Jason J. Emer, MD; Claire Wolinsky, BS
The Mount Sinai School of Medicine, Department of Dermatology, New York, New York
Abstract
The treatment of many dermatological disorders, such as autoimmune and immune-mediated diseases, consists of the use of systemic corticosteroids alone or in combination with other steroid-sparing immunosuppressants. Often, these treatment regimens are sufficient to control disease activity with relatively few side effects if monitored by a diligent physician. Some patients, however, may be refractory to treatment or develop intolerable side effects from therapy. For these patients, alternative treatment modalities with less toxicity and greater efficacy are required. Rituximab is a genetically engineered, chimeric monoclonal antibody directed against the B-cell lineage specific CD20 antigen. Originally developed for the treatment of B-cell non-Hodgkin’s lymphoma, rituximab has increasingly been used to treat a variety of autoimmune and immune-mediated disorders, such as rheumatoid arthritis, pemphigus diseases, systemic lupus erythematosus, dermatomyositis, and idiopathic thrombocytopenic purpura to name a few. Since very few randomized, controlled, clinical trials exist regarding the use of rituximab in the treatment of dermatological disorders, guidelines for the off-label use of this medication come from anecdotal case reports and cohort studies. Further clinical studies are needed to validate the safety and efficacy of rituximab therapy in dermatological disorders. Until then, we present a literature review of the emerging use of this B-cell depletion therapy.
(J Clin Aesthetic Dermatol. 2009;2(5):29–37)
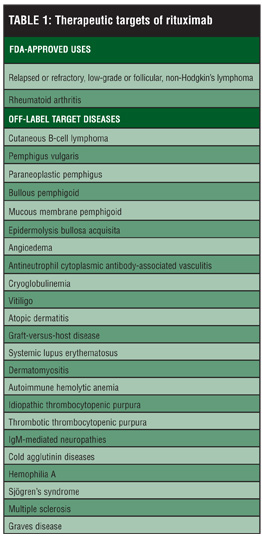
Rituximab (Rituxan®, Genentech, South San Francisco, California) is a unique, chimeric, murine-human monoclonal antibody directed against the B-lymphocyte specific antigen CD20 expressed only by pre-B (hematopoietic) and mature (peripheral) B cells.[1] CD20 is suspected to play a significant role in the regulation of cell-cycle initiation and differentiation of the B-cell lineage, evident by a rapid B-cell depletion after treatment, which can be maintained for 6 to 12 months.[2,3] Three mechanisms have been proposed for this finding, including the following: 1) complement-dependent cytotoxicity, 2) antibody-dependent cellular cytotoxicity, and 3) induction of apoptosis.[4–6] Hematopoietic stem cells and plasma cells are spared with rituximab treatment due to their lack of the CD20 antigen; thus, serum immunoglobulin levels typically remain stable.[7–9] Until recently, the primary use of rituximab has been in the induction of B-cell depletion for the treatment of B-lymphocyte malignancies, such as relapsed or refractory, low-grade or follicular, CD20-positive, B-cell non-Hodgkin’s lymphoma (NHL). Rituximab is clinically well tolerated with rare occurrences of serious adverse events, making it an appealing alternative treatment option in patients with refractory autoimmune or immune-mediated conditions (Table 1).[10–12]
{kind=link}
Since 2006, rituximab has also been approved for use in patients with moderate-to-severe rheumatoid arthritis (RA) refractory to disease-modifying antirheumatic drugs (DMARD) and/or anti-tumor necrosis factor therapy (TNF).[13,14] The approval for rituximab in RA was established by multiple clinical trials that proved that B-cell depletion therapy significantly helped patients with active RA who had previously failed other therapies including DMARD treatment.[15–17] It was hypothesized and proven that B cells played a significant role in the pathophysiology of RA by their function in the following: 1) the production of autoantibodies, 2) antigen presentation, 3) regulation of T-cell activation, and 4) the production of pro-inflammatory cytokines.18,19 As more is understood about rituximab and its potential as a targeted biologic treatment in various autoimmune and immune-mediated diseases, clinicians are paving the way for the expanding use of this medication in the field of dermatology.
