Therapeutic and Aesthetic Uses of Photodynamic Therapy
Part one of a five-part series
by Michael H. Gold, MD
Medical Director, Gold Skin Care Center and The Laser & Rejuvenation Center, Nashville, Tennessee
Abstract
The utilization of aminolevulinic acid–photodynamic therapy in dermatology has steadily been on the rise since its introduction into our therapeutic armamentarium almost 10 years ago. Clinicians are realizing the continued benefits of this therapy from a therapeutic and cosmetic/aesthetic outcome. This was first seen in the treatment of nonhyperkeratotic actinic keratoses of the face and scalp where resolution of the actinic keratoses was achieved and a cosmetic improvement noted from the therapies. Clinicians are embracing photorejuvenation utilizing aminolevulinic acid–photodynamic therapy, which is reviewed in this article.
(J Clin Aesthetic Derm. 2008;1(2):32–37)
*****************************************************************************************************************************************
Photodynamic therapy (PDT) has become a recognized therapy in dermatology over the past 10 years and now is being utilized by many dermatologists on a regular basis to treat a variety of dermatologic disorders. This paper presents a series of review articles to help the reader understand which dermatologic entities are being treated through the use of PDT, the clinical trials which led to these uses, and how PDT is utilized in clinical practice. The first of these articles reviews how PDT is used in the treatment of actinic keratoses (AKs) and photorejuvenation of the skin.
PDT is a therapy that requires three ingredients—a photosensitizer, light, and oxygen. The most commonly used photosensitizers in dermatology are 20% 5-aminolevulinic acid (ALA) and its methyl ester, also known as MAL. In the United States, ALA is currently available for use, and MAL is in its final study phases. MAL is commonly used in other parts of the world. ALA is also available in Latin America and in parts of Asia, with more registrations expected in other countries in the near future.
ALA and MAL are selectively absorbed in the skin by actinically damaged skin cells, nonmelanoma skin cancer cells, and the pilosebaceous unit. It is because of this selectivity that both ALA and MAL are used to treat AKs and in photorejuvenation of the skin. MAL has been studied extensively for its use on nonmelanoma skin cancers and is widely used in Europe for this indication. Several studies have found that apoptosis, direct damage to actinically damaged cells and/or skin cancer cells, may be involved in the mechanism of action for both ALA and MAL.[1,2]
ALA in the United States is packaged as Levulan® Kerastick® (Dusa Pharmaceuticals, Wilmington, Massachusetts), which is a 20% 5-ALA solution (Figure 1). It has a Food and Drug Administration (FDA) clearance for the treatment of nonhyperkeratotic AKs of the face and scalp utilizing a blue light source for 16 minutes and 40 seconds following a drug incubation time of 14 to 18 hours. The blue light source most commonly used with ALA is known as the BluU® (Dusa Pharmaceuticals, Wilmington, Massachusetts) (Figure 2). MAL is also known as Metvix® (PhotoCure ASA, Norway; Galderma, Fort Worth, Texas) in Europe (Figure 3). It has European Union (EU) approval for the treatment of nonhyperkeratotic AKs of the face and scalp and basal cell carcinomas (BCCs) which are not suitable for conventional therapy. It is best utilized with a red light source, known commonly as the Aktilite® (Galderma, Fort Worth, Texas), as shown in Figure 4. Most recommend gentle curetting of the lesion prior to application of the MAL followed by three hours under occlusion of the MAL before exposure to the red light source. MAL, to be known as Metvixia® (Galderma Laboratories, Fort Worth, Texas) in the United States, is in the final stages of US clinical testing for its AK approval and may be available for use in the United States by the end of this year.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
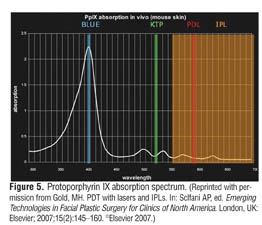
ALA is the photosensitizer most commonly used in the United States and will be the primary focus of the remainder of this manuscript. ALA is involved in the heme biosynthetic pathway and forms the rate-limiting step in that when utilized on the skin surface, ALA acts as a pro-drug, and is converted to protoporphyrin IX (PpIX), which can then be activated by an appropriate light source to create a PDT response. The absorption spectrum of PpIX is shown in Figure 5. From the figure, one can appreciate the main absorption peak, known as the Soret band, to be in the blue light range. There is also a large absorption peak in the red light range and smaller peaks where other lasers and light sources can be used in a PDT setting. It is from the utilization of a variety of lasers and light sources that the use of PDT in the United States has become so widespread.
