Sarah Otto, CNP; Matthew J. Zirwas, MD
Dr. Zirwas is Assistant Professor of Dermatology, The Ohio State University, Columbus, Ohio. Ms. Otto is from the Division of Dermatology, The Ohio State University, Columbus, Ohio. The authors report no relevant conflicts of interest.
Case
An 81-year-old man presented with a recalcitrant case of cheilitis that had been ongoing for seven months (Figure 1). His dermatitis was extremely itchy and painful. It was predominantly right sided, but extended around his mouth and even on to his lip mucosa. The lower vermillion border was obscured by the eruption. His lips were fissured, intensely dry, and slightly swollen. His oral cavity was also noted to be mildly erythematous. Acrodermatitis enteropathica was originally in the differential diagnosis, but ruled out after obtaining a normal zinc level.
{kind=link}
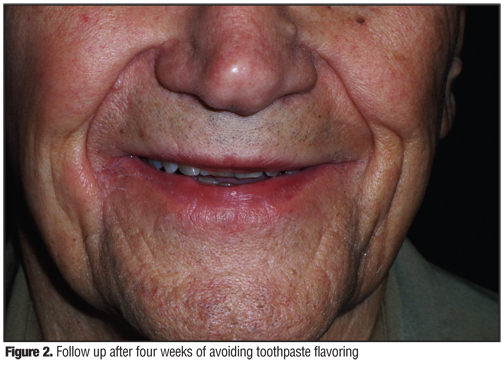
Allergic contact dermatitis (ACD) was then considered and the patient was referred to The Ohio State University Contact and Occupational Dermatitis Center in Columbus, Ohio. He underwent patch testing and was found to have a 1+ reaction to fragrance mix 1 and cinnamic alcohol. He also had a 2+ reaction to his own Arm & Hammer Advance White Fresh Mint Toothpaste. The patient was switched to Tom’s of Maine Natural Orange and Mango Toothpaste and LISTERINE Antiseptic Mouthwash, Natural Citrus. Upon seeing him at his four-week follow-up visit, his rash had almost completely resolved (Figure 2).
{kind=link}
Discussion
This case is of interest for several reasons. Although allergy to fragrance or flavorings is common, in the majority of cases we have seen, patients with cheilitis and fragrance allergy have not improved following avoidance of flavorings. However, in this case, the cheilitis resolved with avoidance of mint- and cinnamon-related toothpaste flavors, confirming that the toothpaste flavoring was the relevant exposure leading to the cheilitis.
Clinical factors the authors have noted in their experience that increase the likelihood of finding a relevant contact allergen to explain cheilitis include asymmetrical presentation, with one side being persistently more involved than the other and an obscured vermillion border, indicating that the eruption is spreading beyond the lip and onto the skin. This patient demonstrated both of these findings.
Finally, the patch test reactions to fragrance mix 1 and cinnamic alcohol were both 1+ reactions. The authors consider 1+ reactions to be positive reactions and counsel patients to avoid allergens with this reaction, based primarily on the assessment of relevance. It is generally accepted that positive reactions, whether 1+ (palpable, but does not fill patch-test site), 2+ (palpable and fills patch site), or 3+ (reaction extends beyond patch-test site or vesicles are present), are considered evidence of allergy to the tested substance.
Toothpaste is a commonly used personal care product. Americans spend an average of 38.5 total days brushing their teeth over a lifetime, according to the Academy of Periodontology.[1] It is used primarily to improve dental health and prevent tooth decay. On average, consumers spend $5.2 billion dollars on oral hygiene annually.[2] The main categories of substances used in the formulation of toothpaste are abrasives, detergents, binding agents, humectants, preservatives, coloring agents, antiseptics, fluoride salts, and flavorings.[3] Modern toothpastes were developed in the 1800’s and flavoring was one of the first ingredients to be added.[4] Flavoring not only makes the toothpaste more enjoyable to use, but it also freshens breath. However, in the majority of cases described, the responsibility for toothpaste allergic contact cheilitis has lain with the flavoring substances, while other components of the toothpastes have more rarely been found to be the cause.[3]
Patch testing for toothpaste allergy can be challenging. Many of the relevant allergens can also be irritants, which may lead to false-positive results. This is especially true when testing particular toothpastes directly. Some advise conducting the patch test with a diluted form of the product to avoid false-positive results from the irritating ingredients, such as detergents and abrasives.[3] However, it is also difficult to avoid false-negative results from dilutions.
