J Clin Aesthet Dermatol. 2025;18(12):73–75.
by Iman Ali, MD; Roger Ceilley, MD; and Ciaran Smythe, DO
Dr. Ali is with the Department of Internal Medicine at Texas Health Presbyterian Dallas in Dallas, Texas, and the McGovern Medical School at the University of Texas Health Science Center at Houston in Houston, Texas. Dr. Ceilley is with Dermatology P.C. in West Des Moines, Iowa. Dr. Smythe is with the Department of Dermatology at Lake Granbury Medical Center in Dallas, Texas.
FUNDING: No funding was provided for this article.
DISCLOSURES: Dr. Smythe is the founder and owner of Solas Medical LLC. The remaining authors have no conflicts of interest relevant to the contents of this article.
ABSTRACT: Background: Fractional carbon dioxide (CO2) laser resurfacing is an effective treatment of various dermatological conditions. Pain, erythema, and edema following fractional ablative resurfacing are key limitations to patient comfort and satisfaction. Objective: This study aims to describe a novel technique using laser-assisted drug delivery to administer a combination of local anesthetics and epinephrine both during and after fractional CO2 laser resurfacing, enhancing procedural anesthesia and postprocedure recovery. Methods: We performed an observational review of patient-reported pain scores and clinical outcomes in patients treated with application of an anesthetic spray during and after fractional CO2 laser resurfacing treatments. Results: Patients demonstrated an average of 68% reduction in pain scores (p<0.001) scores postapplication, with additional clinical improvements in postlaser erythema and edema. Conclusion: Laser-assisted drug delivery of local anesthetics and epinephrine after fractional ablative resurfacing appears to offer a simple, low-cost adjunct for improving patient experience and recovery. Further investigation is warranted. Keywords: Fractional CO2 laser resurfacing, laser-assisted drug delivery, anesthetic, lidocaine, bupivacaine, epinephrine
Introduction
Fractional carbon dioxide (CO2) laser resurfacing is an effective treatment for various dermatological conditions such as photoaging, wrinkles, acne scarring, and abnormal pigmentation. By creating microscopic zones of thermal injury within the skin, it stimulates collagen production and remodeling, leading to significant improvements in skin texture, tone, and overall appearance.1 Compared to traditional full-field lasers, fractional CO2 systems offer the advantage of shorter recovery times and a reduced risk of complications due to the preservation of untreated skin between ablated zones.1
However, this procedure does present with challenges. Pain during and after treatment remains a significant concern, often requiring the use of topical or local anesthetics. In addition, patients frequently experience postprocedural erythema and edema, which can vary in duration and severity depending on individual skin sensitivity, the location treated, and intensity of procedure.1
Various anesthesia methods are used in dermatologic laser procedures to optimize patient comfort and procedural tolerance. Topical anesthetics, such as lidocaine and benzocaine, are commonly used for superficial treatments and offer noninvasive pain reduction.2 For procedures involving deeper tissue penetration or more extensive areas, regional nerve blocks, specifically infraorbital, mental, and supraorbital, provide targeted and effective analgesia.2 In some cases, systemic medications may be administered to manage anxiety and discomfort. These include oral anxiolytics such as lorazepam, inhaled agents such as nitrous oxide, and, in rare instances, general anesthesia for complex or highly sensitive treatments.3 Determining the anesthetic approach depends on the area of skin being treated, laser parameters, and individual patient factors.
Laser-assisted drug delivery (LADD) is an emerging technique that uses microthermal injury created by fractional lasers to enhance the transcutaneous absorption of topically applied agents. By disrupting the stratum corneum (and, depending on the depth of penetration, reaching the dermal-epidermal junction), fractional lasers temporarily increase skin permeability, allowing more efficient delivery of therapeutic compounds.4 While LADD has been extensively studied for the administration of agents such as corticosteroids and 5-fluorouracil, its application in postprocedural analgesia remains underexplored.5,6 This approach presents a promising opportunity to deliver local anesthetics directly into sensitized tissue following laser resurfacing, potentially improving patient comfort and accelerating recovery.
The objective of this research study is to describe a drug delivery method applied during and after fractional CO2 laser resurfacing that can improve patient pain management and promote faster visible recovery.
Methods
Patients who received full-face resurfacing treatment with the Solas 10600 FX fractional CO2 laser (Solas Medical LLC) were selected and provided consent for this study. All procedures were performed by a dermatology resident physician.
