A Multicenter, Randomized, Investigator-blind, Controlled Study of Short-term Healing
David Pariser, MD, Department of Dermatology, Eastern Virginia Medical School and Virginia Clinical Research, Inc., Norfolk, Virginia; James Spencer, MD; Department of Dermatology, Mt. Sinai School of Medicine, New York, New York; Brian Berman, MD, PhD; Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, Florida; Suzanne Bruce, MD; Private Practice, Houston, Texas; Lisa Parr, PharmD, RAC; Obagi Medical Products, Inc., Long Beach, California; Kenneth Gross, MD, Skin Surgery Medical Group, Inc., San Diego, California, and Division of Dermatology, University of California San Diego, San Diego, California.
This study was supported by OMP, Inc. Dr. Pariser received a grant from Obagi Medical Products, Inc., to perform this study. Dr. Spencer also received a research grant from Obagi Medical Products, Inc. Dr. Berman has a University of Miami consulting agreement with Obagi Medical Products, Inc. Dr. Bruce has received honoraria from Obagi Medical Products, Inc. Dr. Parr is an employee of and owns stock in Obagi Medical Products, Inc. Dr. Gross has a clinical research facility within his private practice and was paid to do the research for this study.
Abstract
Objective: To evaluate the efficacy and tolerability of using a 4% hydroquinone/0.05% tretinoin skin care system compared with standard treatment of cleanser plus healing ointment to enhance aesthetic outcomes resulting from electrodesiccation and curettage treatment for superficial truncal basal cell carcinomas. Design: Multicenter, investigator-masked, randomized, parallel-group study. Patients received either the hydroquinone/tretinoin system or the standard treatment twice daily for three weeks before and after electrodesiccation and curettage (post-electrodesiccation and curettage, lesions received standard treatment until reepithelialization was greater than or equal to 75 percent; assigned treatment regimens then resumed). Setting: Patients attending academic, institutional, and private dermatology clinics. Participants: 51 patients with 1 to 3 superficial truncal basal cell carcinomas. Measurements: The primary efficacy outcome was the incidence of treatment success for scar cosmesis, defined as a global assessment of excellent or good wound appearance (on a scale of excellent, good, fair, and poor), as evaluated by the investigators. After the end of the study, seven expert masked graders (dermatologists or plastic surgeons) reviewed the photographs from all of the lesions and also evaluated global assessment. Results: The incidence of treatment success in the hydroquinone/tretinoin and standard treatment groups was 72 percent versus 63 percent according to the masked investigators and 45 to 68 percent versus 20 to 44 percent, respectively, according to the seven expert masked graders. All the expert graders reported a higher incidence of treatment success with the hydroquinone/ tretinoin system than with standard treatment and this difference was statistically significant for five of the seven graders. Conclusion: The adjunctive use of the hydroquinone/tretinoin skin care system may offer enhanced aesthetic results postelectrodesiccation and curettage compared with standard treatment.
(J Clin Aesthetic Dermatol. 2009;2(5):38–43)
Electrodesiccation and curettage (EDC) is commonly used to treat superficial basal cell carcinomas (BCCs), but the resulting scars can be aesthetically unpleasing and a major disadvantage of this procedure. The use of a hydroquinone/tretinoin-based skin care system (The Obagi Nu-Derm® System, Obagi Medical Products, Inc., Long Beach, California) is known to improve overall skin quality and has been shown to significantly improve hyperpigmentation, tactile roughness, sallowness, laxity, wrinkling, and skin clarity when used for the treatment of photodamage.[1,2] Both hydroquinone and tretinoin are effective in reducing dyspigmentation,[3–8] and tretinoin has also been reported to improve scar cosmesis[9–12] and accelerate the speed of healing and/or reepithelialization after dermabrasion,[13] chemical peeling,[14] or full-thickness wounds.[15] As a result, use of the hydroquinone/tretinoin skin care system may help improve the appearance of the skin after EDC.
Here, we present the results of a study that evaluated whether using a hydroquinone/tretinoin-based skin care system before and after EDC treatment of superficial BCCs offered improved scar cosmesis.
