Michael H. Gold, MD
Dr. Gold is the founder and medical director of Gold Skin Care Center, Advanced Aesthetics Medical Spa, The Laser and Rejuvenation Center, and Tennessee Clinical Research Center located in Nashville, Tennessee. He is also Clinical Assistant Professor at Vanderbilt University School of Medicine and School of Nursing in Nashville, Tennessee; Visiting Professor of Dermatology, Huashan Hospital, Fudan University, Shanghai, China; and Visiting Professor of Dermatology, No. 1 Hospital of China Medical University, Shenyang, China. Dr. Gold has performed clinical research for Alma Lasers, Lumenis, and Sciton and speaks on their behalf.
Abstract
A variety of medical devices are described under the heading of tissue tightening devices. This article reviews the tissue tightening devices currently available in the United States and some that may receive clearance in the upcoming year. These include the various radiofrequency devices as well as the pulsed light devices that achieve similar end results. The one noticeable factor seen with this group of devices is the paucity of large, clinical, controlled trials that appear in the medical literature for this group of medical devices as a whole.
Introduction
Tissue tightening, or noninvasive skin tightening, is a popular concept in 2010 as more devices have entered the market. Although this article is an update of a previous report written several years ago, the players, with minimal difference, remain the same.[1] The basic premise of these devices is the same—whether one is evaluating a radiofrequency (RF) device or a pulsed light device targeting water as its chromophore—there is initial collagen contraction and destruction through both mechanical and biochemical pathways. As a result of the deep delivered energy into the skin, collagen remodeling through a controlled wound healing response occurs over time with associated neocollagenesis. This collagen remodeling also yields the desired tissue tightening that is seen with these devices.
Appropriate cooling is also required for these devices, since the energy delivered needs to penetrate to the deep dermal and subcutaneous fat layers without damaging the more superficial structures.
It is also important to note that these devices have evolved over the years. At first, most noted that these devices, in order to achieve their desired results, created a great deal of pain, on many occasions requiring anesthesia of some variety for the procedure to be successfully performed. We now know that these devices can work very well with reduced energy settings and that they do not need to be performed under anesthesia, which makes the procedure more palatable and ultimately safer for our patients. The second major area that needs to be fully understood is that for tissue tightening devices to be successful, there must be appropriate patient selection. Not every patient can be treated successfully with these devices, and unfortunately, when these devices were first introduced, many reported how well everyone would respond to the therapy. Patient selection is key for successful therapy. In fact, areas of skin laxity without a great deal of muscular attachment seem to be the areas that respond best to tissue tightening devices. Clinicians need to inform all of their patients that although they will likely see an immediate tissue tightening effect, it may be short lived and full clinical results and efficacy may not be seen for the first several months. Patients should also be informed that once results are seen, they will continue to improve through about six months. Long-term clinical data in tissue tightening are lacking, so how long the results will be maintained and whether maintenance therapy will be needed and when will come into play as more data emerge.
What’s New in the Way of Devices
The first tissue tightening device in the United States market was known as Thermage® ThermaCool®. In the past several years, this company and Reliant Technologies merged to form Solta Medical (Hayward, California). The ThermaCool is a monopolar RF device that has the most studied and published clinical trials of all of the tissue tightening devices on the market.
Thermage/Solta has looked at many facets of the tissue tightening business and systematically worked with clinicians to perform single-center and multicenter clinical trials. In its simplest form, this device utilizes monopolar RF energy to deliver heat deep into the dermal tissues—volumetric, deep, dermal heating, which has also been shown to involve the fibrous septae of the fat layer of the skin. In the original clinical trials for this device and in early clinical experience, many clinicians felt that high energies delivered with one to two passes would yield the best clinical results. The treatments were quite painful and many clinicians needed to use sedation with the procedure to make it acceptable to those receiving it. Also, with increasing fluences being used, some adverse effects, such as fat necrosis and atrophic scarring, were noted in some patients. With proper study and analysis, most would now favor that when utilizing these newer device treatment paradigms, which involve lower energies, multiple passes, and utilizing patient feedback on heat sensation and the endpoint of therapy, is perhaps the best approach for this device. A recent clinical review of 5,700 treatment sessions has confirmed this approach with this device. The incidence of continued fat necrosis has also been studied extensively and has virtually disappeared with the new treatment paradigms now in place. Again, patient selection and expectations are crucial.
