 J Clin Aesthet Dermatol. 2021;14(1):E61–E63.
J Clin Aesthet Dermatol. 2021;14(1):E61–E63.
by Lee Walker, BDS MFDS MJDF and Raul Cetto, MBBS, PhD, MRCS, DOHNS, PGDip (AestMed)
Dr. Walker is with BCity Clinics in Liverpool, England. Dr. Cetto is with Clinic One Point Six in London, England.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
ABSTRACT: Clinicians employ several techniques to augment lips with hyaluronic acid (HA) filler. To the best of our knowledge, however, no previous study has documented the use of a 4-mm 30-gauge needle in this context. This paper describes the anatomical rationale behind and practical application of such a needle applied very superficially in the vermillion border during lip augmentation. Using a 4-mm 30-gauge needle facilitates precise HA placement into the safer subcutaneous plane of the lip and lowers the pressure needed to extrude the filler, which might optimize patient comfort. This technique aims to increase the safety and predictability of lip augmentation with HA fillers. Credit is owed to Dr. Jean Louis Sebagh, who provided the inspiration to use the described needle for this evidence-based technique.
KEYWORDS: Hyaluronic acid, lip augmentation, 4-mm 30-gauge needle, safety
The lips, which are highly vascularized and dynamic, are predominately supplied by the superior and inferior labial arteries. The course and distribution of these arteries and their collaterals are highly variable. Papers describing the topography, distribution, and patterns of the lip vasculature have highlighted areas that may be more prone to complications during dermal filler injections.1–3 Arguably, therefore, the vessel depth and tissue planes are constants that clinicians can use to ensure a lower probability of a vascular accident.
Broadly, labial arteries can exist in one of three anatomical locations: submucosally on the nonkeratinized, or “wet,” side, intramuscularly between the superficial and deep layers of the orbicularis oris muscle, or subcutaneously on the keratinized, or “dry,” side.3 For simplicity, we use the mucosal-cutaneous junction (i.e., the wet/dry border) to delineate these positions.
The submucosal position is the most likely to bear the labial arteries, followed by the intramuscular and subcutaneous planes. A study of 26 cadavers (50% female) revealed that the superior and inferior labial arteries in the upper lip ran between the oral mucosa and the orbicularis oris muscle (i.e., submucosal plane) in 69.2 percent of the specimens.1 The same group also reported that, in 193 Caucasian cadavers (56.5% female), the labial vessels were submucosal in 78.1 percent, intramuscular in 17.5 percent and subcutaneous in 2.1 percent of specimens, respectively.3 A study of 25 Turkish male head cadavers located the superior labial artery ran in the submucosal position in 50 percent of specimens and intramuscular in the remaining 50 percent. Dissection revealed no subcutaneous superior labial arteries.4
Several studies have assessed the depth of the superior and inferior labial arteries to date (Table 1).5–7 Furthermore, Lee et al2 reported that the mean depths of the superior labial artery at the vermillion border ranged from 3.3 to 3.9 mm; pursuing superficial injection (<4 mm) only in the vermillion border is essential to avoid vascular injury. The average depth suggests an increased likelihood of complications when using the standard 13-mm needle that is usually prepacked with hyaluronic acid (HA) fillers. Given the rarity of serious complications with HA fillers, a prospective study is impractical and clinicians need to rely on the precautionary principle.

Based on anatomical observations, the vermilion borders of both lips are safe for the superficial injection of fillers. All areas of the lower lip are safe, reflecting the ascending arteries’ small size. Tansatit et al1 suggested placing filler into the middle of the lip to avoid injection between the muscle layer and the mucosa. Cotofana et al3 concurred that injection into the subcutaneous plane is safer for lip augmentation and better to avoid superficial arteries than that in the midline of both lips.
Our search for a safer technique for lip augmentation was not satisfied by any of the available literature. Instead, the idea of an evidenced-based approach to a safer method of lip injection was inspired by watching Dr. Jean Louis Sebagh inject his patient with a 4-mm 30-gauge needle at the International Teoxane Expert Day in Paris, France, in October 20158—a technique he has employed since at various conferences. We modified the use of this 4-mm 30-gauge needle to produce the technique described here.
A new technique
Based on anatomical information, we place filler very superficially in the vermillion border during lip augmentation. The filler’s rheology means that inserting the tip of the 4-mm 30-gauge needle into the border and exerting pressure produces an anterograde run of HA. This technique (Video 1) reduces the number of entry points and, therefore, lip trauma.