{kind=link}
Pivotal Clinical Trials with ALA-PDT
In the Phase 2 clinical trial of ALA-PDT, 39 patients with nonhyperkeratotic AKs of the face and scalp were entered into the trial. Individual AKs were treated with ALA and each AK received 16 minutes and 40 seconds of blue light after a drug incubation of 14 to 18 hours. Pain was a common adverse event during and after treatment, and post-treatment erythema and edema, leading to crust formation for up to one week, was also observed by most of the study participants. Eight weeks following treatment, 66 percent of these individually treated AKs resolved (total clearance). A second treatment was given to the individual AKs which had not resolved with the first therapy and the percent total clearance increased to 85 percent.[3] As a secondary endpoint for the Phase 2 clinical trial, participants were also asked to judge their cosmetic appearance following the therapy. Ninety-four percent of the participants noted their cosmetic appearance as either good to excellent.
From the positive results attained from the Phase 2 clinical trial, a Phase 3, multicenter, placebo-controlled clinical trial was undertaken with 243 individuals. Treatment parameters were the same as the Phase 2 trials. Results showed that there was a greater than 70 percent complete clearance of individual AKs at 12 weeks; those not clear were treated again, and at 24 weeks, 88 percent of the individuals had a greater than or equal to 75-percent clearance of their AKs as compared to 20 percent in the placebo arm.[4] As was seen in the Phase 2 clinical trial, downtime with healing and pain (known as the PDT effect) was evident in the majority of individuals.
From these two clinical trials, ALA was FDA cleared for use in the United States. Thus, many dermatologists developed an interest in PDT, noting that ALA–PDT could successfully treat AKs while also producing a cosmetic benefit, an interesting finding in this era of cosmetic and aesthetic dermatology.
Open-Labeled ALA-PDT Clinical Trials
Several investigators began reporting their experiences with ALA–PDT shortly after the FDA approval. Many began looking at different ways to use ALA–PDT in their clinical practices because it would be easier to use than the conventional method of 14 to 18 hours of drug incubation and only through the use of a blue light source.
Interest in the treatment of photorejuvenation of the skin has been keen over the past 10 years as the development of lasers and light sources in the infrared and near infrared spectrum of light have been shown to improve many aspects of aging skin. This has also been of interest to those looking at PDT, as many of these same lasers and light sources are part of the absorption spectrum of PpIX and have been part of the PDT revolution of these past 10 years.
In 2002, Gold reported early experiences with ALA–PDT utilizing a blue light source.[5] His patients received individual treatment of their AKs with ALA and a 14- to 18-hour drug incubation before exposure to blue light for 16 minutes and 40 seconds. From this group, there appeared not only to be resolution of the treated AKs, but a response in contiguous areas to those being treated, resulting in a rejuvenation effect, as shown in Figure 6. A PDT effect was also evident in this series of patients.
{kind=link}
Armenakas et al, in 2003,[6] reported on the use of a long pulsed dye laser (PDL) in the individual treatment of AKs of the face and scalp. They demonstrated the safety and efficacy of the PDL in the treatment of AKs of the face and scalp. They demonstrated that short contact ALA (three hours) responded similarly to longer contact drug incubation (14–18 hours). A group of patients also had successful therapy of AKs on the extremities as well.