A newer model, the ThermaCool® NXT (Figure 1), incorporated some of the newer features into the system while making the external system more aesthetically pleasing.[2–13] Several tips and newer hand pieces have become available with this new device (Figure 2). These include tips for the body and eye and a hand piece for cellulite. A new Comfort Plus Technology (CPT) tip is also available, which incorporates massage with RF energy delivery, increasing the speed of the procedure yet making it even more comfortable.
{kind=link}
{kind=link}
Other RF devices also exist in the United States market. The Polaris™ and ReFirme™ from Syneron™ (Yokneam, Israel) (Figure 3) utilize bipolar RF at the ends of laser systems (780–910nm diode for the Polaris and 700–2000nm infrared light for the ReFirme™). Their premise is that by combining light and RF current, less RF energy is needed and that proper collagen denaturation and resultant remodeling will occur to provide the desired effect, predominantly diminution of lines and wrinkles, with some tissue tightening noted. The cooling apparatus is within the handpiece of the device. A major adverse event noted with these RF devices is known as tissue arcing, which can lead to scar formation. This has been noted when the hand piece has not been placed properly on the skin, causing some of the RF energy to not be delivered deep enough into the skin.1 Overall, the procedure is tolerated well by most patients and wrinkle reduction can be achieved.
{kind=link}
Another bipolar RF device is known as the Aluma™ from Lumenis (Santa Clara, California) (Figure 4). It utilizes its bipolar RF energy with an accompanying vacuum apparatus, which takes the tissue into the vacuum and delivers deep dermal energy specifically targeted to the deep dermis. The vacuum diminishes the pain associated with the procedure, which is virtually nonexistent and has been demonstrated in clinical trials.[14] Less energy for an effective treatment is needed, as the vacuum apparatus brings the electrodes closer to the dermal tissue. This device is approved for the treatment of fine lines and wrinkles (Figure 5) but many are finding that it is also useful for tissue tightening in other areas of the body. Although newer, larger treatment tips were developed, this device has disappeared from the US market in recent years. However, it has recently re-emerged in some parts of Asia, with the possibility of being re-introduced into the US market at some point later this year.
{kind=link}
{kind=link}
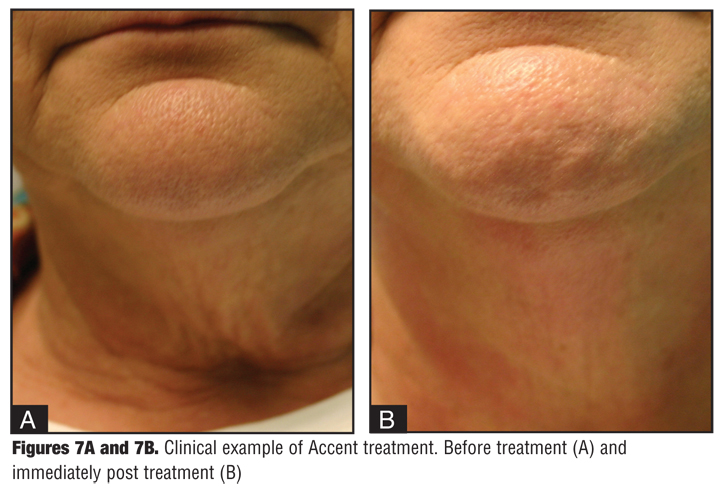
The last of the approved RF devices in the United States is known as the Accent™ made by Alma Lasers™ (Buffalo Grove, Illinois). It utilizes both unipolar and bipolar RF and delivers different depths of RF current to the skin—bipolar for more superficial heating and unipolar for deeper dermal heating. It also utilizes a closed system (i.e., no grounding plate is required) differentiating it from the other monopolar system on the market. Several published clinical trials show its effectiveness in reducing the appearance of cellulite and its effects on tissue tightening.[15–18] The Accent™ XL, an updated version of the device, is currently available (Figure 6 and Figure 7). Several treatment tips have become available for this device, including a UniLarge tip, an eye tip, and a cellulite-massaging tip. A new Pixel RF hand piece has been developed for this device as well and should be available in the United States later in 2010. The Pixel RF uses bipolar RF electrodes placed at the end of roller tips that are moved over the skin for improvement of scars and wrinkles, and tissue tightening.