Mechanism of Action
Rituximab is a chimeric monoclonal antibody of the immunoglobulin G1 (IgG1) sub-class, comprising a murine variable region (Fab region) and a human constant region (Fc region). The Fab region has variable sections that define a specific target antigen so the antibody can attract and secure an exclusive antigen, specifically the binding of rituximab (IgG1) to CD20 on pre-B and mature B lymphocytes. The Fc region is the tail end of the antibody that interacts with cell surface receptors to activate the immune system, in this case a cascade of events leading to the ultimate depletion of circulating B lymphocytes via complement-dependent cell lysis, antibody-dependent cellular cytotoxicity, and apoptosis.[20] Evidence suggests that the foremost mechanism of B-cell elimination is complement mediated, as a correlation was found with rituximab treatment and the abundance of complement regulatory proteins on target cells.[21]
CD20 is expressed exclusively on pre-B and mature B lymphocytes; thus, treatment with rituximab spares hematopoietic stem cells and plasma cells because of a lacking CD20 antigen. This selectivity allows for B-cell regeneration from unaffected hematopoietic precursors as well as the continued production of immunoglobulins from plasma cells. B-cell regeneration into peripheral circulation has been shown to occur at approximately 6 to 12 months following therapy, and serum immunoglobulins have not been shown to decrease significantly.[2,3,7–9,22] In systemic lupus erythematosus (SLE) and RA, rituximab resulted in the reconstitution of B cells with a new immunoglobulin rearrangement pattern, pointing to naïve B lymphocytes that are produced in the bone marrow rather than from depleted memory B cells,[23,24] suggesting that treatment with rituximab may result in more complete remissions as the newly committed naïve B cells may differentiate into nonautoantibody-producing plasma cells.[25] The removal or transitory decrease in mature CD20-positive, B lymphocytes with commitment to the differentiation into autoantibody-producing plasma cells is what makes rituximab unique and attractive to autoimmune and immune-mediated diseases.
In addition to a direct depletion of B cells by various mechanisms, rituximab may also act on other immune cells such as autoreactive T-effector cells, regulatory T cells, and monocyte-derived macrophages.[20] CD4+ T cells are crucial for the autoantibody response against the desmosomal adhesion molecules desmoglein 3 (Dsg3) and Dsg1 in patients with pemphigus vulgaris (PV). Eming et al[26] found a significant reduction in Dsg3-specific CD4+ T cells after administering rituximab in patients with PV. Eleven patients with extensive PV were treated with rituximab at 375mg/m2 given intravenously (IV) once weekly for four weeks. Frequencies of autoreactive CD4+ T cells in the peripheral blood were determined, the clinical response was evaluated, and serum autoantibody titers were quantified. Rituximab induced peripheral B-cell depletion for 6 to 12 months, leading to a dramatic decline of serum autoantibodies and significant clinical improvement in all PV patients. The quantities of Dsg3-specific CD4+ T cells also decreased significantly. The authors concluded that the response to rituximab in PV involved two mechanisms: 1) the depletion of autoreactive B cells and 2) the specific down-regulation of Dsg3-specific CD4+ T cells.
