 J Clin Aesthet Dermatol. 2024;17(2):20-22.
J Clin Aesthet Dermatol. 2024;17(2):20-22.
by Yun Seok Yang, MD; Duk Han Kim, MD; Ji Hyun Ha, MD; Na Young Ko, MD; Joong Keun Kim, MD; Woo Jin Choi, MD;
Byong Han Song, MD; Sang Hyeon Hwang, MD; Ki Min Sohn, MD; and Hye-Jin Ahn, MD
Drs. Yang, Kim, Ha, Ko, Kim, Choi, Song, Hwang, and Sohn are with the Renewme Dermatologic Clinic in Seoul, South Korea. Dr. Ahn is with the Department of Dermatology at Kyung Hee University College of Medicine and Kyung Hee University Hospital in Seoul, Korea.
FUNDING: This research was supported by CLASSYS.Inc in the Republic of Korea.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
ABSTRACT: Monopolar radiofrequency (RF) non-invasively tightens and rejuvenates the skin by stimulating collagen fiber production. Since the introduction of the monopolar RF device in the early 2000’s, RF devices have advanced and they can rejuvenate of periorbital and forehead wrinkles, as well as skin laxity of the lower face and neck. We compared the differences in the treatment effects based on the tip size. This randomized split-face study comprised 31 participants aged 29 to 75 years old (three males and 28 females) who underwent one session of monopolar RF; one side of the face was treated with a 3cm2 tip and the other with a 4cm2 tip. Facial wrinkle scores were measured on the upper face and the lower face before and after treatment for up to three months. Significant improvement was observed in the periorbital area (p<0.001), forehead (p=0.72), and glabellar (p=0.63) treated with a smaller tip. However, nasolabial folds (p=0.8) and marionette lines (p=0.13) showed better improvement when treated with a larger tip.
Keywords: face, monopolar radiofrequency, rejuvenation, wrinkle
Aging is an inevitable process characterized by wrinkles and fine lines on the face, thereby affecting its appearance. Various rejuvenation treatments have been developed to reverse the signs of aging. One such treatment is the monopolar radiofrequency (RF) technology, which tightens and rejuvenates the skin. RF treatment results in conformational changes in the collagen network and stimulation of collagen production de novo induced by elevated temperatures.1 Reportedly, monopolar RF improves the facial skin structure; however, the results vary in different facial areas and subareas in the same individual.2 This study aimed to perform a split-face comparison evaluating RF efficacy using a 3cm2 tip versus a 4cm2 tip on different facial areas.
Methods
This randomized split-face trial comprised 31 participants (three males and 28 females) with Fitzpatrick Skin Types III and IV, aged 29 to 75 years old (mean age 52.45 years). They were included when both wrinkles were symmetrical grade. Informed consent was obtained from all participants. The treatment was performed under local anesthesia (topical application of 5-MC cream, Lidocaine 96mg/g; The-U Pharmaceutical Co., Ltd., South Korea; 30 min before treatment). After the application of the conductive fluid, each participant underwent a single session of monopolar RF (Volnewmer, Classys, South Korea). The newly developed monopolar RF device in this study was equipped with two handpieces; therefore, the clinician could apply the 3cm2 and 4cm2 tips without changing the tip. One side of the face was treated with a 3cm2 tip, and the other with a 4cm2 tip, 300 shots each. It was treated with 2.5~3 level energy, depending on the individual. The total delivered energy was 16-19kJ/cm2, and the average delivered energy for the 3cm2 tip and the 4cm2 tip was 16.4J/cm2 and 16.6J/cm2, respectively. Before and 1 and 3 months after clinical photographs were taken using a facial skin analyzer (MarkVu, PSI plus, South Korea) to compare the wrinkle scores in different facial areas. Two dermatologists blindly measured the mean facial wrinkle scores3 on the upper face, including the periorbital and forehead lines, and the glabella, and the lower face, including the nasolabial folds and marionette lines (Table 1). The participants’ comfort level on a 5- point scale (0, no pain; 1, mild pain; 2, moderate pain; 3, severe pain; 4, intolerable pain) and participants satisfaction assessment on a 4-point scale (1, worse; 2, <25% mild improvement; 3, 25-49% improvement; 4: >50% major improvement) was assessed.
A linear mixed model was used to compare the changes in the wrinkle scores before and after treatment according to the tip size. Statistical significance was set at p<0.05. Data were analyzed using the IBM SPSS software (version 27.0; IBM Corp., Armonk, NY, USA).