{kind=link}
{kind=link}
The second type of energy being used in tissue tightening is broadband infrared light, in the range of 800 to 1800nm, depending on the device being utilized. Three such devices are currently available—the Titan® by Cutera® (Brisbane, California), the StarLux® IR by Palomar Medical Technologies (Burlington, Massachusetts), and the SkinTyte™ by Sciton (Palo Alto, California).
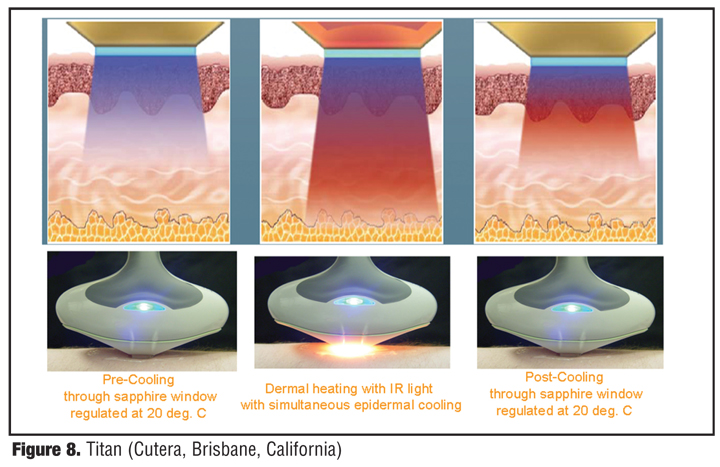
The Titan device was the first of the light-based systems to emerge onto the tissue tightening scene. It utilizes light energy in the range of 1100 to 1800nm, specifically targeting water as its chromophore to achieve its desired effect of collagen denaturation leading to collagen remodeling and tissue tightening. It has a cooling apparatus in the treatment hand piece and requires upwards of six seconds for proper pre- and post-cooling to be achieved (Figure 8). Tissue tightening has been noted as a result, and pain seems to have been addressed after some initial concerns regarding the pain associated with this light source.[19]
{kind=link}
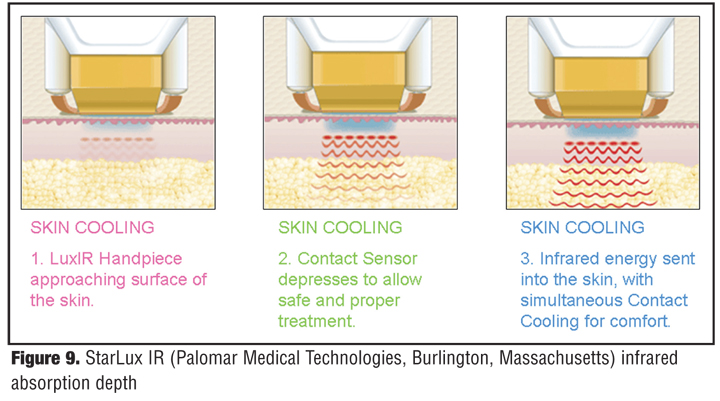
The StarLux® IR delivers fractionated energy through the hand piece of the device, which emits light in the range of 850 to 1350nm to the deep dermis, again targeting water as the principal chromophore (Figure 9) along with its mechanism of action and infrared absorption depth. Several treatments are required with this device for successful collagen remodeling to be achieved.20
{kind=link}
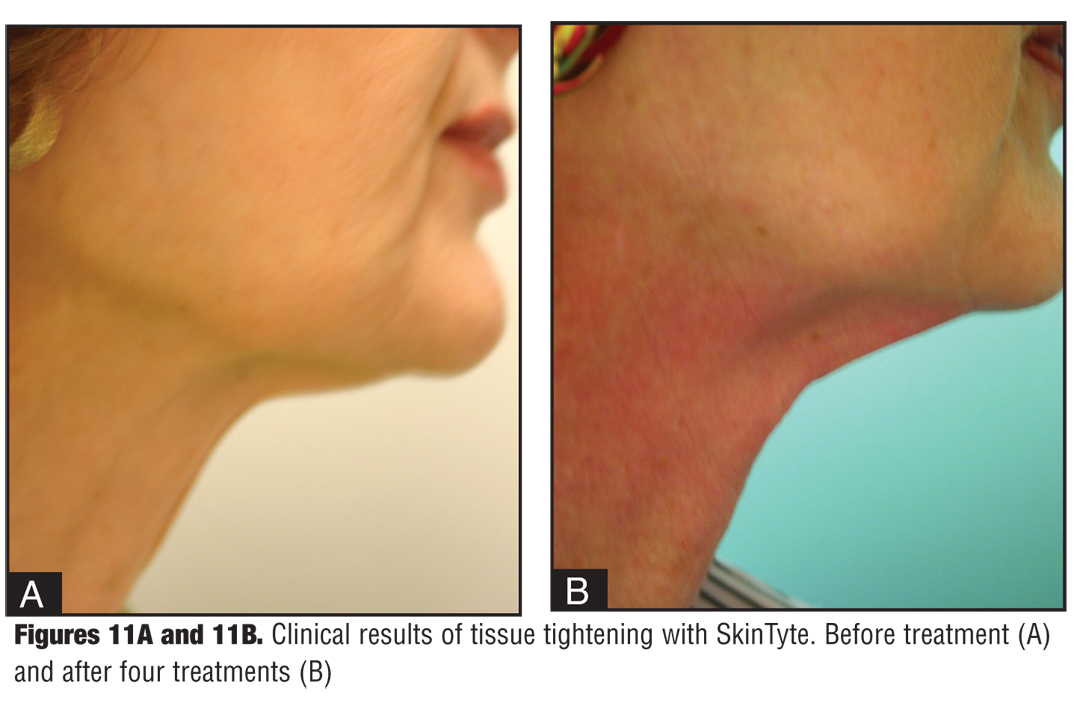