The most common flavorings that are frequently responsible for toothpaste allergies are cinnamal, spearmint, peppermint, carvone, and anethole.[3] Because most toothpaste is flavored with either a variation of mint or cinnamon, it can be challenging to find toothpaste free of these flavors for those who have an allergy. The authors sought to systematically evaluate the potentially allergenic ingredients currently used in toothpaste that are readily available in the United States. This information should be helpful to clinicians who detect allergy to substances, especially flavors that may be present in most toothpaste purchased by their patients.
Methods
The authors used a recently published database of all toothpastes that are commercially available at Walgreens pharmacies (operated by Walgreen Co., Deerfield, Illinois).[5] For each toothpaste, this database lists all allergens from the North American Contact Dermatitis Group (NACDG) screening panel that are present in the product. The database was created by a dermatologist with specific expertise in ACD. Using this database, the authors entered the name of each toothpaste and the allergens in that toothpaste into a Microsoft Excel spreadsheet (Microsoft Corporation, Redmond, Washington). Using filters, the authors then determined the number of toothpastes that contain each allergen.
Results
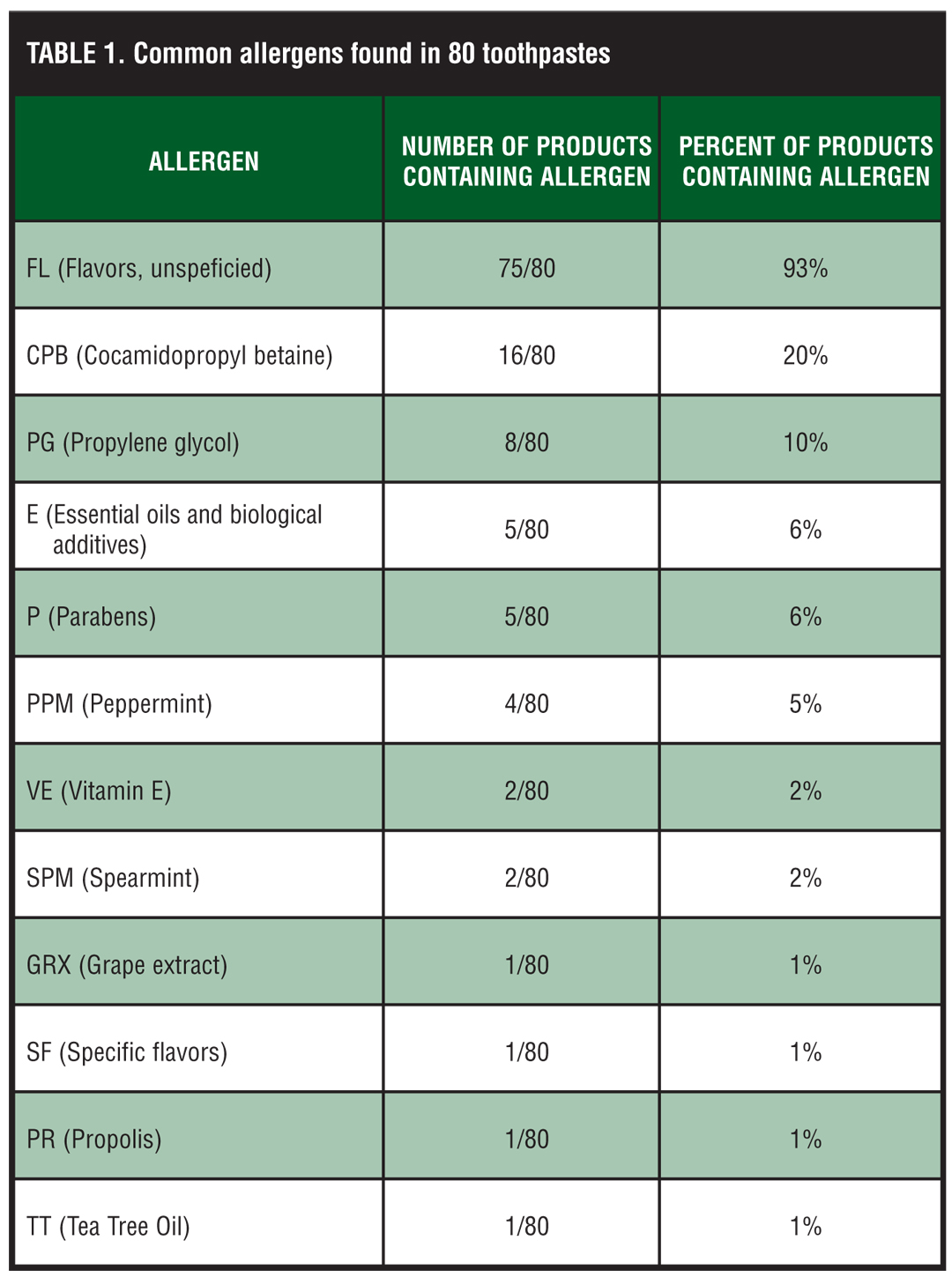
The database included 80 types of toothpaste, 76 of which contained unspecified flavoring, which makes flavoring the most commonly present allergen (Table 1). There were only four toothpastes that did not contain flavoring of any kind. However, there were also four toothpastes that did contain alternative flavors, but did not contain mint, spearmint, peppermint, or cinnamon flavoring, which are the most common flavor allergies. Therefore, if a patient’s allergy can be narrowed down specifically to a mint or cinnamon favor allergy, then he or she would be able to use alternative flavoring, such as grape, strawberry, orange-mango, or apricot.
{kind=link}
The second most commonly present allergen in toothpaste was cocamidopropyl betaine (CAPB). Even with this being the second most common allergen, only 16 of the 80 toothpastes actually contained this surfactant. The third most common allergen was propylene glycol, a water-soluble vehicle. Eight of 80 toothpastes contained this allergen.