Methods
Patients. Adults were eligible for enrollment in this multicenter, randomized, investigator-blind study if they had one, two, or three biopsy-proven superficial BCCs on the trunk, each with a diameter of >0.5cm and <2.5cm. Each lesion was required to be at least 10cm away from any other lesion.
Patients were required to use a sunscreen on the wound site each day and be willing to refrain from using any other topical products on the wound site. Women of childbearing potential were required to use a reliable method of birth control for one month before starting the study and continue use throughout the study.
Exclusion criteria included an allergy to hydroquinone, tretinoin, sunscreen, or other ingredients in the treatment regimens; a history or family history of vitiligo, or keloidal or hypertrophic scarring; uncontrolled systemic disease or insulin-dependent diabetes; immunological disorders; pregnancy, breastfeeding, or trying to become pregnant; or participation in an investigational study in the preceding 30 days. The following washout periods were required: one week for topical antibiotics; four weeks for systemic antibiotics, topical retinoids, topical and systemic steroids, alpha- and beta-hydroxy acids, polyhydroxy acids, 4-hydroxyanisole, hydroquinone, and other depigmenting products; three months for estrogen/birth control pills if their use had not been stable for the preceding three months; and one year for systemic retinoids.
The study was approved by the relevant institutional review boards and was conducted in accordance with the Declaration of Helsinki and its amendments. All patients gave signed informed consent.
Treatment regimen. Patients were randomly assigned (1:1) to receive twice-daily treatment with either a modified version of a hydroquinone 4%/tretinoin-based skin care system (the modified version of the NuDerm® system comprised cleanser [morning and evening] plus 4% hydroquinone cream [morning and evening] plus sunscreen [morning] plus 0.05% tretinoin cream [evening]; no toner or exfoliant was used) or standard treatment with a cleanser (Cetaphil® gentle skin cleanser, Galderma Laboratories, Fort Worth, Texas) plus healing ointment (Aquaphor®, Beiersdorf Inc., Wilton, Connecticut). Each regimen was used for three weeks before and after EDC, with the post-EDC therapy beginning only once a lesion had reached greater than or equal to 75 percent re-epithelialization. For at least two weeks after EDC, until such time as greater than or equal to 75 percent reepithelialization was achieved, lesions in both groups received only twice-daily applications of cleanser and healing ointment. Patients were instructed to apply sufficient amounts of the study products to fully cover each lesion plus an additional 0.5 to 1cm margin around it.
To maintain blinding, the investigators were not involved in dispensing or collecting the study products.
Outcome measures. Patients were evaluated by the investigators before and during initial treatment with the hydroquinone/tretinoin system or standard treatment, before and immediately after EDC, once greater than or equal to 75 percent reepithelialization was achieved after EDC, and at one and three weeks following the post-EDC resumption of treatment. The primary efficacy outcome was the incidence of treatment success for scar cosmesis, which was defined as a global assessment of excellent or good wound appearance (on a scale where 0=excellent, 1=good, 2=fair, and 3=poor). Distortion (i.e., wound contraction) was evaluated according to a modified version of the validated Beausang scale[16] (using a scale where 0=none, 1=mild, 2=moderate, and 3=severe). Hyperpigmentation and erythema were evaluated on a scale where 0=none, 1=mild/barely noticeable, 2=moderate/easily noticeable, and 3=severe/prominent. Lesion diameter was also assessed (prior to EDC and at three weeks after the post-EDC resumption of treatment).
After the end of the study, seven expert graders (dermatologists or plastic surgeons) reviewed the photographs from all the lesions, while masked as to treatment identity, and evaluated global assessment using the same scale as the investigators.
Statistical analysis. Between-group differences were evaluated using a chi-square test for expert grader global assessment scores; a Cochran-Mantel-Haenszel test stratified by investigator for hyperpigmentation scores; a two-way analysis of variance for changes in lesion diameter; and Fisher’s exact test for the incidence of adverse events. An a-level of 0.05 was used to determine statistical significance.
Results
Patients. A total of 51 patients (with 59 lesions) were enrolled in the study, 49 (96%) of whom completed the study. Both discontinuations were unrelated to study treatment and occurred in the group receiving standard treatment—malaise (1 patient) and voluntary withdrawal (1 patient).