The SkinTyte™ (Figure 10) also utilizes light energy in the range of 800 to 1400nm. It works through a sophisticated cooling mechanism as well, with pre- and post-cooling during the actual treatment. Clinical results of this device show tissue tightening (Figure 11).
{kind=link}
{kind=link}
The next device described is not available in the United States at the time of this writing, but may be available later in 2010. TriPollar, manufactured by Pollagen (Israel) (Figure 12), uses three RF poles placed on the skin, and, through its multi-electrode configuration, allows RF cellulite and skin tightening treatments to occur virtually painlessly. Several clinical studies have shown its effectiveness and we are awaiting United States clinical trials to confirm these results.[21–24]
{kind=link}
Conclusion
Tissue tightening devices have continued to be a major force in the noninvasive skin tightening market. Clinical research studies, although small in most cases, have supported their usefulness, and we must continue to refine our techniques and choose appropriate patients with realistic expectations for optimal results.
References
1. Gold MH. Tissue tightening—a hot topic utilizing deep dermal heating. J Drugs Dermatol. 2007;6(12):1238–1242.
2. Dierickx CC. The role of deep heating for noninvasive skin rejuvenation. Lasers Surg Med. 2006;38:799–807.
3. Fitzpatrick R, Geronemus R, Goldberg D, et al. Multicenter study of noninvasive radiofrequency for periorbital tissue tightening. Lasers Surg Med. 2004;34(3):203–204.
4. Alster TS, Tanzi E. Improvement of neck and cheek laxity with a nonablative radiofrequency device: a lifting experience. Dermatol Surg. 2004;30(4 Pt 1):503–507.
