by Amy Forman Taub, MD, Assistant Clinical Professor of Dermatology, Northwestern University Medical School, Chicago, Illinois; Founder/Director of Advanced Dermatology, Skinfo, SkinQRI, Lincolnshire, Illinois
Erin C. DeVita, CST, CMSLO, CCRC, Advanced Dermatology, SkinQRI, Lincolnshire, Illinois
Abstract
Introduction: Many laser and light devices have reported to be successful in the treatment of the flushing, background erythema, and telangiectasias that characterize erythematotelangiectatic rosacea including pulsed dye laser, potassium titanyl phosphate, intense pulsed light, and dual-wavelength lasers. A technology called ELOS (electro-optical synergy) combines pulsed light or laser with bipolar radiofrequency. This combination, developed in 2000, was based on the premise that these two forms of energy could be synergistic. One such device (Aurora SRA—skin-rejuvenation advanced handpiece, Syneron Medical Ltd., Yokneam, Israel) has a light spectrum of 470 to 980nm, energy up to 45J/cm2, and a range of radiofrequency energy of 5 to 25J/cm3 and is indicated for the treatment of vascular and pigmented lesions. Methods: We attempted to quantify the improvement of moderate-to-severe type-1 rosacea after three and five full-face treatments with this modality. Twenty-one patients with moderate-to-severe rosacea underwent five monthly full-face treatments with this device. The patients were evaluated with high-resolution photographs (Canfield Visia CR, Canfield, Fairfield, New Jersey) and self-evaluated via the National Rosacea Society’s official “Scorecard.” Results: Erythema and telangiectasia (physician assessed) as well as flushing and global status (patient assessed) achieved improvement that was statistically significant. Five treatments were no more effective than three, although the photographs reveal subtle improvements. There were no significant adverse events. Conclusion: The results of this study suggest that the combination of optical and RF energies is effective for the treatment of rosacea. ELOS, as well as other vascular-focused lasers and light sources, provides an important treatment option for patients who fail medical therapy, reach a plateau in their response to medical therapy, or wish to avoid chronic oral therapy.
(J Clin Aesthetic Derm. 2008;1(1)37–40)
Many laser and light devices have been reported to be successful in the treatment of the flushing, background erythema, and telangiectasias that characterize type-1 rosacea, also known as erythematotelangiectatic type.[1] Pulsed dye laser (PDL),[2] potassium titanyl phosphate (KTP),[3] intense pulsed light (IPL),[4] and dual-wavelength lasers[5] have all been reported to improve the signs and symptoms of rosacea.
A technology called ELOS (electro-optical synergy)[6] combines pulsed light or laser with bipolar radiofrequency (RF). This combination, developed in 2000, was based on the premise that the two forms of energy could be synergistic.[7] One study found this combination therapy to be more effective for photorejuvenation[8] than IPL alone.[9] One such device (Aurora SRA—skin-rejuvenation advanced handpiece, Syneron Medical, Ltd., Yokneam, Israel) has a light spectrum of 470–980nm with an energy up to 45J/cm2 and a range of RF energy of 5 to 25J/cm3 and is indicated for the treatment of superficial benign and persistent vascular and pigmented lesions. We attempted to quantify the improvement of moderate-to-severe type-1 rosacea after three and five full-face treatments with this modality.
Materials and Methods
Inclusion and exclusion criteria. Twenty-one patients with moderate-to-severe rosacea who were at least 30 years of age and were diagnosed with rosacea at least one year prior were recruited for participation in the study. Exclusion criteria were no vascular laser treatment within one year; no collagen injections or chemical peels within the past six months; and no laser resurfacing, nonablative resurfacing, phenol peels, or 30 percent or more trichloroacetic acid (TCA) peels within the past two years. Moderate-to-severe rosacea was defined as having a baseline erythema greater than two on a scale of 0 to 3, based on the investigator’s examination. All patients were required to have not started any new topical or oral therapies for the previous three months and to continue the same for the duration of the study.
