by Michael H. Gold, MD, Medical Director, Gold Skin Care Center and The Laser & Rejuvenation Center, Nashville, Tennessee; The Laser & Rejuvenation Center, Nashville, Tennessee
Amy Pope, PA-C, The Laser & Rejuvenation Center, Nashville, Tennessee
Disclosure: Dr. Gold is a consultant to, speaks for, performs research for, receives honoraria from, and owns stock in DUSA Pharmaceuticals. He is also a consultant to, speaks for, performs research for, and receives honoraria from Cynosure.
Abstract
Fractional resurfacing has become a very popular laser modality in recent years, and photodynamic therapy (PDT) has become a mainstay of many practices treating a wide array of clinical entities. In this case report, we describe a recalcitrant verrucous lesion on the foot that is unresponsive to cryotherapy, pulsed dye laser, and pulsed dye laser with PDT. The lesion did, however, respond very well to the use of a fractional laser to enhance the penetration of the PDT photosensitizer and then responded to pulsed dye laser with PDT. Fractional resurfacing prior to PDT may be a novel dermatologic treatment approach, making PDT an even better treatment option in the future.
(J Clin Aesthetic Derm. 2008;1(1):30–33)
********************************************************************************************************************************************************
Fractional resurfacing has become one of the most popular dermatologic surgical laser procedures performed in today’s laser world. A variety of devices have been developed recently that fit into the fractional laser armamentarium. Recently, these have been classified as either nonablative fractional resurfacing devices or ablative fractional devices. Basically, these devices work by creating “holes” in the skin with adjacent areas of normal skin, and this can be done in either a nonablative or an ablative mode. These devices have been recently reviewed.[1]
The use of photodynamic therapy (PDT) with aminolevulinic acid (ALA) has grown tremendously in the US over the past several years. The Food and Drug Administration (FDA) approved indication for the use of ALA-PDT in the United States is for the treatment of nonhyperkeratotic actinic keratoses (AK) of the face and scalp utilizing a 14- to 18-hour drug-incubation period and exposure to a blue-light source for 16 minutes and 40 seconds.[2] All other uses, including the common US uses—photorejuvenation with or without associated AK, treatment of moderate-to-severe inflammatory acne vulgaris, treatment of sebaceous gland hyperplasia, and treatment of hidradenitis suppurativa—are considered off label by the FDA. Therefore, each time we utilize this therapy in an off-label mode, we must inform our patients.[3]
Verrucae are common entities routinely seen in dermatology offices. They come in a variety of sizes and may coalesce to form large lesions. In certain areas of the body, such as the feet, pain and functional abnormalities among patients with verrucae have routinely been reported.[4]
Treatment options for verrucae are varied and numerous. Most of these treatment options rely on destruction of the lesion (i.e., the viral cell) and commonly include cryotherapy,[5] curettage, excision, carbon dioxide laser therapy,[6] pulsed dye laser therapy,[7] electrosurgery, and the use of topical acid medications.[8,9] Other therapies have also been reported, including infrared coagulation,[10] topically applied 5-fluorouracil,[11] intralesional bleomycin,[12] and topically applied dinitrochlorobenzene.[13] However, despite all of these modalities, many verrucae remain resistant to these therapies.
PDT has been used in the past to treat recalcitrant verrucous lesions.[14–20] We describe a case in which PDT and fractional resurfacing were utilized together in an attempt to enhance the effects of PDT on a recalcitrant verrucous lesion on the foot.
Case Report
We identified a 33-year-old man who had a recalcitrant verrucous lesion on his left foot for more than 10 years. The patient had previously undergone cryotherapy, pulsed dye laser treatment, pulsed dye laser multiplexed with 1064-nm laser, ALA with pulsed dye laser, and ALA with pulsed dye laser and multiplexed 1064-nm laser. All of these therapies failed to reduce this recalcitrant lesion, as seen in Figure 1.
{kind=link}
The patient then presented for a novel therapy, previously not described. The affected area was treated using the erbium YAG (2940nm) fractionated device (ProFractional®, Sciton, Palo Alto, California). The settings for the ProFractional® device were 450 microns and a 1.9-percent overlap. Following the therapy, ALA-PDT (Levulan® Kerastick®, DUSA Pharmaceuticals, Inc., Wilmington, Massachusetts) was applied and occluded for 24 hours. The patient returned 24 hours later and the subjected areas were then treated with a pulsed dye laser. The settings on this pulsed dye laser were: 595nm, 10 joules/cm2, spot size 7mm, 1Hz, 0.5 microseconds, with two passes. One month following the treatment, the lesion was markedly reduced in size, as shown in Figure 2.