With an increased understanding of the intricate interaction between B cells and other immune cells, rituximab therapy may be used to indirectly decrease the production of T-cell modulating cytokines, interfere with the presentation and processing of autoantigens, and reduce activation of autoreactive T cells.[27] The success of rituximab in T-cell-mediated autoimmune diseases—such as RA, and in conditions not directly linked to autoantibody production, such as atopic dermatitis (AD)[28]—supports the possible use of rituximab for the benefit of these alternative mechanisms. Nonetheless, the exact contribution of each mechanism to the various proposed diagnoses remain unclear at this time.[1,29]
Dosage and Administration
Currently, there are two official US Food and Drug Administration (FDA)-approved dosing regimens for the use of rituximab (Table 2). In NHL, rituximab is given as an IV infusion of 375mg/m2 once weekly for 4 to 8 consecutive weeks as a single agent or in combination with chemotherapy regimens.[30] In RA, the dosing is two IV infusions of 1,000mg given two weeks apart (Days 1 and 15), along with the administration of methotrexate.[31–33]
{kind=link}
Although these protocols are the standard approved and most common, there is no official consensus on the most efficacious and safest dosing of rituximab in off-label applications. In SLE, dose-escalation studies revealed no difference in clinical remission or B-cell depletion with a single IV infusion of 100mg/m2 compared to 375mg/m2 or four weekly infusions at 375mg/m2.[24,34,35] In RA, there was no additional benefit found when administering four versus two weekly IV infusions of 375mg/m2.[36] Further, findings have indicated that patients treated with repeated courses of rituximab have sustained clinical responses with no new adverse events.[37,38] In autoimmune blistering disorders, the most commonly reported dosing schedule is 375mg/m2 administered as an IV infusion weekly for four consecutive weeks, as used in NHL. Schmidt et al[39] reported complete remission in one PV patient after only two rituximab treatments. Others have reported a delay in clinical response of rituximab therapy in a small number of patients with PV requiring the need for an increased infusion number or an induction cycle with maintenance treatments.[40,41]
Regimens using rituximab concurrently with other medications (such as immunosuppressants and/or immuno-modulators) have also been reported in the literature. Specifically, high-dose intravenous immunoglobulin (IVIG) has proven beneficial for several autoimmune diseases and has therefore been investigated for its use in combination with rituximab.[13,42] Ahmed et al[42] reported clinical remission and a reduction of autoantibodies in several PV patients treated with the combination of rituximab (375mg/m2) and IVIG (2g/kg). In 11 patients, a total of 10 rituximab IV infusions per patient were applied in combination with six IVIG treatments over six months. In the remaining 26 patients, four rituximab IV infusions were administered at weekly intervals. Adjuvant immunosuppressant therapy was continued in all but three published cases of rituximab-treated autoimmune bullous disorders and was generally tapered according to clinical response.[27] There have also been reports of success in using intralesional injections for primary cutaneous B-cell lymphoma.[43]
Adverse Events
The incidence of serious adverse events with rituximab is very low and generally well tolerated aside from common, mild, infusion-related reactions that manifest as fever, chills, headache, weakness, nausea, pruritus, and rash.[29] Temporarily stopping or slowing the IV infusion often reverses or relieves symptoms, and premedication with analgesics (acetaminophen), antihistamines (diphen-hydramine), and glucocorticoids (methylpred-nisolone) can control such events.[44,45] After the first infusion, infusion-related reactions are much less common. Approximately 80 percent of fatal infusion reactions occur with the first infusion.[30]
Increased infections are always of concern in patients on any immunosuppressive therapy, especially in patients on combinational treatment because of compounded immunosuppression. In a recent study of rituximab for the treatment of RA, infections occurred in 35 percent of patients in the rituximab group compared to 28 percent in the placebo group. Further, serious infections occurred in two percent of the rituximab group compared to one percent in the placebo group.[33] As noted before, immuno-globulin levels do not decrease dramatically with rituximab treatment, thus maintaining protective humoral immunity while on treatment.
Black box warnings are documented for rituximab and include the following: tumor lysis syndrome, fatal infusion reactions, and severe mucocutaneous reactions including Stevens-Johnson syndrome and toxic epidermal necrolysis. Other worrisome serious adverse events included in the package insert include the following: hepatitis B re-activation, progressive multifocal leuko-encephalopathy infection, hypersensitivity reactions (such as anaphylaxis, serious pulmonary events, cardiac arrhythmias, and renal failure), hematological abnormalities (cytopenias and hemolytic anemia), and gastrointestinal perforation and obstruction. Variables including the extremes of age, concomitant immunosuppressive treatment, poor general medical health, and patients with an underlying malignancy may increase the likelihood that a patient will experience an adverse event.