Patients received a standard pretreatment 7% lidocaine and 23% tetracaine topical anesthetic mixture applied to the full face prior to the laser treatment. Immediately after the procedure, 2 to 3mL of a topical anesthetic spray composed of a 1:1 mixture of lidocaine 1% with epinephrine (1:100,000) and bupivacaine 0.5% was applied to the full treated area to reduce postprocedural pain and minimize erythema and edema.
Patient-reported pain scores were recorded using a numeric rating scale (1-10) immediately after completion of full-face fractional CO2 laser resurfacing and again 10 minutes after application of the analgesic. A score of 1 represented no pain and 10 indicated severe pain. Clinical observations of immediate post-procedural erythema and edema were recorded and compared to historical expectations for fractional CO2 laser treatments.
Results
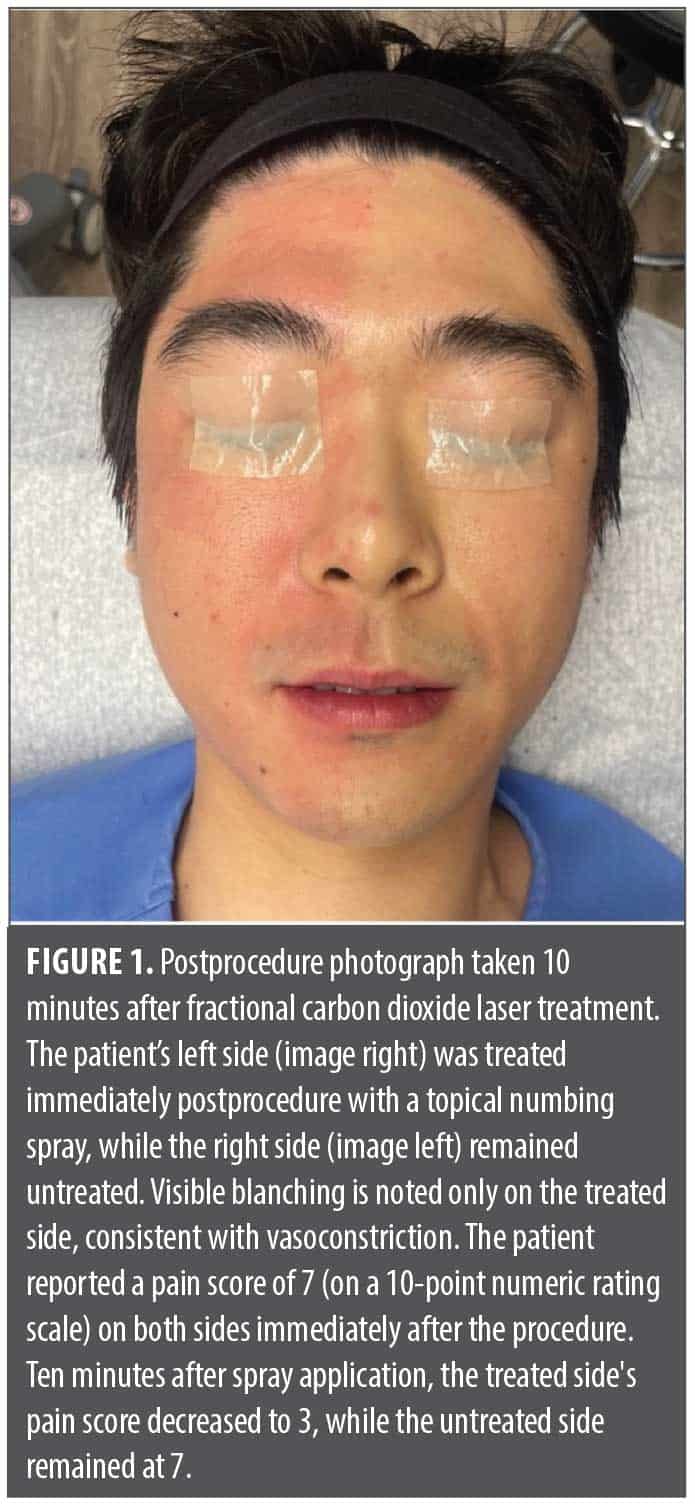
A preliminary observational series was conducted with patients (n=8), aged 28 to 57 years, who underwent fractional CO2 laser resurfacing. On average, pain scores were reduced by 68% within 10 minutes of numbing spray application (p<0.001, paired t test). Decreased clinical erythema and edema were observed compared to the expected post-CO2 laser appearance, as demonstrated in the patient, who provided photoconsent, in Figure 1. Additionally, patients who received the intraprocedural anesthetic spray reported greater comfort during subsequent deeper laser passes. Table 1 highlights pain responses before and after the numbing spray.