Investigators then began looking at shorter drug incubation times and treatment of the entire face to affect both clinical and subclinical AKs giving a full rejuvenation effect. Clinical reports soon appeared to support this hypothesis. Touma et al[7] demonstrated that a one-hour, drug-incubation time was as efficacious as a 14- to 18-hour drug-incubation time in improving AKs and the parameters of photodamage (i.e., photorejuvenation with a blue light source). Photorejuvenation improvements were noted in the sallowness of the skin, fine wrinkling, and mottled hyperpigmentation with a one-hour drug incubation as effective as a longer drug incubation time period.
Ruiz-Rodriquez et al[8] studied a shorter drug-incubation time (3 hours) with an intense pulsed light (IPL) source. This group of investigators treated 17 patients with an IPL device and showed that after two IPL sessions, all of the AKs cleared with the IPL–PDT therapy. They also showed an 87-percent improvement in skin texture, wrinkling, pigmentary changes, and telangiectasias. This was the first clinical trial utilizing the IPL device with PDT and they termed their therapy photodynamic photorejuvenation.
Other investigations followed. Gold et al[9] utilized a short drug-incubation time of 30 to 60 minutes in 10 patients and full-face ALA application. They found that 83 percent of the AKs responded to therapy. There was also improvement in crow’s feet in 90 percent, skin roughness in 100 percent, hyperpigmentation in 90 percent, and facial erythema in 70 percent. Goldman et al[10] looked at blue light and a one-hour drug incubation in 32 individuals. They found that 90 percent of the AKs responded to this therapy, 72 percent of individuals experienced improvement in skin texture, and 59 percent experienced improvement in pigment changes. In addition, they found that 62.5 percent of patients in their study preferred PDT over cryotherapy, perhaps the most common therapy performed for the treatment of AKs. Avram et al11 studied an IPL device in 17 patients with a one-hour, full-face drug incubation. In this study, 69 percent of the AKs responded with one IPL treatment, and there was a 55-percent reduction in telangiectasias, a 48-percent reduction in pigmentary dischromias, and a 25-percent improvement in skin texture. Alexiades-Armenakas et al12 studied 19 individuals with actinic cheilitis and a long-pulsed PDL. They showed a 68-percent clearance at 12 months in this treatment group with up to two treatments.
All of these studies supported the use of ALA–PDT in treating AKs, actinic cheilitis, and the signs of photorejuvenation, with fewer treatments than with other modalities. Gilbert13 looked at the pre-treatment of AKs prior to the use of ALA–PDT and found that by utilizing 5-fluorouracil topically for five nights prior to ALA–PDT, patients could achieve an even better result than conventional PDT alone, with clearance rates of 90 percent obtained with the combination therapy.
Split-Face Clinical Trials in the United States
Five split-face clinical trials have been published in the peer-reviewed literature utilizing ALA–PDT in the United States. The first, by Alster et al14, compared ALA with an IPL on one side of the face to IPL alone on the other side of the face in 10 individuals. They found that the ALA–IPL-treated side improved in the parameters of photorejuvenation compared to the IPL-treated side. Key[15] examined subjects utilizing a PDL with ALA on one half of the face. The ALA–PDL side improved in parameters of photorejuvenation more than the PDL side alone. Goldberg et al[16] examined a split-face ALA–IPL versus IPL alone and through skin biopsies examined the production of type-I collagen production. They found that there was a greater increase in type-I collagen production in those patients receiving ALA–IPL over IPL alone.
Dover et al[17] used an IPL protocol in which patients received three split-face ALA–IPL treatments at three-week intervals followed by two additional IPL full-face treatments. They were then evaluated at four weeks following the last IPL treatment. Twenty nine individuals participated in this clinical trial. The group found improvement in the global score for photoaging (80% PDT–IPL versus 50% IPL alone); mottled hyperpigmentation (95% PDT–IPL versus 65% IPL alone); and improvement in fine lines (55% PDT–IPL versus 20% IPL alone). No statistical changes were seen in tactile skin roughness or sallowness over baseline.