Another concern with the use of rituximab is the formation of human antichimeric antibodies (HACAs). The development of HACAs has been seen at a higher incidence in patients with autoimmune diseases[34] when compared to those with lymphoma.[22,46] Nonetheless, it is unclear what role HACAs play with regard to the clinical efficacy and adverse events of rituximab therapy.[45] As current safety information is based on treatment in NHL and RA patients, strict caution should be taken when using rituximab medication as an off-label indication for other disorders. There is suggestion that rituximab therapy carries less risk of adverse events in treating patients with RA versus NHL.[13] Even so, without many controlled, clinical trials assessing the safety and efficacy of rituximab for off-label indications, such as dermatological disease, future research is needed to more clearly define clinical guidelines for physicians to follow.
Off-label Indications for Rituximab in Dermatology
Primary cutaneous B-cell lymphoma (PCBCL). PCBCL has been classified into three major histological subtypes by the World Health Organization (WHO): 1) follicle center, 2) marginal zone, and 3) diffuse large B-cell lymphoma.[47] Follicle center and marginal zone B-cell lymphomas follow a more indolent course with a superior prognosis, while diffuse large B-cell lymphoma carries a much poorer prognosis.[48] Multiple case reports in all three subgroups have demonstrated success with both systemic and intralesional rituximab.[50–53]
Gellrich et al[51] reported an overall response rate of 90 percent (70% complete and 20% partial) in a study using eight weekly IV infusions of rituximab 375mg/m2 as monotherapy in 10 patients with PCBCL. The median duration of remission was 23 months. The authors concluded that rituximab was an effective and less toxic alternative treatment in a subset of patients with PCBCL (relapsed and/or aggressive disease, elderly patients, and multiple lesions). Another study performed by Valencak et al[48] demonstrated complete clinical remission in 14 of 16 patients in the study with 11 patients only requiring four weeks of consecutive rituximab IV infusion at 375mg/m2. The remaining five patients required six weeks of consecutive therapy to achieve clinical remission. The results suggested that single-agent treatment with rituximab appeared to be feasible, safe, and have a high rate of durable remissions. The authors concluded that rituximab is an attractive treatment option for PCBCL and should be directly compared with local radiotherapy.
While intralesional injection of rituximab permits a smaller dose of medication, the recurrence rate may be higher. In a retrospective study by Fink-Puches et al,[53] rituximab therapy was well tolerated and found to be an effective treatment for PCBCL. They discovered that in comparison to IV administration, intralesional application of the drug allowed for the use of lower dosages. Two patients treated with systemic rituximab achieved complete remission and the same was observed in 6 of 7 patients after 1 to 8 cycles of intralesional treatment (10mg per lesion three times weekly until clear). A local recurrence was observed in one patient after 27 months of follow up, and in two patients, recurrences developed at other body sites after 12 and 14 months of follow up. No severe side effect was noted except for slight pain during intralesional injection.
Pemphigus diseases. Autoimmune blistering diseases, including pemphigus diseases, are associated with the production of autoantibodies against specific components of the structural support found in the epidermis and dermoepidermal junction. These support proteins are essential for the integrity of the skin; thus, severe skin disease ensues if this structural support is damaged.