The patients were a mean of 56 years old and 55 percent were male. All patients were Caucasian—Fitzpatrick skin type was I (31%), II (35%), III (27%), or IV (6%). Both groups were comparable in terms of demographic details at baseline.
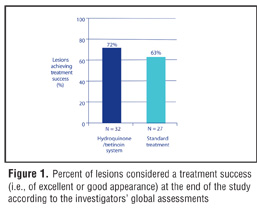
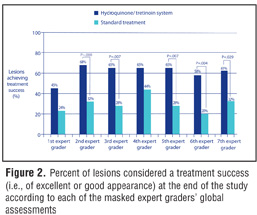
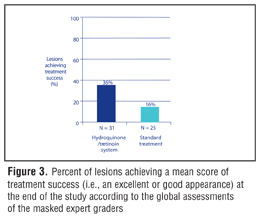
Efficacy. The investigators’ global assessments indicated that, at the end of the study, treatment success (i.e., an excellent or good wound appearance) was observed in 72 percent of lesions receiving the hydroquinone/tretinoin system compared with 63 percent of lesions receiving standard treatment (Figure 1). Results from the masked graders’ photographic review of lesions at the end of the study indicated that, depending on the individual grader, treatment success was achieved in 45 to 68 percent of lesions receiving the hydroquinone/tretinoin system compared with 20 to 44 percent of lesions receiving standard treatment (Figure 2). The results from five of the seven expert graders showed a significant between-group difference in the incidence of treatment success (with the P value ranging between 0.004 and 0.029 in these five sets of scores). Calculation of the mean expert grader score for each individual lesion revealed that 36 percent of the lesions receiving the hydroquinone/ tretinoin system were considered to have a mean score representing treatment success compared with 16 percent of lesions receiving standard treatment (Figure 3). With this overall analysis, the between-group difference was not statistically significant.
{kind=link}
{kind=link}
{kind=link}
All lesions for which photographs were available immediately post-EDC and three weeks after the post-EDC resumption of treatment are shown in Figure 4. At three weeks post-resumption of treatment, the percent of lesions that had no or mild distortion (i.e., contraction) was 100 percent with the hydroquinone/tretinoin system and 93 percent with the standard treatment. The mean lesion diameter three weeks after the post-EDC resumption of treatment was greater than before EDC in both groups. The increase was significantly larger with the hydroquinone/ tretinoin system (with which the mean diameter increased from 1.1cm to 1.8cm) than with standard treatment (with which the mean diameter increased from 1.1cm to 1.4cm) (P=0.001).
{kind=link}
Tolerability. Both treatment regimens were similarly well tolerated with no significant between-group differences in the incidence of adverse events overall or in the incidence of individual adverse events. Adverse events that were at least probably related to treatment occurred in 3/26 (12%) patients in the hydroquinone/tretinoin group (all occurring prior to EDC) and 1/25 (4%) patients in the standard treatment group (occurring post-EDC). They consisted of moderate contact dermatitis (4% with hydroquinone/ tretinoin vs. 0% with standard treatment) and mild application site conditions—itching (4% vs. 4%), erythema (4% vs. 0%), and stinging (4% vs. 0%).
At the end of the study, investigator evaluations revealed a significant between-treatment difference in the severity of hyperpigmentation in favor of the hydroquinone/tretinoin system (P=.021). Hyperpigmentation was absent or mild in 100 percent of the lesions receiving the hydroquinone/ tretinoin system and 96 percent of the lesions receiving standard treatment. In addition, erythema was absent or mild at the end of the study in 28 percent of lesions receiving the hydroquinone/tretinoin system and 22 percent of lesions receiving standard treatment.
Discussion
The results of this study suggest that the adjunctive use of the hydroquinone/tretinoin system before and after EDC can improve the appearance of the skin postprocedure. All of the expert graders reported a higher incidence of treatment success (the primary efficacy endpoint) with the hydroquinone/tretinoin system than with standard treatment; a statistically significant difference for five of the seven graders. This finding is in agreement with the relatively higher incidence of treatment success with the hydroquinone/tretinoin system also reported by the study investigators. There was some variability in the scores reported by the different expert graders even though they each reviewed an identical set of photographs. This is likely to be at least partly attributable to differences in clinical judgment and perhaps to difficulties in making an accurate assessment from a two-dimensional image. The provision of standardized photographic guides depicting each grade on the global assessment scale, together with pre-evaluation training of the graders, might be considered in future studies as one approach to potentially improve between-grader scoring consistency.
