by Martha Viera, MD; Sadegh Amini, MD; Ran Huo, BS;
Shasa Hu, MD; Margaret Oliviero, ARAP; Sara Bassalo, MD; and Harold Rabinovitz, MD
Introduction
Fibroepithelioma of Pinkus (FEP) is an uncommon subtype of basal cell carcinoma (BCC) with a distinct growth pattern first described by Hermann Pinkus in 1953 as a premalignant fibroepithelial tumor.[1,2] Pinkus noted four such lesions to have a peculiar histologic appearance that resembled both a reticulated seborrheic keratosis and a BCC. These lesions are frequently slow growing and found on the trunk or extremities of individuals between 40 and 60 years of age.[3] Clinically, they appear as benign, slowly enlarging, raised or pedunculated solid tumors with a constricted base and of variable color, including shades of pink, yellow, brown, or skin color. They are most commonly found on the trunk or extremities.[4–7] Several forms of FEP, including cystic, pleomorphic, eroded, and giant variants have been described. The differential diagnoses include intradermal and compound melanocytic nevi, pedunculated fibroma, fibroepithelial papilloma (acrocordon), granuloma, hemangioma, amelanotic melanoma, neurofibroma, seborreic keratosis, nevus lipomatosus, and nevus sebaceous.3,7 The definitive diagnosis is generally made by histopathology. As variants of BCC, FEP lesions illustrate the interaction and interdependence of stromal and epithelial components in BCC.[1]
Dermatoscopy and confocal microscopy are noninvasive adjuvant tools that allow the in-vivo evaluation of structures, colors, and patterns in the epidermis, dermoepidermal junction, and the papillary dermis not visible to the naked eye.[8] The term dermatoscopy was introduced by German dermatologist Johann Saphier in the 1920s.[9] The first Consensus Conference on Skin Surface Microscopy was held in 1989 in Hamburg and the Consensus Net meeting on Dermoscopy was held in Rome in 2001.[10] These meetings standardized the definitions of structures seen in benign and malignant pigmented lesions. In the last 10 years, dermatoscopy, also termed epiluminescence microscopy, has opened a new dimension in the examination of pigmented and non-pigmented lesions of the skin.[11]
Confocal microscopy, first introduced to the scientific community in 1957[12] uses an image-capturing device that produces in-vivo “optical sections” of an object under observation. This device provides cellular resolution images, which may be used to refine the differential diagnosis of lesions in clinical practice. Both confocal microscopy and dermatoscopy are believed to improve diagnostic accuracy. To our knowledge, the characteristics of FEP as seen on confocal microscopy have not been described.
We present a patient with FEP, which clinically resembled an intradermal nevus. The presence of dermatoscopic and confocal features assisted in the diagnosis, which was subsequently confirmed by histopathology.
Case Report
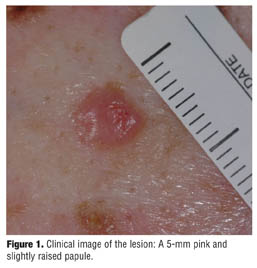
A 73-year-old Caucasian man presented to the dermatology clinic for a routine skin examination. On physical examination, numerous, sharply defined, light brown papules were found on the patient’s upper and mid back that clinically resembled seborrheic keratosis. Additionally, a 5-mm pink, asymptomatic, slightly raised papule was observed (Figure 1). The clinical diagnosis was most suggestive of an intradermal nevus. The dermatoscopic evaluation revealed a pink to light red lesion with linear vessels and white intersecting septal lines (Figure 2). The differential diagnosis was subsequently modified to include an “unusual” BCC, FEP, and intradermal nevus. Reflectance confocal microscopy at the dermo-epidermal junction demonstrated dark tumor silhouettes with clefting surrounded by thickened collagen (Figure 3). This pattern of basaloid islands have been described in BCC and are suggestive of a variant of BCC (in this specific case, a FEP). A shave biopsy was performed and the specimen sent for histopathologic evaluation with hematoxylin and eosin staining. Histology revealed elongating, branching, anastomosing cords of basaloid cells extending downward from the epidermis into the dermis, surrounded by a fibrous stroma confirming the diagnosis of FEP (Figure 4). Curettage and desiccation were performed and the patient was followed with no evidence of recurrence.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
Fibroepithelioma of Pinkus is an unusual neoplasm that is often difficult to diagnose as it simulates other malignant neoplasms of the skin. In our patient, the clinical presentation was most suggestive of an intradermal melanocytic nevus. However, the dermatoscopic pattern was most consistent with an unusual BCC or FEP. According to the literature, the pattern of FEP can be characterized by the presence of white streaks and fine arborizing vessels, either alone or associated with dotted vessels. Milia-like cysts and ulceration may also be observed. In pigmented FEPs, structureless, gray-brown areas of pigmentation and variable numbers of gray-blue dots may be seen.[13] Our patient’s dermatoscopic evaluation did not resemble an intradermal melanocytic nevus, which is characterized by a globular-homogeneous pattern, milia-like cysts, and comma-shaped vessels. Case series have shown that dermatoscopic images are useful in identifying FEPs (diagnosis confirmed with histopathology). In addition, confocal microscopy aided in the diagnosis of a basaloid tumor. These features included clefting and dark tumor silhouettes suggestive of basaloid tumor islands surrounded by thickened collagen.