Standard therapy for autoimmune bullous diseases typically includes long-term systemic corticosteroids as sole therapy or in combination with other steroid-sparing immunosuppressants and/or IVIG. Severe adverse events, such as sepsis from systemic corticosteroids and immuno-suppressive treatments, are the major contributing factors of the high mortality rate (5–10%) in PV.[15] For most patients, these classical treatments are sufficient to induce remission, but others may be refractory to treatment or be unable to tolerate the many side effects. The importance of finding alternative, less toxic, more efficacious treatments in such patients led to initial trials of rituximab in PV. Rituximab has since been successfully applied to the treatment of autoimmune blistering disorders, with success manifesting in multiple case reports and cohort studies. Even a recent consensus statement was published regarding the use of rituximab in the treatment of autoimmune bullous skin diseases.[3]
The overall goal of rituximab treatment in autoimmune bullous disorders is the long-term depletion of pathogenic, autoantibody-producing B cells, as a correlation exists between the depletion of CD20-positive B cells and clinical improvement.[42,54–56] In paraneoplastic pemphigus (PNP), which is a lymphoma-associated autoimmune phenomena, malignant B-cell clones cause the production of autoreactive antibodies to various components of desmosomes and hemidesmosomes. Rituximab has shown an excellent response, unless there was progression of the underlying malignancy.[57,58] Two prospective clinical studies on the use of rituximab in PV have shown excellent clinical remissions.[42,55]
Most clinicians have demonstrated an excellent clinical response to rituximab in severe pemphigus, even though the understanding of its success is still debated. Although a decline of B cells is correlated with clinical remission, decreases in autoantibody titers have not been consistently found in clinically responsive patients. There is suggestion that various epitopes of autoantibodies exist and some are more pathogenic than others. Specifically, the desmoglein-specific antibody IgG1 subtype may be less pathogenic and may predominately account for the documented high antibody titers as compared to the IgG4 antibody subtype, which may be more virulent and most responsible for severe disease.[22,59] Rituximab may eliminate the precursor cells to pathogenic autoantibody-producing, short-lived plasma cells, but may not act on long-lived plasma cells often responsible for the high titers of serum autoantibodies sometimes seen in treated pemphigus patients.[55] Memory B cells, which express the CD20 antigen and are susceptible to rituximab, may produce the more pathogenic antibodies and plasma cells, which do not express CD20 and are not susceptible to rituximab, may produce the less pathogenic antibodies. Either theory relies on the selectivity of rituximab to targeting cells with only the CD20 antigen.[60,61]
As discussed, rituximab is believed to exert its effect by eliminating pathogenic B cells for more than six months, after which a new generation of B lymphocytes emerge secreting a different set of immunoglobulins than the previous autoantibodies produced by past pathogenic B cells. Although many patients have been found to relapse at the time of B-cell recurrence without any good evidence to explain these relapses, it may be that patients who experience disease recurrence may have an initially incomplete depletion of B cells. To support this, some studies have associated higher numbers of memory B cells in patients with RA who relapse.[23] Another theory argues that long-lived plasma cells in the bone marrow down-regulate CD20 and are spared by rituximab.[54] Alternatively, relapse may be due to the various other types of immune cells spared by rituximab. Autoreactive T cells may re-stimulate the remaining autoreactive B cells or the new lineage of B cells and lead to relapse.[27] Repeating cycles of rituximab in patients with relapse has been used frequently, although there is concern over the long-term effects of a prolonged reduction or depletion of B cells on humoral and cellular immunity.[55]
Currently, the optimal dosing regimen for the use of rituximab in autoimmune blistering diseases is not known. Recent literature has allowed concurrent systemic corticosteroids or immunosuppressive therapy at least until partial clinical response has been obtained. Most studies for PV have been conducted using rituximab at 375mg/m2 IV for four consecutive weeks with improvement noted at 2 to 6 weeks.[22] Complete remission may be seen several weeks after initial improvement and has been seen as late as 360 days.[55] Few studies have extended past one year; thus, the long-term safety and efficacy of rituximab in autoimmune blistering disorders is still largely unknown. Rituximab has been well-tolerated in most cases; however, four serious infections have been reported (including sepsis and pneumonia), indicating a need for the close surveillance of PV patients undergoing treatment with rituximab.[29]
It should also be noted that there are cases documenting success using rituximab therapy for other similar diseases, such as the subepidermal blistering autoimmune disorders—bullous pemphigoid, epidermolysis bullosa acquisita, and mucous membrane pemphigoid.[3,27]
Dermatomyositis (DM). DM is a systemic inflam-matory myopathy with characteristic cutaneous findings of heliotrope rash and Gottron papules. Of the five criteria that aid in diagnosing this disorder, four relate to the muscle disease (progressive proximal symmetrical weakness, elevated muscle enzyme levels, abnormal findings on electromyograms, and abnormal findings from muscle biopsy) and the fifth criterion is of cutaneous disease, such as the aforementioned characteristic findings and others, such as malar erythema, poikiloderma in a photosensitive distribution, violaceous erythema on the extensor surfaces, and periungual and/or cuticular changes. The standard of care in treatment includes systemic corticosteroids with or without steroid-sparing immunosuppressive agents as well as diligent sun-exposure avoidance. Similar to the treatment of pemphigus diseases, these first-line therapies carry significant risk of toxic side effects and a number of patients may be unresponsive to mono or combinational therapies.