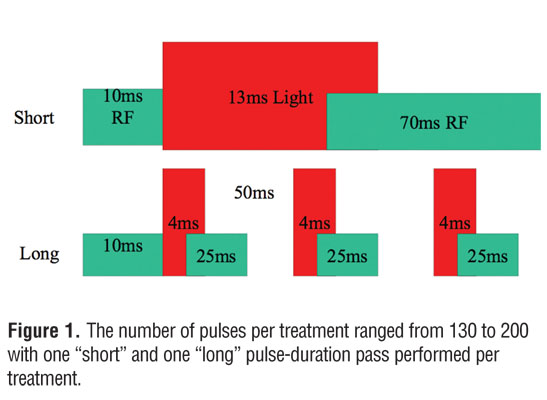
Procedure. Five full-face, monthly treatments with ELOS (light 470–980/bipolar RF) were performed. The parameters of the treatment were: optical energy of 23 to 36J/cm2, RF energy of 20 to 25J/cm3, contact cooling set at 10°C, ISM (impedence safety monitoring—see discussion for explanation) 14 to 18, and ISL (impedence safety limit) of 22. The number of pulses per treatment ranged from 130 to 200 with one “short” and one “long” pulse-duration pass performed per treatment (Figure 1). Short passes were performed horizontally on the face and long passes were performed vertically. Ultrasound gel was applied prior to the procedure and a cold-air device was utilized throughout the procedure (Zimmer Air Chiller, Fischer Medzin Technik, Germany).
{kind=link}
Assessment. An evaluation of the following parameters was performed: flushing, nontransient erythema, papules/pustules, and telangiectasia. Assessments were performed by the treating clinician on a quartile scale (0=absent, 1=mild, 2=moderate, 3=severe) based on clinical assessment and high-resolution photographs (Canfield Visia CR, Canfield, Fairfield, New Jersey), and the patients assessed themselves based on the National Rosacea Society’s official “Scorecard” (Figure 2).
{kind=link}
Follow-up. Follow-up was performed one month after three treatments (before the fourth treatment), one month after five treatments, and three months after five treatments.
Results
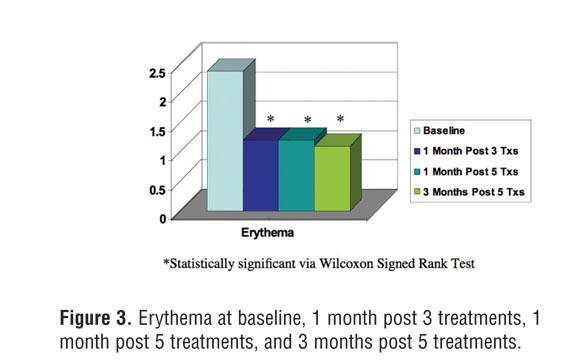
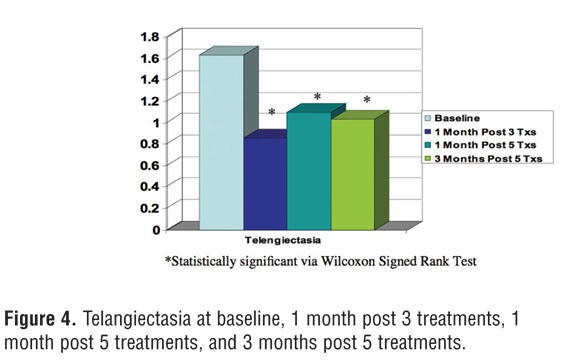
The treating physician evaluated at baseline the nontransient erythema on average as 2.38/3, and the patients rated their telangiectasias plus erythema as 2.43/3. These ratings fell to 1.21 and 1.17 one month after the third treatment, 1.21 and 1.23 one month after the fifth treatment, and 1.1 and 1.27 three months after the fifth treatment. All of these were statistically significant by the Wilcoxon signed rank test (Figure 3). Similarly, the telangiectasias were graded at baseline by the physician as 1.64, one month after three treatments as 0.86, one month after five treatments as 1.1, and three months after five treatments as 1.01, and all were statistically significant (Figure 4). Patients’ assessments of flushing diminished from 1.8 to 0.6 and 0.8 at one month after three treatments and three months after five treatments, respectively (Figure 5). Patients’ global assessments of their rosacea overall at baseline was 2.36/3.0, one month after three treatments was 1.02, one month after five treatments was 1.17, and three months after five treatments was 1.14, again all were statistically significant (Figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The photographs of patients’ results reveal significant apparent improvement in overall redness and telangiectasia (Figure 7). As noted above, the numerical grading of the results by both investigating physicians and patients were not significantly different one month after three treatments versus three months after five treatments. Figure 8 shows a subjective improvement in skin tone with five treatments as opposed to three.
