
Volker Meyer, MD; Tobias Goerge, MD; Thomas A. Luger, MD; Stefan Beissert, MD
Department of Dermatology, University of Münster, Münster, Germany
Disclosure: Dr. Luger has received an honorarium as a speaker for Basilea Pharmaceutica, Munich, Germany. Drs. Meyer, Goerge, and Beissert report no relevant conflicts of interest. This clinical research is supported by a restricted grant from Basilea Pharmaceutica, Munich, Germany.Abstract
Palmoplantar hyperkeratotic psoriasis can be challenging to treat since micro-trauma induced by manual labor supports the development of new lesions via the isomorphic Koebner reaction. In this article, the authors report the successful treatment of severe palmoplantar hyperkeratotic psoriasis with etanercept and alitretinoin combination therapy. The results indicate that the new retinoid alitretinoin can be effectively used in combination with anti-tumor necrosis factor blocking agents for the treatment of psoriasis in individual cases. (J Clin Aesthet Dermatol. 2011;4(4):45–46.)
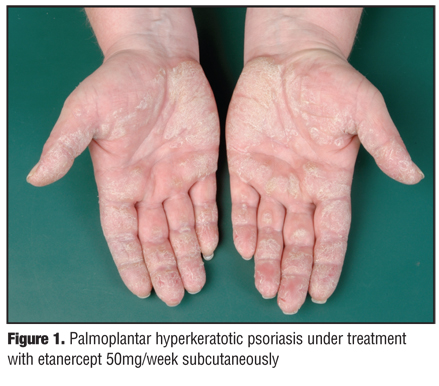
A 56-year-old Caucasian woman presented with a 12-month history of psoriasis with a Psoriasis Area and Severity Index (PASI) of 17. While working (which involved daily, intensive, manual activities) she developed marked palmoplantar hyperkeratosis with painful fissures, especially on the fingertips (Figure 1). Her past medical history revealed hypertension, which required antihypertensive medication. Psoriatic arthritis was ruled out.
{kind=link}
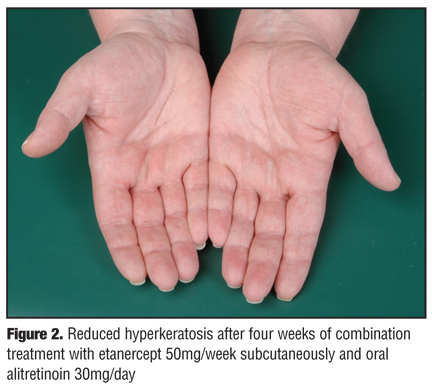
Her previous antipsoriatic treatment regimen consisted of methotrexate applied subcutaneously in doses up to 20mg weekly in combination with efalizumab with good control of her psoriasis, as evidenced by PASI scores ?5. After discontinuation of efalizumab, her psoriasis relapsed with PASI scores between 13 and 17. Subsequently, etanercept 50mg/week subcutaneously was initiated together with topical calcipotriol in combination with corticosteroids. The patient showed a good response with significant reduction of truncal plaques. However, severe hyperkeratosis persisted on the palms (Figure 1) and soles, which significantly impaired work. The addition of methotrexate 15mg/week subcutaneously did not improve palmoplantar lesions. Accordingly, methotrexate was discontinued, and after a wash-out period of two weeks, oral alitretinoin 30mg once daily was introduced in combination with etanercept. This combination treatment resulted in a marked reduction of palmoplantar hyper-keratosis within four weeks (Figure 2). After eight weeks of combination therapy, the lesions had disappeared completely. After 10 months, alitretinoin was discontinued, which resulted in a relapse of palmoplantar hyperkeratosis. Therefore, alitretinoin was reintroduced. Overall, combination therapy was well tolerated for a follow-up time of 13 months.
{kind=link}
Discussion
Psoriasis can develop on the palms and soles in approximately 15 percent of patients.[1] Patients with occupational manual work are especially at risk, and the isomorphic Koebner reaction may contribute to significant palmar hyperkeratosis refractory to conventional treatment. Topical vitamin D or corticosteroids as well as methotrexate were unable to effectively reduce palmar lesions in the patient discussed in this case. Therefore, the development of treatment regimens that target palmoplantar hyperkeratotic dermatitis is particularly relevant.
Alitretinoin (Toctino®, Basilea Pharmaceutica GmbH, Munich, Germany) is a pan-retinoid agonist, binding to all known retinoid receptors (retinoic acid receptor [RAR]-alpha, -beta, -gamma, and retinoid X receptor [RXR]-a,lpha -beta, -gamma) and is approved for the treatment of severe chronic hand dermatitis.[2,3] Potential side effects are dryness of mucous membranes, headache, elevated liver function tests, and blood lipid levels. The predominant retinoid receptors found in adult human skin are RAR-gamma and RXR-alpha. While RAR primarily regulates cellular differentiation and proliferation, RXR modulates cellular apoptosis. In vitro, alitretinoin showed more affinity to RAR than to RXR and was able to reduce the expression of inflammatory cytokines, such as tumor necrosis factor (TNF)-alpha, interleukin (IL)-1 beta, and IL-12 p40.[2,4]
Besides TNF-alpha, the IL-12/IL-23 axis plays an important role in the development of psoriasis.[5,6] Since alitretinoin can inhibit IL-12 p40 expression via interference with the RAR, the authors speculate that the beneficial therapeutic effects of alitretinoin might possibly be due to suppression of IL-12/IL-23 cytokines.
The authors’ findings show that alitretinoin can be used effectively in combination with etanercept and eventually other anti-TNF-alpha antibodies in patients with treatment-refractory palmoplantar hyperkeratotic psoriasis.
References
1. Kumar B, Saraswat A, Kaur I. Palmoplantar lesions in psoriasis: a study of 3,065 patients. Acta Derm Venerol. 2002;82:192–195.
2. Cheng C, Michaels J, Scheinfeld N. Alitretionin: a comprehensive review. Expert Opin Investig Drugs. 2008;17:437–443.
3. Ruzicka T, Larsen FG, Galewicz D, et al. Oral alitretinoin (9-cis-retinoic acid) therapy for chronic hand dermatitis in patients refractory to standard therapy: results of a randomized, double-blind, placebo-controlled, multicenter trial. Arch Dermatol. 2004;140:1453–1459.
4. Xu J, Drew PD. 9-Cis-retinoic acid suppresses inflammatory responses of microglia and astrocytes. J Neuroimmunol. 2006;171:135–144.
5. Nair RP, Duffin KC, Helms C, et al. Genome-wide scan reveals association of psoriasis with IL-23 and NF-kB pathways. Nat Genetics. 2009;41(2):199–204.
6. Gottlieb A, Menter A, Mendelsohn A, et al. Ustekinumab, a human interleukin 12/23 monoclonal antibody, for psoriatic arthritis: randomised, double-blind, placebo-controlled, crossover trail. Lancet. 2009;373:633–640.