The pathogenesis of the cutaneous disease is poorly understood, but it is believed that similarities exist with that of SLE, in which T cells are involved and antibody-mediated cell cytotoxicity plays a role. There are still many uncertainties regarding the role of B cells in DM, but it is believed that a humoral-mediated (autoantibodies) activation of the complement leads to inflammation and necrosis of endothelial cells allowing for activated T cells to migrate into muscle causing ischemia.[62,63] The role of microvascular injury in skin disease is yet to be fully elucidated. Whereas perivascular B cells dominate in muscle biopsies, mainly T cells are seen in skin biopsies.[64] Rituximab may act to decrease B-cell production of one of the defined or yet unidentified autoantibodies, similar to its role in the treatment of pemphigus diseases. Alternatively, it may act through the dysregulation of B- and T-cell interactions to disrupt the expansion of autoreactive T-cell populations as suggested in SLE.[65,66]
Several patients with recalcitrant DM have demonstrated positive clinical responses to rituximab.[67,68] Only one pilot study has described the use of rituximab in six patients with DM.[69] In this study, patients received four weekly IV infusions of rituximab at 100mg/m2 (3 patients) or 375mg/m2 (3 patients). Patients were continued on concomitant immunosuppressive medications during the trial. All patients had significant reduction of cutaneous and muscle disease.
In a small cohort, Dinh et al70 reported marked clinical improvement in cutaneous disease of DM, specifically the heliotrope rash and the violaceous poikiloderma were the most responsive to treatment. Alternatively, Chung et al[71]reported B-cell depletion therapy with rituximab had only a modest effect on muscle disease and a limited effect on skin disease in their cohort of patients with DM. A larger Phase II/III trial is currently underway assessing the use of rituximab in adult and pediatric DM.[72]
Graft-versus-host disease (GVHD). Sixty to 70 percent of individuals are affected by chronic GVHD after allogenic stem cell transplant.[73] Forty percent of these patients are refractory to conventional therapies, such as prednisone and cyclosporine, and experience an average mortality of 26 percent.[74] Patients with refractory GVHD are usually treated with several salvage therapies primarily targeted at T cells, such as mycophenolate mofetil, sirolimus, daclizumab, thalidomide, and alemtuzumab or targeted at cytokines, such as anti-TNF monoclonal antibodies.