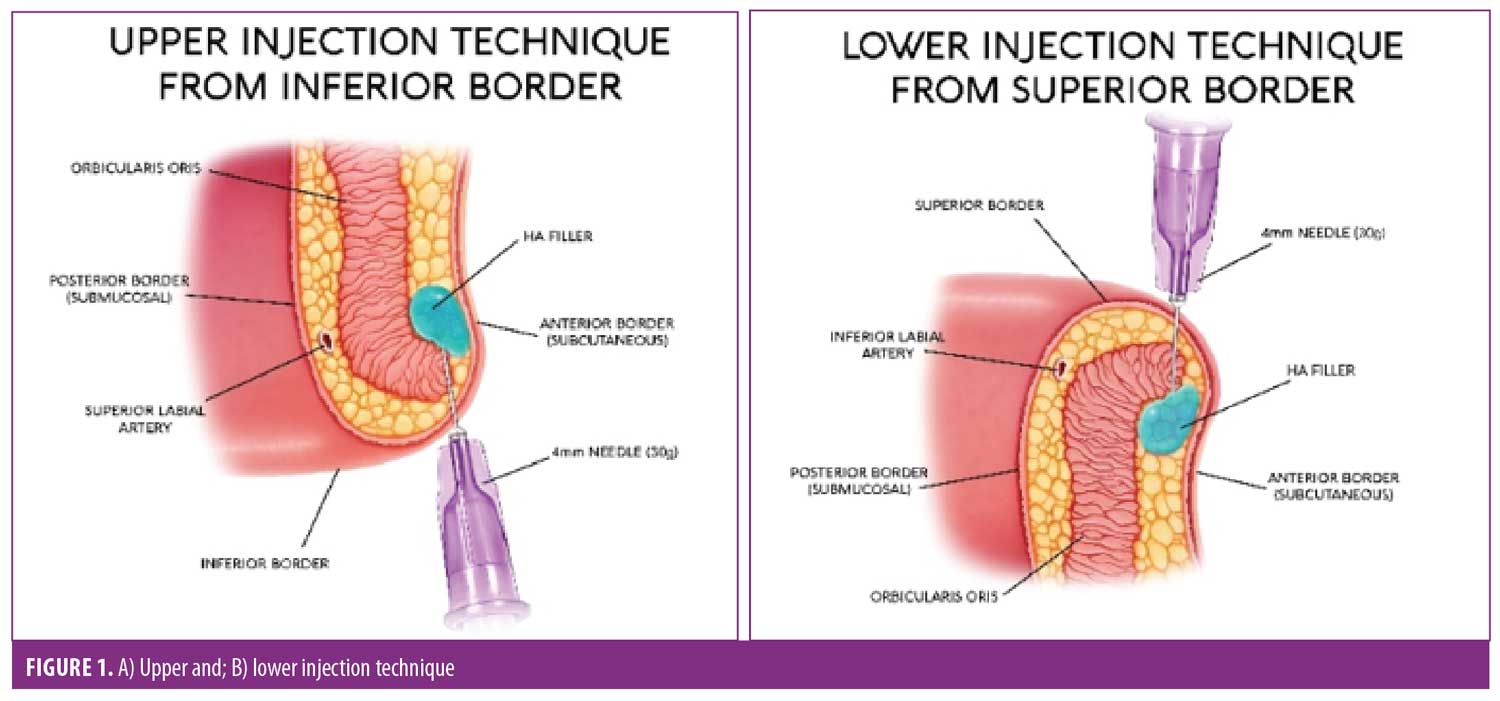
Using a 4-mm needle to inject into the upper and lower lips from anteroinferior and anterosuperior positions, respectively (Figure 1), may allow for safer placement of HA fillers than administration into subcutaneous perioral fat. This, in turn, reduces the risk of intravascular injection. Clinicians injecting from the posterior or mucosal side of the lip promote a greater risk of injury to the labial vessels. Using a 13-mm needle further increases the chance of perforating the labial vessels.
Ongoing clinical experience using this technique suggests areas for further study. The presence of anterogradely running filler could arise from hydrodissection induced by the filler pressure. Possibly,the filler may run along a currently unidentified discrete anatomical tube or space. Anecdotally, in our experience using 4-mm technique, we have observed that the technique reduces pain. This probably reflects the lower pressure necessary to extrude the filler into the highly innervated lip tissue relative to as seen with the conventional approach. However, quantifying the reduction in pain requires further study.
Conclusion
Anatomical evidence suggests that injecting HA filler into the subcutaneous plane is safer than administrating it into the submucosal plane. The anatomical evidence also suggests that the midline may be a higher-risk area for adverse outcomes following the injection of HA fillers. Moreover, varying depths of the labial vessels suggest that using 4-mm needles constitutes a safer approach to lip augmentation using HA filler than when using 13-mm needles. Once again, we would like to credit Dr. Sebagh for pioneering the use of the 4-mm 30-gauge needle in the context of lip injections.
Acknowledgments
The authors acknowledge the editorial support of Mark Greener and MedSense Ltd.
References
- Tansatit T, Apinuntrum P, Phetudom T. A typical pattern of the labial arteries with implication for lip augmentation with injectable fillers. Aesthetic Plast Surg. 2014;38(6):1083–1089.
- Lee S-H, Gil Y-C, Choi Y-J, et al. Topographic anatomy of the superior labial artery for dermal filler injection. Plast Reconstr Surg. 2015;135(2):445–450.
- Cotofana S, Pretterklieber B, Lucius R, et al. Distribution pattern of the superior and inferior labial arteries: impact for safe upper and lower lip augmentation procedures. Plast Reconstr Surg. 2017;139(5):1075–1082.
- Pinar YA, Bilge O, Govsa F. Anatomic study of the blood supply of perioral region. Clin Anat. 2005;18(5):330–339.
- Al-Hoqail RA, Meguid EMA. Anatomic dissection of the arterial supply of the lips: an anatomical and analytical approach. J Craniofac Surg. 2008;19(3):785–794.
- Edizer M, Magden O, Tayfur V, et al. Arterial anatomy of the lower lip: a cadaveric study. Plast Reconstr Surg. 2003;111(7):2176–2181.
- Magden O, Edizer M, Atabey A, et al. Cadaveric study of the arterial anatomy of the upper lip. Plast Reconstr Surg. 2004;114(2):355–359.
- Sebagh JL. Lip technique with hyaluronic acid. YouTube. Available at: https://www.youtube.com/watch?v=PEiFbnsjGV4. Published November 18, 2016. Accessed September 2020.