{kind=link}
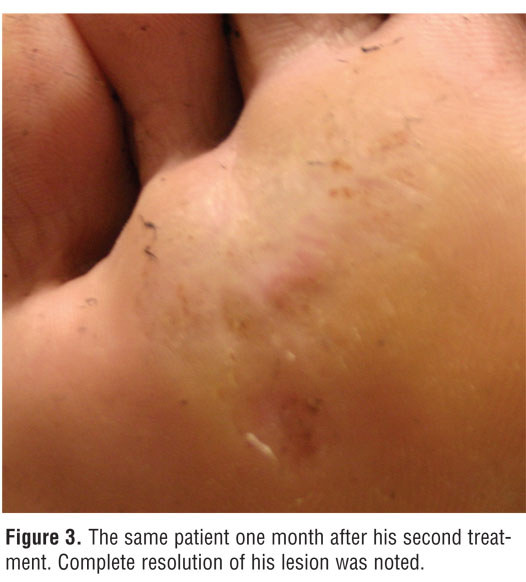
A second therapy was performed one month later, utilizing the ProFractional® device at 600 microns and a 2.0 percent overlap. Once again, ALA was applied under occlusion for 24 hours. The patient returned for a pulsed dye laser treatment utilizing the same settings as the first treatment. One month later, complete resolution of the lesion was obtained, as shown in Figure 3. The patient has maintained this clearing for two months following this last treatment.
{kind=link}
Discussion
Amman, et al.,[14] reported on the use of PDT in six patients with recalcitrant verrucous lesions on the hands. All of the patients had numerous other therapies before receiving their PDT treatments. The average time duration for these verrucous lesions was from 2 to 10 years. A 20% ALA oil-in-water emulsion was utilized under occlusion for 5 to 6 hours before exposure to a slide projector used as a light source for 30 minutes. Two months following the treatments, the areas treated still showed an inflammatory skin eruption surrounding the verrucous lesion. One of the six patients treated showed a complete response in the verrucous lesion; the other five did not respond.
In 1997, Smetana, et al.,[15] reported their experience with recalcitrant verrucae and molluscum lesions in two patients. In the verrucous-lesion patient, a 15-year, post-kidney-transplant patient presented with recalcitrant verrucae on the hands. The researchers utilized a 20% ALA cream containing 2 percent ethylenediaminetetracetic acid and 2 percent dimethyl sulfoxide applied to the recalcitrant lesions. The ALA was incubated on the lesions for four hours and therapy was performed utilizing a red-light source. The lesions showed dramatic improvement at the one-month follow-up period and no recurrences were noted two years later.
In the first described placebo-controlled clinical trial of recalcitrant verrucae with PDT, Stender, et al.,[16] (in 2000) described their findings in 232 hand and foot verrucous lesions found in 45 individuals. Lesions received either ALA-PDT or a placebo with a four-hour, under-occlusion-drug incubation treated with a red-light source. Patients received three weekly treatments and, if needed, an additional treatment given at one month following the third treatment. Follow-up at 14 weeks showed a reduction in wart area of 98 percent in the ALA group versus 52 percent in the placebo group. At 18 weeks, the relative reduction seen was 100 percent in the ALA group versus 71 percent in the placebo group. Patients in the ALA group noted more pain than those in the placebo group.
In 2001, Fabbrocini, et al.,[17] reported their findings with patients who had recalcitrant plantar verrucous lesions. In this clinical trial, they evaluated 67 patients whose verrucae were pretreated for seven days with an ointment containing 10% urea and 10% salicylic acid. The patients’ verrucae were then gently curettaged before a 20% ALA-cream preparation was applied. The lesions were occluded for five hours. Sixty-four lesions were treated with the ALA cream, while 57 lesions were treated with only the cream base. A tungsten lamp was used as the photoactivator, emitting light in the 400- to 700-nm range. Patients received one treatment, and if they showed no signs of clearing, they received two additional therapies at one-week intervals. They were then followed for up to two years. Results showed that 75 percent of the ALA-treated lesions completely cleared compared with 22.8 percent of the cream-only-treated lesions. Of interest, 47.9 percent of the ALA-treated lesions cleared with only one treatment.
Other treatments have shown further encouraging results with the use of ALA-PDT in the treatment of recalcitrant verrucae. Stender, et al.,[18] evaluated various light sources in 30 patients with a total of 250 recalcitrant verrucae of the hands and feet. A 20% ALA-cream preparation was used and lesions were incubated for five hours under occlusion before light exposure. Results showed complete clearance in 73 percent of the lesions with three white-light treatments, 71 percent after one white-light treatment, 42 percent after three red-light treatments, 23 percent after three blue-light treatments, and 20 percent after a series of up to four cryotherapy treatments.
In 2003, Mizuki, et al.,[19] reported on the use of ALA-PDT in plane warts of the face that were unresponsive to conventional therapies in a 13-year-old boy. A 20% ALA, oil-in-water emulsion was applied and a halide-light source utilized after a six-hour, under-occlusion-drug-incubation period. Two sessions and a five-month follow-up yielded complete resolution.
Smucler and Jatsova,[20] in 2005, reported on the use of ALA and a pulsed dye laser in the treatment of recalcitrant verrucae. In 112 lesions, they found that a pulsed dye laser cleared 81 percent of the lesions treated, with a mean of 3.34 sessions. ALA and the pulsed dye laser cleared 100 percent of the 86 treated lesions, with a mean of 1.95 sessions. Finally, a pulsed dye laser plus a light-emitting diode cleared 96 percent of the 76 treated lesions, with a mean of 2.53 sessions.