With both regimens, the incidences of treatment success reported by the investigators, and by the individual expert graders, were higher than those calculated in the overall analysis of expert grader results on an individual lesion basis. This is because the overall analysis effectively sets a higher threshold for treatment success than the other evaluations. Thus, in the investigator evaluations and the individual expert grader evaluations, a lesion is considered to have achieved treatment success as the result of a single evaluator’s assessment. In contrast, in the overall analysis, each individual lesion is considered to have achieved treatment success only if the mean scores from all the expert graders were excellent or good. The overall analysis therefore offers an alternative means of analyzing the results, which takes into account the variability in scoring between the expert graders. Regardless of whether the results are evaluated in terms of the investigator assessments, the individual expert grader assessments, or the overall analysis of expert grader assessments, the incidence of treatment success was consistently higher with the hydroquinone/tretinoin system than with standard treatment—the differential being up to 38 percent with the individual expert graders and nine percent with the investigators.
The appearance of the lesions at the end of the study varied greatly between different lesions. While some of this is likely due to inevitable inter-individual differences, some of the variation might also have been attributable to differences in surgical technique between the study sites. In the lesions that showed the best healing, the end-of-study photographs showed almost normal-looking skin with the “scar” being barely perceptible. These lesions tended to be in the hydroquinone/tretinoin group. In addition, only in the group treated with the hydroquinone/tretinoin system was distortion (contraction) either “none” or “mild” at the end of the study for every lesion. Distortion results from a puckering of the skin around the edge of the wound—as if a purse string is being tightened around it—and may result in a less-than-perfect aesthetic outcome. Furthermore, after the study, some of the expert graders commented that the wound edges were generally more elevated with the standard treatment than with the hydroquinone/tretinoin system. Wound elevation is generally believed to contribute to poor cosmetic outcomes of scars as well as hypertrophic scarring. To evaluate this further, it may be beneficial in future research to include an assessment of wound-edge elevation. In addition, longer-term evaluations might be considered to evaluate how the improvements in scar cosmesis observed in this study progress over the ensuing weeks and months.
Possibly the most clinically important findings in this study are the lower tendency to distortion, hyper-pigmentation, and erythema with the hydroquinone/ tretinoin treatment—distortion was absent or no more than mild in 100 percent of the lesions treated with the hydroquinone/tretinoin system (and greater than this in 7% of the lesions receiving control treatment), hyper-pigmentation was absent or mild at the end of the study in 100 percent of the lesions treated with the hydroquinone/ tretinoin system (and greater than this in 4% of the lesions receiving standard treatment), and erythema was absent or mild at the end of the study in 28 percent of lesions receiving the hydroquinone/tretinoin system (compared with 22% of lesions receiving standard treatment). This lower tendency toward distortion, hyperpigmentation, and erythema in the hydroquinone/tretinoin group could help promote more favorable wound cosmesis.