Discussion
The results of this study support the potential of LADD as an effective strategy to reduce post-procedural pain following fractional CO2 laser resurfacing. The enhanced permeability of the skin created by laser-induced microchannels facilitates deeper, more efficient penetration of topically applied anesthetics. This approach uses the rapid onset of lidocaine for immediate pain relief, while the addition of bupivacaine, known for its longer duration of action, prolongs analgesia and improves postprocedural comfort. Although lidocaine is primarily used for its speed of onset, it also exhibits mild vasodilatory effects, which can theoretically enhance systemic absorption and anesthetic efficacy in the absence of vasoconstrictors.7 To counteract this, epinephrine is frequently added for its vasoconstrictive properties, which reduces local blood flow. This limits systemic absorption, prolongs anesthetic duration, and helps mitigate common post-treatment symptoms such as erythema and edema. The addition of bupivacaine, with its slower onset but prolonged effect, complements the immediate relief from lidocaine, providing a broader window of analgesia.8 Together, these mechanisms provide a targeted, synergistic approach to improving patient comfort and accelerating visible recovery following fractional resurfacing procedures.
This approach could greatly improve overall patient experience. Enhanced anesthetic delivery improves patient comfort by reducing postprocedure pain and potentially minimizing treatment-related anxiety. Additionally, the vasoconstrictive effect of epinephrine helps minimize postprocedure erythema and edema, leading to a more favorable immediate appearance. These benefits collectively enhance patient satisfaction, not only by improving the immediate procedural experience but also by potentially shortening recovery time. As a result, patients may be more inclined to pursue future treatments, thereby supporting better long-term therapeutic outcomes.
This study has several limitations. The small sample size and absence of control groups restrict the generalizability of the findings. In particular, the lack of a control group that did not receive the anesthetic spray makes it difficult to determine whether the observed effects were attributable to the intervention itself. Two of the eight patients underwent a split-face design and showed reduced pain and erythema on the treated side only ten minutes after application (Figure 1). Lastly, because pain reporting is inherently subjective, variability in patient responses may have influenced the results.
Future research should include larger, prospective studies to strengthen the validity and generalizability of the findings. Additionally, investigating the use of this delivery method for other topical agents, such as anti-inflammatory medications or scar-prevention compounds, may help expand its therapeutic potential.
Conclusion
Laser-assisted delivery of an anesthetic-vasoconstrictor combination spray, administered immediately following fractional CO2 laser resurfacing and optionally between sequential laser passes, appears to improve procedural tolerance and postprocedural tolerance. This technique is simple, cost-effective, and easily integrated into existing practice workflows. More providers and larger patient cohorts are needed to confirm efficacy and safety, and studies with other devices and topical medications may expand this technique to additional procedures and energy-based systems.
References
- Yumeen S, Khan T. Laser carbon dioxide resurfacing. In: StatPeals. StatPearls Publishing; 2025-. Updated April 23, 2023. https://www.ncbi.nlm.nih.gov/books/NBK560544/
- Gaitan S, Markus R. Anesthesia methods in laser resurfacing. Semin Plast Surg. 2012;26(3):117-124.
- Vejjabhinanta V, Martins A, Huo R, Nouri K. Anesthesia for laser surgery. In: Nouri K, ed. In Lasers in Dermatology and Medicine. 2011;329-335.
- Sklar LR, Burnett CT, Waibel JS, Moy RL, Ozog DM. Laser assisted drug delivery: a review of an evolving technology. Lasers Surg Med. 2014;46(4):249-262.
- Alegre-Sánchez A, Jiménez-Gómez N, Boixeda P. Laser-assisted drug delivery. Actas Dermosifiliogr (Engl Ed). 2018;109(10), 858-867.
- Waibel JS, Wulkan AJ, Shumaker PR. Treatment of hypertrophic scars using laser and laser assisted corticosteroid delivery. Lasers Surg Med. 2013;45(3):135-140.
- Becker DE, Reed KL. Local anesthetics: review of pharmacological considerations. Anesth Prog. 2012;59(2):90-101.
- Covino BG. Pharmacology of local anesthetic agents. Br J Anaesth. 1986;58(7):701-716.