Gold et al[18] reported a split-face clinical trial utilizing ALA–IPL on one half of the face with an IPL on the other half. Three split-face treatments at four-week intervals, with follow-up at one and three months following the last treatment were performed. Thirteen patients were included in this study. The group found the following changes in the ALA–IPL side versus the IPL side: improvement in AKs (78% vs. 53.6%); crows feet (55% vs. 28.5%); tactile skin roughness (55% vs. 29.5%); mottled hyperpigmentation (60.3% vs. 37.2%); and in improvement in erythema (84.6% vs. 53.8%). No adverse effects were noted and no PDT effect was seen.
These trials confirmed the use of a short-contact, full-face ALA in the treatment of AKs and photorejuvenation. They also confirmed that a variety of lasers and light sources were successful when utilizing ALA–PDT and that with short-contact, full-face therapy, the PDT effect (commonly seen with long drug incubation PDT) could successfully be eliminated in most cases making the therapy more useful and more palatable for most dermatologists in the United States. PDT has continued to grow more and more each year.
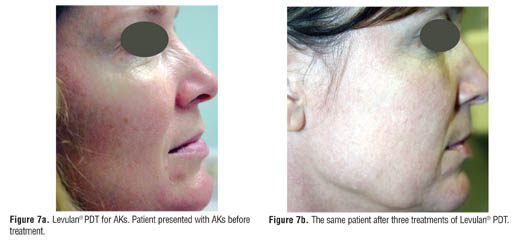
A recent report by Gold19 reviewed the pharmacoeconomics of utilizing ALA–PDT as compared to other commonly used AK treatments and found that ALA–PDT was economically feasible in these days of managed care and cost constraints among healthcare providers. Redbord and Hanke[20] reviewed a series of patients treated with ALA–PDT looking at the adverse events profiles seen in their patient population. Two adverse events, namely phototoxicity, were seen in 200 cases of PDT performed, again demonstrating the safety of this therapy when utilizing short-contact, full-face therapy. Ruiz-Rodriquez et al[21] recently reported on the use of a fractional laser device as a way to enhance the penetration of ALA into the skin when used prior to ALA–PDT treatments in a split-face study. They successfully showed that with the fractional laser prior to ALA application, periorbital lines and wrinkles improved more on the side that used the fractional laser prior to ALA–PDT. Examples of successful treatments with ALA–PDT are shown in Figure 6 and Figure 7. (Figure 8 shows a patient before and after treatment.)
{kind=link}
{kind=link}
The Methyl Ester of ALA
The second photosensitizer, Metvix®/Metvixia®, or MAL, is the methyl ester of ALA and is currently being used on a regular basis throughout Europe, Australia, and in other parts of the world. As has been stated, it has EU clearance for the treatment of nonhyperkeratotic AKs of the face and scalp and BCCs that are not suitable for conventional surgery. Conventional surgery includes excisional surgery, electrocautery and desiccation, and cryosurgery. Moh’s surgery is not usually included in their description of conventional therapy. Numerous clinical trials have been published to date, which, without question, demonstrate the efficacy of this product in the treatment of AKs, Bowen’s Disease, and nonmelanoma skin cancers. These have been thoroughly reviewed in previous manuscripts.[22,23]
In the United States, it is anticipated that MAL will be FDA approved for the treatment of nonhyperkeratotic AKs of the face and scalp. MAL is not FDA approved to treat BCCs and is not yet available for use in the United States.
MAL is best utilized with a red light source at 630nm and most recommend lesion preparation with a curette followed by three hours under occlusion of the drug prior to light exposure. Two treatments at one-week intervals are usually recommended. A PDT effect is usually reported with most of these treatments as a result of the longer drug-incubation period currently being utilized and due to the deeper penetrating red light source. Comparative clinical trials of Levulan® in a one-hour drug incubation, as is the standard in the United States today, and Metvix® in a three-hour drug incubation have not been performed to determine differences between efficacy and adverse events, although there have been reports suggesting there may be differences.[24,25]
Clinical trials for photorejuvenation with MAL are still in their infancy. The first, by Zane et al[27] looked at 20 patients with 137 AKs and severe photodamage. They found an 83.3-percent clearance of the AKs after two treatments, as well as improvement in photoaging, mottled hyperpigmentation, fine lines, roughness, and the sallowness of the skin. A PDT effect was evident in most patients.