Fibroepithelioma of Pinkus lesions can be easily missed clinically, as they often resemble benign lesions such as intradermal nevi and seborrheic keratoses. With our patient, the use of dermatoscopy and confocal microscopy aided in the diagnosis, which was confirmed with histopathology.
Treatment options for FEP are similar to those of BCC, including electrodessication and curettage, excision, or Mohs micrographic surgery. Fibroepithelioma of Pinkus is not known to have an aggressive clinical and biological course.
Fibroepithelioma of Pinkus is a neoplasm in which the clinical diagnosis represents a challenge. As shown in this case, adjuvant tools, such as dermatoscopy and confocal microscopy, are extremely useful in aiding in the diagnosis of difficult lesions. This is the first case in the literature describing the confocal features of FEP.
References
1. Arnold H, Odom R, and James W, eds. Andrew’s Diseases of the Skin, Clinical Dermatology. 8th ed. Philadelphia, Pa: WB Saunders Co; 1990:870.
2. Pinkus H. Premalignant fibroepithelial tumors of skin. AMA Arch Derm Syphilol. 1953;67(6):598–615.
3. Barr RJ, Herten RJ, Stone OJ. Multiple premalignant fibroepitheliomas of Pinkus: a case report and review of the literature. Cutis. 1978;21(3):335–337.
4. Bowen AR, LeBoit PE. Fibroepithelioma of pinkus is a fenestrated trichoblastoma. Am J Dermatopathol. 2005;27(2):149–154.
5. Bryant J. Fibroepithelioma of Pinkus overlying breast cancer. Arch Dermatol. 1985;121(3):310.
6. Jones CC, Ansari SJ, Tschen JA. Cystic fibroepithelioma of pinkus. J Cutan Pathol. 1991;18(3):220–222.
7. Cohen PR, Tschen JA. Fibroepithelioma of Pinkus presenting as a sessile thigh nodule. Skinmed. 2003;2(6):385–387.
8. Taylor S, Westerhof W, Im S, Lim J. Noninvasive techniques for the evaluation of skin color. J Am Acad Dermatol. 2006;54(5 Suppl 2):S282–S290.
9. Braun RP, Rabinovitz HS, Oliviero M, Kopf AW, Saurat JH. Dermoscopy of pigmented skin lesions. J Am Acad Dermatol. 2005;52(1):109–121.
10. Argenziano G, Soyer H, Chimenti S, Talamini R, Corona R, and Sera F. Dermoscopy of pigmented skin lesions: results of a consensus meeting via the internet. J Am Acad Dermatol. 2003;48:679–693.
11. Pehamberger H, Binder M, Steiner A, Wolff K. In vivo epiluminescence microscopy: improvement of early diagnosis of melanoma. J Invest Dermatol. 1993;100(3):356S–362S.
12. Minsky M. Memoir on inventing the confocal scanning microscope. Scanning. 1988;10:128–138.
13. Zalaudek I, Ferrara G, Broganelli P, et al. Dermoscopy patterns of fibroepithelioma of Pinkus. Arch Dermatol. 2006; 142(10):1318–1322.