Essential oils and biological additives were the fifth most common allergen with 5 of 80 toothpastes containing essential oils. This ingredient is related to flavoring and all of the toothpastes that contained essential oils in the database also contained flavoring. Therefore, if a flavor allergy was suspected it would be prudent to also avoid toothpastes containing essential oils. In addition, 4 of the 80 toothpastes contained peppermint (PPM) flavoring specifically and 2 of the 80 toothpastes contained spearmint flavoring (SPM). There was also one product that contained specific flavors, which were peppermint and spearmint flavors only.
Parabens were also present in 5 of the 80 toothpastes. They are commonly used as preservatives in personal care products. Therefore, in addition to essential oils, parabens are the fifth most common allergen overall. Vitamin E (tocopherol) was the sixth most common allergen, being present in 2 of the 80 toothpastes.
Grape extract, an alternative flavoring, was used in one toothpaste. Tea tree oil was also used in one toothpaste and propolis was used in one toothpaste. Propolis is a resin that was used in a skin-saving, flavor-free, hypoallergenic toothpaste. This would be a good flavor-free toothpaste option, but should be avoided if a propolis allergy is suspected.
Discussion
The most common allergen occurring in the authors’ search was flavoring, which was present in 95 percent of the toothpaste contained in the Walgreens database. Flavoring is added to toothpaste not only to make toothpaste more enjoyable to use, but also to freshen breath. Therefore, the obvious toothpaste flavor choices are a variation or combination of cinnamon and mint. According to a recent multicenter study of allergic contact cheilitis from toothpaste, the majority of cases responsible for toothpaste allergies were flavoring, and particularly important were those relating to derivatives extracted from the main varieties of mint, such as spearmint, peppermint, menthol, and carvone—widely used in toothpastes to produce a sensation of freshness.[3]
Toothpaste is a personal care product that is commonly used by consumers starting at a very young age. This is one exposure through which sensitivity to flavors can develop.[6] Not only are consumers exposed to flavoring allergens through toothpaste, but also through chewing gum, ice cream, soft drinks, candies, and mouthwash.[7] These common exposures heighten the chance of becoming allergic to common toothpaste flavors.