There also have been three reported cases of allergic contact dermatitis to MAL,[28–30] and this remains a concern for those utilizing this therapy. Overall, MAL provides excellent clinical results; it will be utilized by many, perhaps even with changes to the recommended parameters for photorejuvenation as compared to skin cancer use.
Summary
ALA–PDT and MAL–PDT are both useful therapies for the treatment of AKs and photorejuvenation. Clinical trials have shown efficacy with both modalities in treating AKs and more work has been performed with ALA in the treatment of photorejuvenation, although MAL will work here too. Consensus papers for both therapies, which are useful guides for clinicians, have been published,[31,32] and may be helpful to those looking to enter the PDT field or those looking to expand their knowledge base. PDT has become a commonly used therapy to treat a variety of dermatologic disorders.
References
1. Nakaseko H, Kobayashi M, Akita Y et al. Histological changes and involvement of apoptosis after photodynamic therapy for actinic keratoses. Br J Derm. 2003;148:122–127.
2. Fantini F, Greco A, Cesinaro AM et al. Pathologic Changes after Photodynamic Therapy for Basal Cell Carcinoma and Bowen Disease. Arch Dermatol. 2008;144:186–194.
3. Jeffes EW, McCullough JL, Weinstein GD, et al. Photodynamic therapy of actinic keratoses with topical aminolevulinic acid hydrochloride and fluorescent blue light. J Am Acad Dermatol. 2001;45(1):96–104.
4. Jeffes EW. Levulan: the first approved topical photosensitizer for the treatment of actinic keratosis. J Dermatolog Treat. 2002;13(Suppl 1):S19–23.
5. Gold MH. The evolving role of aminolevulinic acid hydrochloride with photodynamic therapy in photoaging. Cutis. 2002;69(6 Suppl):8–13.
6. Alexiades-Armenakas MR, Geronemus RG. Laser-mediated photodynamic therapy of actinic keratoses. Arch Dermatol. 2003;139(10):1313–1320.
7. Touma D, Yaar M, Whitehead S, et al. A trial of short incubation, broad-area photodynamic therapy for facial actinic keratoses and diffuse photodamage. Arch Dermatol. 2004;140(1):33–40.
8. Ruiz-Rodriguez R, Sanz-Sanchez T, Cordoba S. Photodynamic photorejuvenation. Dermatol Surg. 2002;28(8):742–744.
9. Gold MH. Aminolevulinic acid photodynamic therapy for actinic keratoses and photorejuvenation. Expert Rev Dermatol. 2007;2(4):391–402.
10. Goldman MP, Atkin D, Kincad S. PDT/ALA in the treatment of actinic damage: real world experience. J Lasers Surg Med. 2002;14(S):24.
11. Avram DK, Goldman MP. Effectiveness and safety of ALA-IPL in treating actinic keratoses and photodamage. J Drugs Dermatol. 2004;3(1 Suppl):S36–S39.
12. Alexiades-Armenakas MR, Geronemus RG. Laser-mediated photodynamic therapy of actinic cheilitis. J Drugs Dermatol. 2004;3(5):548–551.
13. Gilbert DJ. Treatment of actinic keratoses with sequential combination of 5-fluorouracil and photodynamic therapy. J Drugs Dermatol. 2005;4(2):161–163.
14. Alster TS, Tanzi EL, Welch EC. Photorejuvenation of facial skin with topical 20% 5-aminolevulinic acid and intense pulsed light treatment: a split-face comparison study. J Drugs Dermatol. 2005;4(1):35–38.