GVHD has been regarded as a T-cell-mediated disease in which donor-derived, alloreactive T cells recognize the recipient as foreign. These pathological T cells attack target tissues directly by cytotoxic attack, by secretion of inflammatory cytokines, such as interleukin-1 (IL-1), TNF-a, IL-6, and interferon-g (IFN-g), and through the promotion of B-cell activation and antibody production.[74] Tissue damage eventually leads to fibrosis and loss of function. An association between the presence of antibodies directed against Y chromosome-encoded minor histocompatibility antigens and the occurrence of chronic GVHD supports the use of an anti-B cell directed therapy.[75] The role of B cells in the pathogenesis of GVHD is supported by several case studies documenting a positive clinical response with the use of rituximab.[73,76–78]
In the largest study thus far, Cutler et al[73] reported on 21 patients with refractory chronic GVHD who had lichenoid and sclerodermatous changes. Patients were treated with one, two, or three cycles of four weekly IV infusions of rituximab at 375mg/m2. Patients were allowed to continue stable doses of other immunosuppressive medications throughout the trial. The overall clinical response rate was 70 percent, including two patients who had complete resolution and were able to discontinue corticosteroid therapy. The study further highlighted that cutaneous and musculoskeletal manifestations of GVHD were more amenable to treatment with rituximab than were mucous membrane and hepatic manifestations.
Other Dermatological Applications of rituximab
Vasculitis. Rituximab use in antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) has been reported extensively in the literature via multiple case reports, case series, and prospective, open-label trials. In addition to AAV, case reports suggest rituximab is also efficacious in cryoglobulinemic vasculitis, Churg-Strauss syndrome, and small vessel vasculitis in patients with previous lymphoma.[22] The exact role of rituximab in AAV is undefined, as B-cell depletion therapy has not correlated well with disease activity and ANCA titers.[79,80] The utility of rituximab in treating granulomas remains unclear as there appears to be conflicting evidence on outcomes in Wegener’s disease.[81,82] Nonetheless, as vasculitis is a type-III hypersensitivity reaction involving immune-complex associated disease states, decreased antibody production by rituximab appears to be a favorable therapeutic intervention overall.
Atopic dermatitis (AD). AD is a chronic inflammatory skin condition manifested by severe pruritus and flaring eczematous lesions resulting from a complex interaction between IgE-bearing antigen presenting cells, T-cell activation, mast-cell degranulation, keratinocytes, eosinophils, and a combination of immediate and cellular immune responses.[83] Mild disease is often managed with topical emollients and devices, glucocorticoids, and calcineurin inhibitors. However, severe disease frequently requires systemic treatment with oral immunosuppressives (glucocorticoids, cyclosporine, mycophenolate mofetil, azathioprine, or leflunomide) or injectable biologic medications (anti-TNF, T-cell inhibitors, or anti-IgE).
Theoretically, B-cell depletion therapy could treat the underlying pathogenesis of AD as B cells and plasma cells have long been presumed to be responsible for the high levels of serum IgE found in individuals with AD. Under this assumption, Simone et al[30] treated six patients with a diagnosis of severe AD with rituximab IV infusions at 1,000mg administered two weeks (Days 1 and 15) apart for a total of two dosages. They monitored clinical parameters (eczema area and severity index [EASI] and pruritus), total and allergen-specific serum IgE levels, skin histology, and inflammatory cells and cytokine expression in the skin and peripheral blood before and after therapy. All patients showed an improvement of skin symptoms within 4 to 8 weeks with significantly decreased EASI scores. Histological alterations, such as spongiosis, acanthosis, and dermal infiltrate, including T- and B-cell numbers, also dramatically improved. However, whereas peripheral B cells were below detectable levels as a consequence of rituximab administration, skin B cells were reduced by approximately 50 percent only. Expression of IL-5 and IL-13 were also reduced after therapy. Moreover, whereas allergen-specific serum IgE levels were not altered, Simone et al[30] observed a slight reduction in total IgE concentrations in the blood. The overall conclusion was that B cells play a major role in the pathogenesis of AD and treatment with rituximab lead to an impressive improvement of AD in patients with severe disease. On the other hand, these convincing initial results were not confirmed in a Czech pilot study in which two patients were treated with rituximab.[84] Further case reports and clinical trials will help to clarify the role of rituximab in the treatment of AD.