The major limitation of EDC is commonly held to be wound cosmesis. Therefore, any treatment that can help mitigate this problem could be of great value clinically. (Similarly, any treatment that is effective in improving post-EDC wound cosmesis might also have clinical utility in improving the appearance of lesser wounds from other treatment modalities—so any approach that helps avoid scar formation post-EDC could have wider applications beyond EDC.) A variety of different modalities have been tried in an attempt to prevent or treat various types of scars—including vitamins A and E, interferon, imiquimod 5% cream, tacrolimus, botulinum toxin, 5-fluorouracil, bleomycin, verapamil, silicone elastomer sheeting, surgical excision, intralesional corticosteroid injections, pressure therapy, radiation, laser treatment, polyurethane dressing, onion extract, and cryotherapy.[17,18] Topical therapies, in particular, have become increasingly popular because of their ease of use, comfort, noninvasiveness, and relatively low cost.[19] However, the effectiveness of some of these options has been called into question and optimal management strategies for others are yet to be defined. Nevertheless, there is ample evidence available to support the scientific rationale of using tretinoin and hydroquinone to ameliorate hyperpigmentation.[20–23] In photodamaged skin, tretinoin has also shown benefit in improving other aspects of the skin’s appearance including wrinkling and yellowing/sallowness.20,21 Tretinoin is thought to enhance the depigmenting effect of hydroquinone24,25 and the combined use of hydroquinone and tretinoin is an established treatment for hyperpigmentation.[26,27]
A rational way to incorporate the hydroquinone/ tretinoin treatment into clinical practice would be to include its use in the wound care instructions given to patients after the biopsy of any suspicious lesion. If the biopsy result indicates a BCC, patients would continue using the hydroquinone/tretinoin system until the post-biopsy follow-up appointment. If they subsequently undergo EDC, instructions to resume use of the hydroquinone/tretinoin system at least two weeks post-EDC could be incorporated into the post-EDC wound care instructions. If the original biopsy indicates the lesion is benign, the patient may discontinue the hydroquinone/ tretinoin treatment. A potential benefit of the treatment they received, or could elect to continue to receive, is the possibility of improved cosmesis of their biopsy scar.
Conclusion
Use of the hydroquinone/tretinoin skin care system adjunctively with EDC may offer enhanced aesthetic results postprocedure compared with standard treatment. It is likely that tretinoin and hydroquinone both play a role in this—as tretinoin enhances wound healing and reduces dyspigmentation, and hydroquinone evens skin coloration and minimizes dyspigmentation.
Both regimens were well tolerated and further research is now warranted to extend our understanding of the potential benefits of the hydroquinone/tretinoin system not only when used in conjunction with EDC but also when used with other procedures (including incisional surgery) and in other disease states.
References
1. Herndon JH, Stephens TJ, Sigler ML. Efficacy of a tretinoin/hydroquinone-based skin health system in the treatment of facial photodamage. Cos Derm. 2006;19:255–262.
2. Comstock J. Using a 4% hydroquinone/tretinoin-based skin care system in conjunction with facial rejuvenation procedures. Poster 2807 presented at the 66th Annual Meeting of the American Academy of Dermatology, February 1–5, 2008, San Antonio, TX. OMP, Inc. http://www.obagi.com/documents/C%20%20E%20Poster%20FINAL.pdf. Accessed January 14, 2009.
3. Haddad AL, Matos LF, Brunstein F, et al. A clinical, prospective, randomized, double-blind trial comparing skin whitening complex with hydroquinone vs. placebo in the treatment of melasma. Int J Dermatol. 2003;42:153–156.
4. Lowe N, Horwitz S, Tanghetti E, et al. Tazarotene versus tazarotene plus hydroquinone in the treatment of photodamaged facial skin: a multicenter, double-blind, randomized study. J Cosmet Laser Ther. 2006;8:121–127.
5. Kakita LS, Lowe NJ. Azelaic acid and glycolic acid combination therapy for facial hyperpigmentation in darker-skinned patients: a clinical comparison with hydroquinone. Clin Ther. 1998;20:960–970.
6. Halder RM, Richards GM. Topical agents used in the management of hyperpigmentation. Skin Therapy Lett. 2004;9:1–3.
7. Pagnoni A, Kligman AM, Sadiq I, Stoudemayer T. Hypopigmented macules of photodamaged skin and their treatment with topical tretinoin. Acta Derm Venereol. 1999;79:305–310.
8. Kang S, Bergfeld W, Gottlieb AB, et al. Long-term efficacy and safety of tretinoin emollient cream 0.05% in the treatment of photodamaged facial skin: a two-year, randomized, placebo-controlled trial. Am J Clin Dermatol. 2005;6:245–253.
9. Janssen de Limpens AM. The local treatment of hypertrophic scars and keloids with topical retinoic acid. Br J Dermatol. 1980;103:319–323.
10. Panabiere-Castaings MH. Retinoic acid in the treatment of keloids. J Dermatol Surg Oncol. 1988;14:1275–1276.
11. Schmidt JB, Binder M, Macheiner W, Bieglmayer C. New treatment of atrophic acne scars by iontophoresis with estriol and tretinoin. Int J Dermatol. 1995;34:53–57.