Results
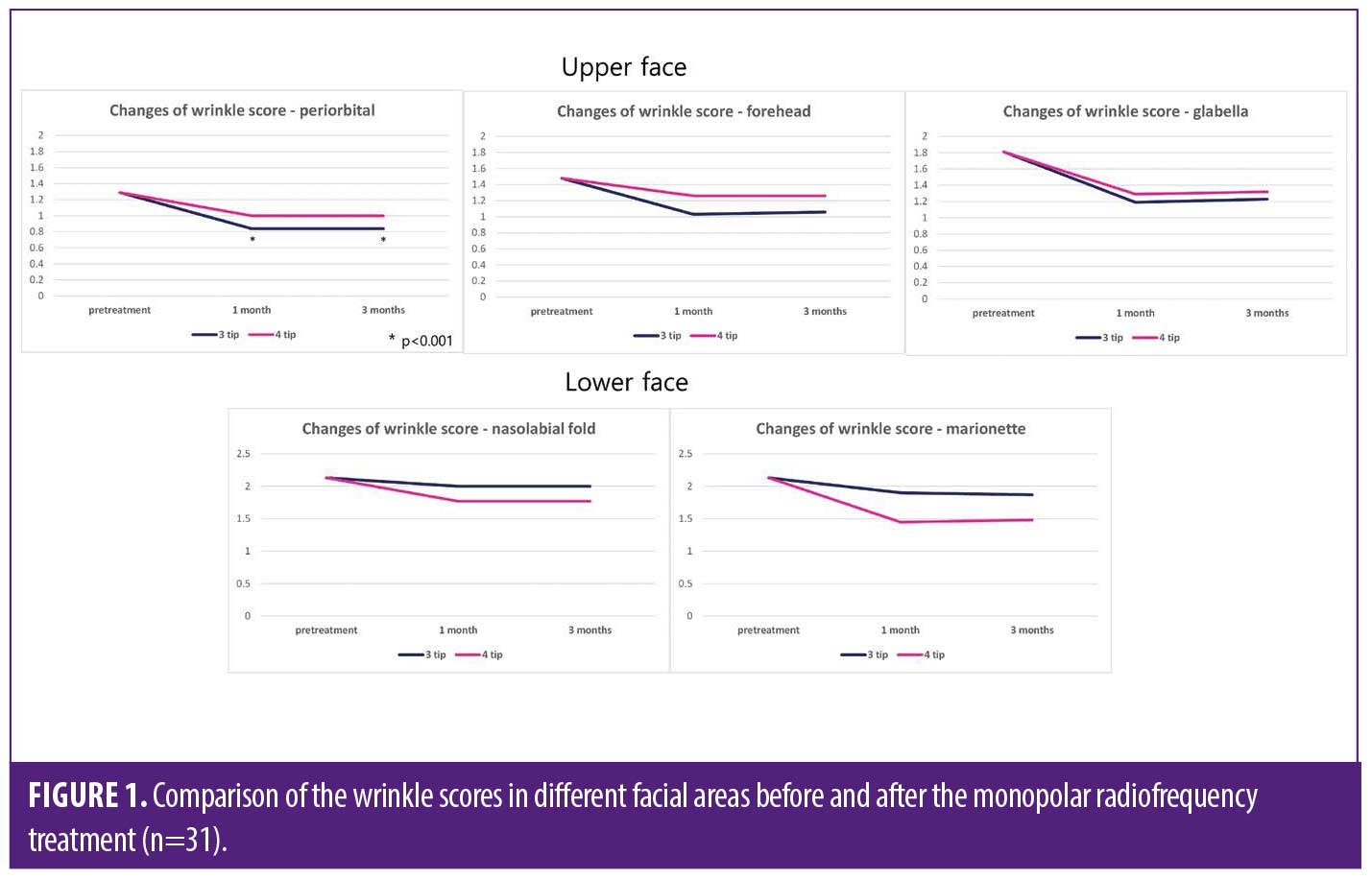
In the upper face, the periorbital area treated with the 3cm2 tip showed significant improvement (Figure 1). In the upper face wrinkles, including the forehead, glabella, and periorbital line, wrinkle scores were 1.48, 1.81, and 1.29 in pretreatment, respectively. The wrinkle score of forehead after treatment were 1.06 with the 3cm2 tip and 1.26 with the 4cm2 tip at three months, the wrinkle score of glabella were 1.23 with the 3cm2 tip and 1.32 with the 4cm2 tip at three months, and the wrinkle score of periorbital line were 0.84 with the 3cm2 tip and 1 with the 4cm2 tip at three months (Table 2). The upper face wrinkle treated with the 3cm2 tip showed better improvement than the area treated with the 4cm2 tip, although the difference was not significant between two tips (p=0.845). However, on the lower face, the nasolabial folds and marionette lines treated with the 4cm2 tip showed better improvement than the area treated with the 3cm2 tip (Figures 1 and 2). In the lower face wrinkles, including the nasolabial folds and marionette line, wrinkle scores were 2.13 and 2.13 in pretreatment, respectively. The wrinkle score of nasolabial folds after treatment were 2 with the 3cm2 tip and 1.77 with the 4cm2 tip at three months and the wrinkle score of marionette line were 1.87 with the 3cm2 tip and 1.48 with the 4cm2 tip at three months (Table 2). The improvements after one month were usually well maintained for up to three months in the clinical photographs.