{kind=link}
{kind=link}
Discussion
Many patients with rosacea plateau at some level, even with optimal medical therapy. Examining the package insert for metronidazole gel 1% (Metrogel, Galderma, Fort Worth, Texas) used once per day reveals a 10-week reduction of 50 percent of papules and pustules and a 39-percent investigator-assessed global improvement of clear or almost clear.[10] In a study comparing metronidazole 1% gel with azelaic acid 15% gel bid, both arms achieved a 75- to 80-percent improvement in acneiform component and a 42-percent improvement in erythema.[11] The Phase-III study of anti-inflammatory-dose doxycyline did not evaluate patients with erythematotelangiectatic rosacea.[12]
From the foregoing, it is clear that type-2 rosacea (papulopustular) is much easier to control with topical therapy, oral antibiotics, and anti-inflammatory medications, although type 1 is more prevalent. Patients who have both types 1 and 2 can get their acneiform component controlled and decrease their erythema to a degree, but telangiectasias persist in the 0.3- to 2.0-mm range. The background redness, probably caused by a dense diffuse network of telangiectasias less than 0.3mm, is variably influenced by medical therapies. The degree of symptoms, such as flushing, frequency and severity, burning, itching, and edema, seem to be more closely correlated with this component than with the fixed telangiectatic component.
Although the cause of rosacea is unknown, the common end result appears to be these reactive vessels. Treatment with vascular lasers makes sense in that it can reduce the density of these vessels. An early study with PDL showed good-to-excellent reduction in telangiectasia and erythema in 27 patients.[2] A study of 40 patients treated with purpuragenic doses of PDL showed a slight-to-moderate improvement in erythema and telangiectasia, although three patients flared and six patients developed postinflammatory hyperpigmentation.[13] In an attempt to tie laser treatment to changes in neuropeptide expression, 32 patients were treated with a single PDL treatment and the majority showed decreased stinger test scores after treatment as well as a reduced number of protein gene product 9.5 positive fibers in the dermis as well as substance P in the papillary dermis.[14]
Treatments with IPL have also shown to be effective. In a study of 32 patients treated with IPL,4 83 percent experienced improved erythema and 75 percent noted reduced flushing. Another study of 508 sites revealed a 77.8-percent clearance rate.[15] Measuring vascular parameters in four patients after a single IPL treatment by a scanning laser Doppler, a 30-percent decrease in blood flow, a 21-precent decrease in intensity of erythema, and a 29-percent decrease in the actual area of the cheek occupied by telangiectasia were noted. IPL systems do have some advantages over PDLs. The pulse duration can be varied and energy can be divided into packets of a few pulses. Wavelengths range from visible to infrared, allowing the energy to reach telangiectasias at various dermal depths. The spot size is also larger, making it easier to treat the entire face. In addition, purpura is less likely to occur with IPL.[5,9]
Although efficacious, light-based therapies for dermatologic conditions are limited because they must penetrate the epidermis to reach their targets. Optical energy is absorbed by epidermal melanin, thus reducing the amount of energy available to cause thermal injury to targets such as hair follicles or blood vessels. If the optical energy is increased for greater penetration, the risk of epidermal injury or hyperpigmentation increases. The choice of energy level is a trade-off between efficacy and safety.[7]
Selective electrothermolysis overcomes the limitations to light-based therapies.[7] With this approach, electrical energy from RF current selectively heats the target tissue without injuring the epidermis. RF current from the electrodes placed on the skin goes through the epidermis and travels to tissues of high electrical conductivity. Since conductivity varies inversely with temperature, cooling the epidermis drives the RF current to deeper tissues, which, when pre-heated with light, have increased conductivity and thus greater likelihood of receiving the RF current. The amount of heat produced in the pre-heated tissue depends on the tissue’s electrical resistance (impedance) to the flow of RF current.
ELOS systems offer monitoring to guard against overheating the skin.[4]Before treatment, the user selects a maximum percentage decrease in impedance (up to 30 percent, corresponding to a similar increase in temperature) that the patient can tolerate with each pulse. This maximum is the Impedance Safety Limit (ISL). If the ISL is set at 25 percent and the impedance decreases (and the temperature increases) by that amount before completion of a pulse, the system automatically stops the pulse, preventing thermal injury to the skin. ELOS also measures the percentage decrease in impedance—the impedance safety measurement (ISM)—with each fired pulse.
Even with these safety measures, side effects can occur, as with any device. Complications with this device are similar to any other pulsed light system: overheating, superficial burns, footprinting, hyperpigmentation, and hypopigmentation. One side effect that is unique due to the RF component is called “arcing.” This can occur if all four corners of the metal rails on the handpiece are not in contact with the skin. In bipolar RF, the electricity flows from one rail to the other, which acts as a ground. If both rails are not in contact with the skin, the electricity must pass through the air and it will then “ground” through the closest target, in this case the skin, causing immediate overheating and second-degree burning of the skin. This can be avoided by careful technique, ensuring good contact at all times between the handpiece and the skin.
