Andrea Losch, MD; Katherine D. Chilek, DO; Matthew J. Zirwas
Andrea Losch, MD and Matthew J. Zirwas are from The Ohio State University, Columbus, Ohio; Katherine D. Chilek, DO, is from Ohio University, Athens, Ohio
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Angiosarcoma is an aggressive tumor that most commonly presents on the scalp or face of elderly patients; however, it can develop in patients with breast cancer following radiation and breast-conserving therapy, complicating 0.1 to 0.2 percent of such cases. Mammography and fine-needle aspiration, though often very useful in evaluating for breast carcinomas and cytological features, are often negative in early stages of angiosarcoma and difficult to interpret. We present the case of a 49-year-old Caucasian woman with a history of stage II invasive ductal carcinoma of the left breast who presented with a two-month history of increased firmness and tenderness in her left breast. On exam, her left breast had significant firmness and hardening of breast tissue with slight erythema of skin. Punch biopsy initially suggested angiosarcoma, but subsequent biopsies instead diagnosed an atypical vascular proliferation. This case represents a patient who presented with an atypical lesion concerning for angiosarcoma. Repeated biopsies were necessary to obtain the correct diagnosis. One biopsy may not be sufficient for distinguishing atypical vascular proliferation from angiosarcoma. We present this case to increase awareness of the difficulty in making this distinction.
(J Clin Aesthet Dermatol. 2011;4(4):47–48.)
Angiosarcoma is an aggressive tumor that most commonly presents on the scalp or face of elderly patients[1]; however, it can develop in patients with breast cancer following radiation and breast-conserving therapy, complicating 0.1 to 0.2 percent of such cases.[2,3] As the trend toward breast-conserving therapy rises, it is important for clinicians to be aware of the risk of secondary malignant tumors developing within previous radiation fields.[4]
The average time between radiation therapy for treatment of primary breast cancer and diagnosis of angiosarcoma varies from 48 to 144 months, or 4 to 12 years, based on data from five different articles.[3–7] However, Billings et al[6] found that the interval to development of postradiation angiosarcoma was less than 36 months in 5 of 27 cases. Angiosarcoma following breast radiation for breast carcinoma typically presented as “blue-ish or purple nodules of the skin, purple discolorations, erythematous macules, sometimes combined with ulceration, edema, or a palpable mass.”[4]
Mammography and fine-needle aspiration, though often very useful in evaluating for breast carcinomas and cytological features, are often negative in early stages of angiosarcoma and difficult to interpret.[2,4] If the diagnosis is confirmed, the most widely used treatment for secondary angiosarcoma following breast radiation is mastectomy with wide tumor-free margins.[4]
Case
The authors present the case of a 49-year-old Caucasian woman with a history of stage II invasive ductal carcinoma of the left breast who presented with a two-month history of increased firmness and tenderness in her left breast. She had undergone a lumpectomy, sentinel node biopsy, chemotherapy, and radiation eight months prior to presentation. At the time of presentation to the authors’ hospital, her symptoms had been present for two months, and she had completed two courses of antibiotics for possible cellulitis with no improvement. Ultrasound evaluation of the left breast was negative for fluid collection or abscess. Her white blood cell count was normal and her erythrocyte sedimentation rate (ESR) was slightly elevated. The patient was afebrile during her hospital stay.
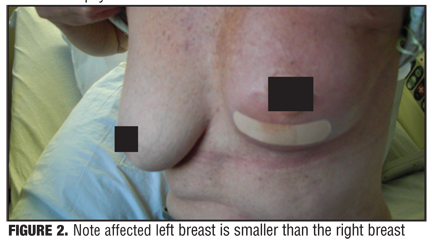
On exam, her left breast had significant firmness (Figure 1) and hardening of breast tissue with slight erythema of skin. Of note, she had neither eczematous changes of the skin or nipple nor any areas of fluctuance. Her left breast was significantly smaller and more firm than the right breast (Figure 2). There was no appreciable left axillary lymphadenopathy.