Recently, Ruiz-Rodriguez, et al.,[21] reported on the use of a fractional resurfacing device to enhance the efficacy associated with PDT-associated photodynamic rejuvenation. Four patients with mild-to-moderate rhytids in the perioral area were evaluated. The area was treated with two sessions of nonablative fractional resurfacing three weeks apart. Immediately following each nonablative fractional resurfacing, one half of the perioral area was treated with the methyl ester of 5-ALA. Three hours later, that area was illuminated with a red-light source. Evaluations of effectiveness were performed four and 12 weeks following the final treatment. An improvement in superficial wrinkles were noted in 3 of the 4 individuals studied, showing a potential enhancement with the use of a fractional device prior to ALA-PDT treatments.
Conclusion
The case presented shows that fractional resurfacing may be an effective pretreatment modality for ALA-PDT in patients with recalcitrant verrucae.[21] This is an intriguing therapeutic modality, and more work needs to be performed to further define the role of fractional resurfacing in enhancing the delivery of ALA and making ALA-PDT treatments more effective.
References
1. Gold MH. Fractional technology: a review and clinical approaches. J Drugs Dermatol. 2007;6: 849–852.
2. Gold MH, Goldman MP. 5-Aminolevulinic acid photodynamic therapy: where we have been and where we are going. Dermatol Surg. 2004;30: 1077–1084.
3. Nestor M, Gold MH, Kauvar A, et al. The use of photodynamic therapy in dermatology: results of a consensus conference. J Drugs Dermatol. 2006;5:140–154.
4. Stender IM. Treatment of human papilloma virus. In: Goldman MP, ed. Photodynamic Therapy. Munich, Germany: Elsevier;2005:77–88.
5. Bourke JF, Berth-Jones J, Hutchinson PE. Cryotherapy of common viral warts at intervals of 1, 2, and 3 weeks. Br J Dermatol. 1995;132:433–436.
6. Logan RA, Zachary CB. Outcome of carbon dioxide laser therapy from persistent cutaneous viral warts. Br J Dermatol. 1989;21:99.
7. Tan OT, Hurwitz TM, Stafford TJ. Pulsed dye laser treatment of recalcitrant verrucae, a preliminary report. Lasers Surg Med. 1993;13:127–137.
8. Hirose R, Hori M, Shukuwa R, et al. Topical treatment of resistant warts with glutaraldehyde. J Dermatol. 1994;21:248–253.
9. Bunney MH, Nolan MW, Williams DA. An assessment of methods of treating viral warts by comparative treatment trials based on standard design. Br J Dermatol. 1976;94:667–680.
10. Halasz CL. Treatment of common warts using the infrared coagulator. J Dermatol Surg Oncol. 1994;20:252–256.
11. Brodell RT, Breadle DL. The treatment of palmar and plantar warts using natural alpha interferon and a needless injector. Dermatol Surg. 1995;21:213–218.
12. James MP, Collier PM, Aherne W, et al. Histologic, pharmacologic, and immunocytochemical effects of injection of bleomycin. J Am Acad Dermatol. 1993;28:933–937.
13. Shah KC, Patel RM, Umrigar DP. Dinitrochlorobenzene treatment of verrucae plana. J Dermatol. 1991;18(11):639–642.
14. Amman R, Hunziker T, Braathen LR. Topical photodynamic therapy in verrucae. Dermatology. 1995;191:346–347.
15. Smetana Z, Malik Z, Orenstein A, et al. Treatment of viral infections with 5-aminloevulinic acid and light. Lasers Surg Med. 1997;21:351–358.
16. Stender IM, Na R, Fogh H, et al. Photodynamic therapy with 5-aminolevulinic acid or placebo for recalcitrant foot and hand warts: randomized double-blind trial. Clin Exp Dermatol. 1999;24(3):154–159.
17. Fabbrocini G, Costanzo M, Ricardo A, et al. Photodynamic therapy with topical 5-aminolevulinic acid for the treatment of plantar warts. J Photochem Photobiol B. 2001;61:30–34.
18. Stender IM, Lock-Anderson J, Wulf HC. Recalcitrant hand and foot warts successfully treated with photodynamic therapy with topical 5-aminolaevulinic acid: a pilot study. Clin Exp Dermatol. 1999;24:154–159.
19. Mizuki D, Kaneko T, Hanada K. Successful treatment of topical photodynamic therapy using 5-aminolaevulinic acid for plane warts. Br J Dermatol. 2003;149:1087–1088.
20. Smucler R, Jatsova E. Comparative study of aminolevulinic acid photodynamic therapy plus pulsed dye laser versus pulsed dye laser alone in the treatment of viral warts. Photomed Laser Surg. 2005;23:202–205.
21. Ruiz-Rodriguez R, Lopez L, Candelas D, Zelickson B. Enhanced efficacy of photodynamic therapy after fractional resurfacing: fractional photodynamic rejuvenation. J Drugs Dermatol. 2007;6:818–820.