The mean comfort level score was 0.61. Seventeen participants (54.8%) reported no pain, nine (29%) reported mild pain, and five (16.1%) reported moderate pain. No participants reported severe or intolerable pain. The mean participants satisfaction assessment one month after treatment was 2.42, thirteen participants (41.9%) reported 25 to 49 percent improvement, and eighteen (58.1%) reported less than 25 percent mild improvement. After three months of treatment, the average satisfaction score slightly decreased to 2.32, and 10 patients (32.3%) maintained a 25 to 49 percent improvement in satisfaction. No serious side effects were reported, except for one participant who was treated with the 4cm2 tip and had a mild erythematous burn on the forehead, which healed spontaneously within a week.

Discussion
The findings of this study suggest that the efficacy of monopolar RF treatment varies depending on the tip size and facial area. As RF energy is produced by an electric current rather than a light source, it is not subject to diminution by tissue scattering or absorption by epidermal melanin, and significant thermal energies can be generated safely within the deeper tissue layers causing collagen contraction and new collagen formation.4 The effect of monopolar RF on laxity mainly occurs as a result of uniform volumetric heating of the dermis.4 A previous study reported that dermal thickness and subcutaneous fat influence RF current distribution and interarea variations in the clinical results.2 Dermal thickness is thicker in the order of eyelids, followed by the forehead, glabella, and submandibular areas, with differences observed among individuals.5,6 Generally, the dermal thickness of the upper face is relatively thinner than the lower face. Thus, for increased efficacy, a monopolar RF device should be able to deliver volumetric heating to an optimal depth. The optimal depth might differ based on the patient’s age and facial area. Small monopolar RF tip targeting the thinnest area around the eyes are currently in use, and a 0.25cm2 monopolar RF tip has been reported to be safe and effective for skin tightening on the upper and lower eyelids.7
The larger the monopolar RF tip size, the more energy can be delivered to the deeper layers.8 RF energy penetration depth is about one third of electrode radius and treatment effects with monopolar devices depend on RF power and size of electrode.9 Heat distribution which is strong at the surface of the active electrode and is reduced dramatically at a distance exceeding the size of electrode, thereby limiting penetration depth.9
In our study, the upper face demonstrated better improvement for the 3cm2 tip than the 4cm2 tip, particularly in the periorbital area, which is the thin skin area (Figure 2). However, in the lower face, better results were observed in areas treated with the 4cm2 tip. The results suggested that the larger tip size could affect deeper dermis than the smaller tip size. In addition, the larger the tip size, the larger the overlapping area, which can enlarge thermal zone effect.
No serious side effects or complaints of severe pain were reported. The improved safety and decreased pain reported in this study were because of the continuous water-cooling system of this new monopolar RF technology, which constantly kept the skin surface temperature at 12–14°C. In the 1-month follow-up, most participants reported mild to moderate improvement, and the satisfaction was well maintained for three months. However, unlike the existing literature reporting that collagen formation continues even after 3 to 6 months,10,11 no further clinical improvement was observed at the 3-month follow-up. A long-term follow-up comparison after the repetition of several treatment sessions is required in future studies. The limitations of this study included small number of participants and wide range of age discrepancy, and a short follow-up period of three months.
In conclusion, our results found a smaller tip size (3cm2) is better for upper facial wrinkles, and a larger tip size (4cm2) is better for lower facial laxity. The new monopolar RF device with a continuous water-cooling system is less painful, safer, and effective for whole-face rejuvenation.
References
- N. Sadick. Tissue tightening technologies: fact or fiction. Aesthetic Surgery Journal. 2008; 28(2):180–188.
- Kruglikov IL. Influence of the Dermis Thickness on the Results of the Skin Treatment with Monopolar and Bipolar Radiofrequency Currents. Biomed Res Int. 2016;2016:1953203.
- Lemperle G, Holmes RE, Cohen SR, Lemperle SM. A classification of facial wrinkles. Plast Reconstr Surg. 2001;108(6):1735–1750.
- Alster TS, Lupton JR. Nonablative cutaneous remodeling using radiofrequency devices. Clin Dermatol. 2007;25(5):487–491.
- Ha RY, Nojima K, Adams WP Jr, Brown SA. Analysis of facial skin thickness: defining the relative thickness index. Plast Reconstr Surg. 2005;115(6):1769–1773
- Meng Y, Feng L, Shan J, et al. Application of high-frequency ultrasound to assess facial skin thickness in association with gender, age, and BMI in healthy adults. BMC Med Imaging. 2022;22(1):113.
- Carruthers J, Carruthers A.Shrinking upper and lower eyelid skin with a novel radiofrequency tip. Dermatol Surg. 2007 Jul;33(7):802–809.
- Suh DH, Ahn HJ, Seo JK, et al. Monopolar radiofrequency treatment for facial laxity: Histometric analysis. J Cosmet Dermatol. 2020 Sep;19(9):2317–2324.
- Michael K, Stephen M. Enhanced Liposuction. Chapter. The Basic Science of Radiofrequency-Based Devices. London: Intechopen. 2022.
- Lolis MS and Goldberg DJ. Radiofrequency in cosmetic dermatology: a review. Dermatol Surg. 2012;38(11):1765–1776.
- Alster TS, Lupton JR. Nonablative cutaneous remodeling using radiofrequency devices. Clin Dermatol. 2007;25(5):487–491.