles.[14] In the current study, patients were not given an opportunity to sample both desonide hydrogel and desonide ointment. Average ratings of product absorbability and (lack of) greasiness were significantly higher among patients receiving desonide hydrogel than among patients receiving desonide ointment. Patients may express a stronger preference for hydrogel-based formulations when given a choice between formulations than when each formulation is presented in isolation.
This preference for desonide hydrogel is likely to encourage adherence to treatment. The preference study[14] described above also utilized Medication Event Monitoring System (MEMS) caps to monitor adherence and found that rate of decline in adherence with desonide hydrogel was much lower than in a previously reported adherence study,[15] which examined the adherence of patients using 0.1% triamcinolone ointment. The current study did not utilize an adherence assessment of this nature; however, it was noted that patients utilized more desonide hydrogel than desonide ointment (37.82g vs. 23.59g). Although the cause of this difference is unknown, one potential explanation is greater treatment adherence among patients in the desonide hydrogel group.
SUMMARY
Desonide hydrogel 0.05% is a safe, effective, well-tolerated, low-potency, class 6, topical corticosteroid for the treatment of mild-to-moderate AD. It is FDA approved as a treatment for patients as young as three months of age. The hydrogel vehicle has been shown to improve moisture content in the stratum corneum, thereby improving the epidermal barrier integrity. In the present study, desonide hydrogel 0.05% was demonstrated to be as efficacious as generic desonide ointment 0.05% in patients with mild-to-moderate AD. In addition, patient rankings of absorbability and (lack of) greasiness were significantly higher among patients receiving desonide hydrogel than among those receiving desonide ointment. Previous studies conducted with desonide hydrogel suggest that the hydrogel vehicle confers preferred status on this desonide formulation compared with ointment, which has been associated with improvement in adherence. Thus, taken together, these results suggest that desonide hydrogel 0.05% is a preferred formulation, with efficacy comparable with that of desonide ointment.
References
1. National Institute of Arthritis and Musculoskeletal and Skin Disease. Handout on Health: Atopic Dermatitis. May 2009. http://www.niams.nih.gov/Health_Info/Atopic_Dermatitis/default.asp. Accessed on: July 24, 2010.
2. Leung DY, Boguniewicz M, Howell MD, et al. New insights into atopic dermatitis. J Clin Invest. 2004;113(5):651–657.
3. Lewis-Jones S. Quality of life and childhood atopic dermatitis: the misery of living with childhood eczema. Int J Clin Pract. 2006;60(8):984–992.
4. Gelbard CM, Hebert AA. Desonide hydrogel: advances in vehicle technology. Expert Rev Dermatol. 2009;4(1):23–27.
5. Eichenfield LF, Basu S, Calvarese B, Trancik RJ. Effect of desonide hydrogel 0.05% on the hypothalamic-pituitary-adrenal axis in pediatric subjects with moderate-to-severe atopic dermatitis. Pediatr Dermatol. 2007;24(3):289–295.
6. Lambe MB. Topical agents in infants. Newborn Infant Nurs Rev. 2001;1(1):25–34.
7. Kircik L, Del Rosso J. A novel hydrogel vehicle formulated for the treatment of atopic dermatitis. J Drugs Dermatol. 2007;6(7):718–722.
8. Hebert AA, Cook-Bolden FE, Basu S, et al. Safety and efficacy of desonide hydrogel 0.05% in pediatric subjects with atopic dermatitis. J Drugs Dermatol. 2007;6(2):175–181.
9. Trookman NS, Rizer RL, Ford RO, Trancik RJ. Atopic dermatitis: advantages of a novel hydrogel vehicle. Presented at: 65th Annual Meeting of the American Academy of Dermatology; February 2–5, 2007; Washington, DC.
10. Trookman NS, Rizer RL, Ford RO, Gotz V. The stratum corneum and atopic dermatitis: moisturizing advantages of a novel desonide hydrogel treatment. Presented at: 66th Annual Meeting of the American Academy of Dermatology; February 1–5, 2008; San Antonio, TX.
11. Trookman NS, Rizer RL, Ford R, Trancik RJ. Topical vehicle preferences in atopic dermatitis patients: evaluating a novel hydrogel vehicle. Presented at: 65th Annual Meeting of the American Academy of Dermatology; February 2–6, 2007; Washington, DC.
12. Trookman NS, Rizer RL, Ho ET, et al. Randomized, evaluator-blind, parallel-group comparison study of the tolerability and subject preference of a benzoyl peroxide microsphere wash compared to a gentle non-medicated cleansing wash in mild to moderate acne. Presented at: Summer Meeting of the American Academy of Dermatology; July 30–August 2, 2009; Boston, MA.
13. Kerney DL, Ford R, Gotz V. Patient assessment of desonide hydrogel for the treatment of mild-to-moderate atopic dermatitis. Presented at: 67th Annual Meeting of the American Academy of Dermatology; March 6–10, 2009; San Francisco, CA.
14. Yentzer BA, Camacho FT, Young T, et al. Good adherence and early efficacy using desonide hydrogel for atopic dermatitis: results from a program addressing patient compliance. J Drugs Dermatol. 2010;9(4):324–329.
15. Krejci-Manwaring J, Tusa MG, Carroll C, et al. Stealth monitoring of adherence to topical medication: adherence is very poor in children with atopic dermatitis. J Am Acad Dermatol. 2007;56(2):211–216.