5. Fisher GH, Jacobson LG, Bernstein LJ, et al. Nonablative radiofrequency treatment of facial laxity. Dermatol Surg. 2005;31(9 Pt 2):1237–1241.
6. Ruiz-Esparza J, Gomez JB. The medical face lift: a noninvasive, nonsurgical approach to tissue tightening in facial skin using nonablative radiofrequency. Dermatol Surg. 2003;29(4):325–332.
7. Biesman B, Carruthers J, Bakers S, et al. Monopolar radiofrequency treatment of human eyelids: a prospective, multicenter, efficacy trial. Lasers Surg Med. 2006;38(10):890–898.
8. Jacobson LG, Alexiades-Armenakas M, Bernstein L, et al. Treatment of nasolabial folds and jowls with a noninvasive radiofrequency device. Arch Dermatol. 2003;139(10):1371–1372.
9. Abraham MT, Ross VE. Current concepts in nonablative radiofrequency rejuvenation of the lower face and neck. Facial Plast Surg. 2005;21(1):65–73.
10. Ruiz-Esparza J, Gomez JB. Nonablative radiofrequency for active acne vulgaris: the use of deep dermal heat in the treatment of moderate to severe active acne vulgaris (thermotherapy): a report of 22 patients. Dermatol Surg. 2003;29(4):333–339.
11. Narukar V. Full thickness permanent scars from bulk heating using an infrared light source. Lasers Surg Med. 2006;S18:96.
12. Weiss RA, Weiss MA, Munavalli G, et al. Monopolar radiofrequency facial tightening: a retrospective analysis of efficacy and safety in over 600 treatments. J Drugs Dermatol. 2006;5(8):707–712.
13. Dover JS, Zelickson B, et al. Results of a survey of 5,700 patient monopolar radiofrequency facial skin tightening treatments: assessment of a low-energy multiple-pass technique leading to a clinical end point algorithm. Dermatol Surg. 2007;33(8):900–907.
14. Gold MH, Goldman MP, Rao J, et al. Treatment of wrinkles and elastosis using vacuum-assisted bipolar radiofrequency heating of the dermis. Dermatol Surg. 2007;33:300–309.
15. Emilia del Pino M, Rosado RH, Azuela A, et al. Effect of controlled volumetric tissue heating with radiofrequency on cellulite and the subcutaneous tissue of the buttocks and thighs. J Drugs Dermatol. 2006;5(8):714–722.
16. Goldberg DJ, Fazeli A, Berlin AL. Clinical, laboratory, and MRI analysis of cellulite treatment with a unipolar radiofrequency device. Dermatol Surg. 2008;34:204–209.
17. Mayoral FA. Skin tightening with a combined unipolar and bipolar radiofrequency device. J Drugs Dermatol. 2007;6(2):212–215.
18. Alexiades-Armenakas M, Dover JS, Arndt KA. Unipolar radio frequency treatment to improve the appearance of cellulite. J Cosm Laser Ther. 2008;10:148–153.
19. Goldberg DJ, Hussain M, Fazeli A, et al. Treatment of skin laxity of the lower face and neck in older individuals with a broad-spectrum infrared light device. J Cosmet Laser Ther. 2007;9:35–40.
20. Weiss RA. Prospective clinical trial of a fixed array novel 1540 fractional erbium laser for scars and rhytids. Lasers Surg Med. 2007;S19:15.
21. Manuskiatti W, Boonthaweeyuwat E, Varothai S. Treatment of striae distensae with a TriPollar radiofreqency device: a pilot study. J Dermatolog Treat. 2009;20(6):359–364.
22. Kaplan H, Gat A. Clinical and histopathological results following TriPollar radiofrequency skin treatments. J Cosmet Laser Ther. 2009;11:78–84.
23. Manuskiatti W, Wachirakaphan C, Lektrakul N, et al. J Eur Acad Dermatol Venereol. 2009;23(7):820–827.
24. Boisnic S. An ex-vivo study of the regen TriPollar device using an experimental human skin model. Les Nouvelles Dermatologiques. 2008;28:331–332. (English translation).