Future Potential Applications for Rituximab in Dermatology
According to the literature, it may be beneficial to use rituximab in the treatment of scleroderma, vitiligo, discoid or cutaneous lupus erythematosus, idiopathic thrombo-cytopenic purpura, angioedema, Castleman’s disease, and Schnitzler syndrome.
Conclusion
Although currently only approved for use in the treatment of NHL and RA, rituximab has demonstrated therapeutic efficacy in a variety of autoimmune and immune-mediated dermatological conditions in which traditional therapy has failed or caused significant intolerance. Until further controlled clinical studies are performed to validate the safety and efficacy of rituximab therapy in dermatological disorders, information regarding the off-label usage of this medication will come from anecdotal case reports and cohort studies. In the majority of patients, rituximab is safe and tolerable with only mild, infusion-related, and infectious complications, although strict care and guidance should be followed with each patient treated as the long-term efficacy, tolerability, and dosing in dermatological conditions has not been firmly established.
References
1. Reff ME, Carner K, Chambers KS, et al. Depletion of B cells in vivo by a chimeric mouse human monoclonal antibody to CD20. Blood. 1994;83(2):435–445.
2. Arin MJ, Engert A, Krieg T, Hunzelmann N. Anti-CD20 monoclonal antibody (rituximab) in the treatment of pemphigus. Br J Dermatol. 2005;153(3):620–625.
3. Hertl M, Zillikens D, Borradori L, et al. Recommendations for the use of rituximab (anti-CD20 antibody) in the treatment of autoimmune bullous skin diseases. J Dtsch Dermatol Ges. 2008;6(5):366–373.
4. Plosker GL, Figgitt DP. Rituximab: a review of its use in non-Hodgkin’s lymphoma and chronic lymphocytic leukaemia. Drugs. 2003;63(8):803–843.
5. Kimby E. Tolerability and safety of rituximab (MabThera). Cancer Treat Rev. 2005;31(6):456–473.
6. Johnson PW, Glennie MJ. Rituximab: mechanisms and applications. Br J Cancer. 2001;85(11):1619–1623.
7. Esposito M, Capriotti E, Giunta A, et al. Long-lasting remission of pemphigus vulgaris treated with rituximab. Acta Derm Venereol. 2006;86(1):87–89.
8. Schmidt E, Hunzelmann N, Zillikens D, et al. Rituximab in refractory autoimmune bullous diseases. Clin Exp Dermatol. 2006;31(4):503–508.
9. Maloney DG, Liles TM, Czerwinski DK, et al. Phase I clinical trial using escalating single-dose infusion of chimeric anti-CD20 monoclonal antibody (IDEC-C2B8) in patients with recurrent B-cell lymphoma. Blood. 1994;84(8):2457–2466.
10. Solal-Céligny P. Safety of rituximab maintenance therapy in follicular lymphomas. Leuk Res. 2006;30(Suppl 1):S16–S21.
11. Vidal L, Gafter-Gvili A, Leibovici L, et al. Rituximab maintenance for the treatment of patients with follicular lymphoma: systematic review and meta-analysis of randomized trials. J Natl Cancer Inst. 2009;101(4):248–255.
12. Marcus R. Use of rituximab in patients with follicular lymphoma. Clin Oncol (R Coll Radiol). 2007;19(1):38–49.
13. Gürcan HM, Keskin DB, Stern JN, et al. A review of the current use of rituximab in autoimmune diseases. Int Immunopharmacol. 2009;9(1):10–25.
14. Higashida J, Wun T, Schmidt S, et al. Safety and efficacy of rituximab in patients with rheumatoid arthritis refractory to disease modifying antirheumatic drugs and anti-tumor necrosis factor-alpha treatment. J Rheumatol. 2005;32 (11):2109–2115.
15. Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med. 2004;350(25): 2572–2581.
16. Edwards JC, Cambridge G. Sustained improvement in rheumatoid arthritis following a protocol designed to deplete