12. Knor T. Flattening of atrophic acne scars by using tretinoin by iontophoresis. Acta Dermatovenerol Croat. 2004;12:84–91.
13. Mandy SH. Tretinoin in the preoperative and postoperative management of dermabrasion. J Am Acad Dermatol. 1986;15:878–879.
14. Hevia O, Nemeth AJ, Taylor JR. Tretinoin accelerates healing after trichloroacetic acid chemical peel. Arch Dermatol. 1991;127:678–682.
15. Popp C, Kligman AM, Stoudemayer TJ. Pretreatment of photoaged forearm skin with topical tretinoin accelerates healing of full-thickness wounds. Br J Dermatol. 1995;132:46–53.
16. Beausang E, Floyd H, Dunn KW, et al. New quantitative scale for clinical scar assessment. Plast Reconstr Surg. 1998;1026:1954–1961.
17. Berman B, Villa AM, Ramirez CC. Novel opportunities in the treatment and prevention of scarring. J Cutan Med Surg. 2004;8 Suppl 3:32–36.
18. Berman B, Perez OA, Konda S, et al. A review of the biologic effects, clinical efficacy, and safety of silicone elastomer sheeting for hypertrophic and keloid scar treatment and management. Dermatol Surg. 2007;33:1291–1302.
19. Zurada JM, Kriegel D, Davis IC. Topical treatments for hypertrophic scars. J Am Acad Dermatol. 2006;55:1024–1031.
20. Kang S, Bergfeld W, Gottlieb AB, et al. Long-term efficacy and safety of tretinoin emollient cream 0.05% in the treatment of photodamaged facial skin: a two-year, randomized, placebo-controlled trial. Am J Clin Dermatol. 2005;6:245–253.
21. Weiss JS, Shavin JS, Nighland M, Grossman R. Tretinoin microsphere gel 0.1% for photodamaged facial skin: a placebo-controlled trial. Cutis. 2006;78:426–432.
22. Haddad AL, Matos LF, Brunstein F, et al. A clinical, prospective, randomized, double-blind trial comparing skin whitening complex with hydroquinone vs. placebo in the treatment of melasma. Int J Dermatol. 2003;42:153–156.
23. Grimes PE. Melasma. Etiologic and therapeutic considerations. Arch Dermatol. 1995;131:1453–1457.
24. Engasser PG, Maibach HI. Cosmetic and dermatology: bleaching creams. J Am Acad Dermatol. 1981;5:143–147.
25. Kasraee B, Handjani F, Aslani FS. Enhancement of the depigmenting effect of hydroquinone and 4-hydroxyanisole by all-trans-retinoic acid (tretinoin): the impairment of glutathione-dependent cytoprotection? Dermatology. 2003;206:289–291.
26. Pérez-Bernal A, Muñoz-Pérez MA, Camacho F. Management of facial hyperpigmentation. Am J Clin Dermatol. 2000;1:261–268.
27. Pathak MA, Fitzpatrick TB, Kraus EW. Usefulness of retinoic acid in the treatment of melasma. J Am Acad Dermatol. 1986;15:894–899.
Ackowledgments
We gratefully acknowledge the participation of the late Robert Loss, MD, as an investigator in this study. We also thank the masked expert graders who evaluated the photographs: Maria Alora-Palli, MD, Harvard Medical School, Boston, Massachusetts; R. Sonia Batra, MD, Department of Dermatology, USC Keck School of Medicine, Los Angeles, California; Barry DiBernardo, MD, FACS, University of Medicine and Dentistry of New Jersey, Newark, and New Jersey Plastic Surgery, Montclair, New Jersey; David Pariser, MD, Eastern Virginia Medical School, Norfolk, Virginia; Alexa Boer Kimball, MD, MPH, Clinical Unit for Research Trials in Skin (CURTIS), Massachusetts General and Brigham and Women’s Hospitals, Harvard Medical School, Boston, Massachusetts; James Leyden, MD, University of Pennsylvania, Philadelphia, Pennsylvania; and Michael B. Stevens, MD, PhD, FACS, Obagi Dermatology, Plastic Surgery, and Laser Center, Beverly Hills, California.