This is the first report to evaluate the safety and efficacy of the use of ELOS technology in the treatment of rosacea. Although not quantified by this study, the authors believe the RF enables effective treatment of larger telangiectasias as well as adding skin smoothing to the treatment. Some thought leaders continue to state that IPL is not as effective as PDL,[16] although studies show similar efficacies but patient preference for IPL therapy.[17] However, the main importance of all of these reports is that multiple types of therapy are necessary to improve the quality of patients’ lives and that vascular-focused laser and light sources should be thought of earlier in the treatment dialog and not as a treatment of last resort. All patients need to have ongoing maintenance of topical and light, ELOS, or laser therapy as rosacea is a chronic condition.
The results of this study suggest that the combination of optical and RF energies are effective in the treatment of rosacea. This technology may provide a treatment option to patients who fail medical therapy, reach a plateau in their response to medical therapy, or wish to avoid chronic oral therapy.
References
1. Crawford GH, Pelle MT, James WD. Rosacea 1. Etiology, pathogenesis, and subtype classification. J Am Acad Dermatol. 2004;51(3):327–341.
2. Lowe NJ, Behr KL, Fitzpatrick R, Goldman M, Ruiz-Esparza J. Flash lamp pumped pulsed dye laser for rosacea-associated telangiectasia and erythema. J Dermatol Surg Oncol. 1991;17(6):522–525.
3. West YB, ALster TS. Comparison of the long-pulse dye (580-595nm) and KTP (532nm) lasers in the treatment of facial and leg telengiectasias. Dermatol Surg. 1998;24(2):221–226.
4. Taub AF. Treatment of rosacea with intense pulsed light. J Drugs Dermatol. 2003;2(3):254–259.
5. Larson AA, Goldman MP. Recalcitrant rosacea successfully treated with multiplexed pulsed dye laser. J Drugs Dermatol. 2007;6(8):843–845.
6. Waldman A, Kreindle M. New technology in aesthetic medicine: ELOS electro optical synergy. J Cosmet Laser Ther. 2003;5(3–4):204–206.
7. Sadick NS. Combination radiofrquency and light energies: electro-optical synergy technology in esthetic medicine. Dermatol Surg. 2005;31(9 Pt 2):1211–1217.
8. Sadick NS, Alexiades-Armenakas M, Bitter P Jr., Hruza, G, Mulholland RS. Enhanced full-face skin rejuvenation using synchronous intense pulse optical and conducted bipolar radiofrequency energy (ELOS): introducing selective radiophotothermolysis. J Drugs Dermatol. 2005;4(2):181–186.
9. Bitter PH. Noninvasive rejuvenation of photodamaged skin using serial, full-face intense pulsed light treatments. Dermatol Surg. 2000;26:835–842; discussion 843.
10. Metrogel. http://www.metrogel.com/AboutMetro1/ AboutMetro1.aspx. Accessed April 30, 2008.
11. Wolf JE Jr, Kerrouche N, Arsonnaud S. Efficacy and safety of once-daily metronidazole 1% gel compared with twice-daily azelaic acid 15% gel in the treatment of rosacea. Cutis. 2006;77(4 Suppl):3–11.
12. Del Rosso JQ, Webster GF, Jackson M, et al. Two randomized phase III clinical trials evaluating anti-inflammatory-dose doxycycline (40-mg doxycycline, USP capsules) administered once daily for treatment of rosacea. J Am Acad Dermatol. 2007;56(5):791–802.
13. Tan ST, Bialostocki A, Armstrong JR. Pulsed dye laser therapy for rosacea. Br J Plast Surg. 2004;574:303–310.
14. Lonne-Rahm S, Nordlind K, Edstrom DW, Ros AM, Berg M. Laser treatment of rosacea: a pathoetiological study. Arch Dermatol. 2004;140(11):1345–1349.
15. Schroeter CA, Haaf-von Below S, Neumann HA. Effective treatment of rosacea using intense pulsed light systems. Dermatol Surg. 2005;31(10):1285–1289.
16. Comments made by Eric F. Bernstein, MD, while moderating the light and laser treatment section of the 2008 American Society of Laser Surgery and Medicine, April 4, 2008; Orlando, FL.
17. McMeekin TO, Lertzman, BH, Hahn H, Arcara K. Randomized study of intense pulsed light and pulsed dye laser in the treatment of facial telangiectasia. Presented at: the American Society for Laser Surgery and Medicine, April 4, 2008, Orlando, FL.
This paper was presented in part at the World Congress of Dermatology in Buenos Aires, Argentina, October 2007. Equipment fees and research grants were provided by Syneron Corporation.