{kind=link}
{kind=link}
A punch biopsy was done which showed slightly increased numbers of irregularly shaped dilated vascular channels lined by prominent endothelial cells in the dermis, extending to the lateral specimen edges. Immunoperoxidase staining for CD31 was positive for endothelial cells lining vascular channels in the dermis. Immunoperoxidase staining for D240 revealed highly increased numbers of lymphatic channels in the dermis. Many perivascular lymphoid cells in the dermis as well as some cells lining vascular and lymphatic channels stained positive for Ki-67. The patient’s initial biopsy was determined to be angiosarcoma. The biopsy was sent for a second opinion to confirm, and at that point it was determined to be an atypical vascular proliferation rather than angiosarcoma. The patient underwent subsequent biopsies in all four quadrants of her breast. These findings were more consistent with atypical vascular proliferation and radiation changes rather than malignancy. It was determined that the patient should be followed clinically and did not need radical excision of the affected area.
Discussion
Postradiation vascular tumors have been described as two types: angiosarcoma postradiation and atypical vascular lesions.[8] The angiosarcoma postradiation is the malignant variant with significant mortality, and atypical vascular lesions behave in a benign manner.[8] However, histology and clinical presentation often show overlap and these vascular tumors may be on one disease spectrum.[8] It has been suggested that some forms of angiosarcoma have arisen from atypical vascular lesions.[1,8] A study of 42 patients ranging in age from 36- to 90-years old showed a substantial time difference between when patients presented with atypical vascular lesions (median 3.5 years) and cutaneous angiosarcoma, (median 6 years) postradiation.9 Stewart-Treves syndrome is distinct from angiosarcoma postradiation because it develops in an arm with chronic lymphedema following mastectomy and axillary lymph node dissection for breast cancer, rather than in a site that received radiation.[10]
The patient described in this case is unique in two ways. First, she presented with a firm, sclerotic, smaller breast, which was due to the underlying pathology rather than her breast surgery, lumpectomy. The authors’ initial differential diagnosis favored postradiation morphea, chronic radiodermatitis, or carcinoma erysipelatoides, as angiosarcoma does not commonly present with a diffuse, sclerotic, hard breast. Additionally, she presented eight months following radiation, which is an extremely short latency period between radiation therapy and angiosarcoma.
This case represents a patient who presented with an atypical lesion concerning for angiosarcoma. Repeated biopsies were necessary to obtain the correct diagnosis. One biopsy may not be sufficient for distinguishing atypical vascular proliferation from angiosarcoma. The authors’ present this case to increase awareness of the difficulty in making this distinction.
References
1. Kligman LH, Kligman AM. The nature of photoaging: its prevention and repair. Photodermatol. 1986;3:215–227.
2. El-Domyati M, Attia S, Saleh F, et al. Intrinsic aging vs. photoaging: a comparative histopathological, immuno-histochemical, and ultrastructural study of skin. Exp Dermatol. 2002;11:398–405.
3. Helfrich YR, Sachs DL, Voorhees JJ. Overview of skin aging and photoaging. Dermatol Nurs. 2008;20:177–183.
4. Uitto J. The role of elastin and collagen in cutaneous aging: intrinsic aging versus photoexposure. J Drugs Dermatol. 2008;7:S12–S16.
5. Sadick NS, Weiss R. Intense pulsed-light photorejuvenation. Semin Cutan Med Surg. 2002;21:280–287.
6. El-Domyati M, Attia S, Saleh F, et al. Effect of topical tretinoin on photoaged facial skin: a histometric, immunohistochemical and ultrastructural study. J Cosmet Dermatol. 2004;3: 191–201.
7. Kim KH, Geronemus RG. Nonablative laser and light therapies for skin rejuvenation. Arch Facial Plast Surg. 2004;6:398–409.
8. Sadick NS, Makino Y. Selective electro-thermolysis in aesthetic medicine: a review. Lasers Surg Med. 2004;34: 91–97.
9. Trelles MA, Allones I, Velez M. Nonablative facial skin photorejuvenation with an intense pulsed light system and adjunctive epidermal care. Lasers Med Sci. 2003;18:104–111.
10. Bogle MA, Ubelhoer N, Weiss RA, et al. Evaluation of the multiple pass, low fluence algorithm for radiofrequency tightening of the lower face. Lasers Surg Med. 2007;39: 210–217.