15. Key DJ. Aminolevulinic acid-pulsed dye laser photodynamic therapy for the treatment of photoaging. Cosmetic Derm. 2005;18:31–36.
16. Marmur ES, Phelps R, Goldberg DJ. Ultrastructural changes seen after ALA-IPL photorejuvenation: a pilot study. J Cosmet Laser Ther. 2005;7:21–24.
17. Dover JS, Bhatia AC, Stewart B, et al. Topical 5-aminolevulinic acid combined with intense pulsed light in the treatment of photoaging. Arch Dermatol. 2005;141(10):1247–1252.
18. Gold MH, Bradshaw VL, Boring MM, et al. Split-face comparison of photodynamic therapy with 5-aminolevulinic acid and intense pulsed light versus intense pulsed light alone for photodamage. Dermatol Surg. 2006;32(6):795–801.
19. Gold MH. Pharmacoeconomic analysis of the treatment of multiple actinic keratoses. J Drugs in Dermatol. 2008;7(1):23–25.
20. Redbord KP, Hanke CW. Topical photodynamic therapy for dermatologic disorders: results and complications. J Drugs Dermatol. 2007;6(12):1197–1202.
21. Ruiz-Rodriquez R, López L, Candelas D, Zelickson B. Enhanced efficacy of photodynamic therapy after fractional resurfacing: fractional photodynamic rejuvenation. J Drugs Dermatol. 2007;6(8):818–820.
22. Lehmann P. Methyl aminolaevulinate-photodynamic therapy: a review of clinical trials in the treatment of actinic keratoses and nonmelanoma skin cancer. Br J Dermatol. 2007;156(5):793–801.
23. Pariser DM, Lowe NJ, Stewart DM, et al. Photodynamic therapy with topical methyl aminolevulinate (Metvix®) is effective and safe in the treatment of actinic keratosis: results of a prospective randomized trial. J Am Acad Dermatol. 2003;48:227–232.
24. Szeimies RM, Karrer S, Radakovic-Fijan S, et al. Photodynamic therapy using topical methyl 5-aminolevulinate compared with cryotherapy for actinic keratosis: a prospective, randomized study. J Am Acad Dermatol. 2002;47:258–262.
25. Freeman M, Vinciullo C, Francis D, et al. A comparison of photodynamic therapy using topical methyl aminolevulinate (Metvix®) with single cycle cryotherapy in patients with actinic keratosis: a prospective, randomized study. J Dermatolog Treat. 2003;14:99–106.
26. Gold MH. 5-Aminolevulinic acid photodynamic therapy versus methyl aminolevulinate photodynamic therapy for inflammatory acne vulgaris. J Am Acad Dermatol. 2008;58(2):S60–S62.
27. Zane C, Capezzera R, Sala R, Venturini M, Calzavara-Pinton P. Clinical and echographic analysis of photodynamic therapy using methylaminolevulinate as sensitizer in the treatment of photodamaged facial skin. Lasers Surg Med. 2007;39(3):203–209.
28. Wulf HC, Philipsen P. Allergic contact dermatitis to 5-aminolaevulinic acid methylester but not 5-aminolaevulinic acid after photodynamic therapy. Br J Dermatol. 2004;150:143–145.
29. Harris MJ, Street G, Gilmour E, et al. Allergic contact dermatitis to 5-aminolevulinic acid methyl ester. Photodermatol Photoimmunol Photomed. 2007;23:35–36.
30. Jungersted JM, Dam TN, Bryld LE et al. Allergic reactions to Metvix. Contact Dermatitis. 2008;58(3):184–186.
31. Nestor M, Gold MH, Kauvar A, et al. The use of photodynamic therapy in dermatology: results of a consensus conference. J Drugs Dermatol. 2006;5:140-154.
32. Braathen LR, Szeimies RM, Basset-Seguin N, et al. Guidelines on the use of photodynamic therapy for nonmelanoma skin cancer: an international consensus. International Society for Photodynamic Therapy in Dermatology. J Am Acad Dermatol. 2007;56(1):125-143.