CAPB was the second most common ingredient listed in the Walgreens database. CAPB is found in a variety of rinse-off products, including shampoos, bath products, hair-styling products, contact lens solutions, acne treatments and toothpaste.[8] It is a surfactant used as a lathering agent or foaming agent, which is why it is often added to toothpaste. It also has some antimicrobial effects and its use has increased because of its nontoxic, low irritancy features.[9] Because it was considered less irritating, its use increased and the variety of products it was used in also expanded. Therefore, the increase in contact-sensitization prevalence is thought to be due to more frequent use as CAPB is substituted for anionic surfactants (such as sodium lauryl sulfate) and cationic surfactants (such as polyoxyethylene dihydroxypropyl linoleaminium chloride), which are more irritating.10 Several studies have demonstrated that the real sensitizers may in fact be contaminant chemicals dimethylaminopropylamine (DMAPA) and amidoamine (AA), rather than CAPB itself. The issue of the real sensitizer has been a matter of controversy.[10] Therefore, the NACDG has switched to routinely testing patients with both CAPB and AA.[11]
Propylene glycol was the third most common allergen. It works as a solvent to mix relatively insoluble ingredients and acts as a preservative.[5] Of 1,494 patch-tested individuals who had a scattered, generalized distribution of dermatitis, six percent were found to be sensitized to propylene glycol.[12] Skin exposure to propylene glycol most commonly occurs through contact with cosmetics or topical medicaments.[13] When patch testing for propylene glycol, it is difficult to distinguish between immunological and irritative responses. Several patch-test studies in different test populations with propylene glycol in concentrations between 2 and 30% revealed a frequency of positive reactions in a range of 0.1 to 3.8% of the patients tested.[13] It has been suggested that propylene glycol be tested with serial dilutions, repeat open-application tests, and/or oral challenge tests, to help determine clinical significance.[14] Propylene glycol and toothpaste both have irritant potential, which can make interpretation challenging.
Essential oils were the fourth most common allergen in the toothpaste products. They are aromatic substances that are extracted from many different plants and a small number of animals or synthesized from coal and petrolatum.[15] Methods of essential oil extraction include distillation, maceration, solvent and carbon dioxide extraction, expression, and enfleurage.[16] There are many components to essential oils and the ingredients may vary by batch, heat, season, moisture, and light, which is why it is difficult to standardize these allergens.[9] Tea tree oil was utilized specifically in one of the toothpastes in our database. A study of more than 2,000 patch-tested individuals found that tea tree oil, the most common essential oil allergen, elicited a positive reaction in 1.8 percent of these patients.[17] There are many essential oils, but only the most prevalent ones known to cause contact dermatitis, such as ylang ylang, tea tree oil, compositae mix, propolis, and colophony, are included in most patch-testing trays.[5] It is important to test and be aware of essential oil allergies, especially when recommending alternative-flavored toothpastes, which may use essential oils to replace common flavorings.
Parabens were found in only six of the toothpastes analyzed in the Walgreens database. Parabens are commonly used preservatives in many over-the-counter products. Each ester has different antimicrobial properties, but they generally all tend to be more effective against fungi than bacteria and therefore commonly used with other preservatives to achieve greater activity against bacteria.[18] Parabens are found worldwide in creams, pastes, beauty products, glues, fats, and oils.[19] Methyl and ethyl parabens are the most frequently used parabens and, with the exception of water, the most commonly used ingredients in cosmetic preparations.[19] Parabens are popular preservatives because they are inexpensive, colorless, odorless, and nontoxic.[19] The NACDG reported that 0.6% of patients reacted to the paraben mix according to their most recent data.[18] The prevalence of ACD from parabens is low; in most studies, it ranges from 0 to 4.2%.[19] ACD has most commonly been reported when paraben-containing products are used on damaged skin.[20] However, in normal use, the paraben preservatives are very rare contact sensitizers and set the standard for relative safety that new preservatives will have difficulty matching.[21]
Propolis is composed of beeswax, resin and vegetable balsam, essential and aromatic oils, pollen, and other substances.[22] It has antimycotic, bacteriostatic, astringent, coleric, spasmolytic, anti-inflammatory, and anesthetic properties. It is widely used in powders, lotions, ointments, solutions, creams, toothpaste, and chewing gum.[22] Propolis is increasingly being recognized as an important allergen, with a rising prevalence from 0.5 to 1.4% over the past 10 years.[23] The ingestion of propolis can also have deleterious effects resulting in allergic contact cheilitis, stomatitis, perioral eczema, labial edema, oral pain, and dyspnea.[24] These reactions have been described after patients have consumed various propolis products, such as tablets, toothpaste, mouthwash, and lozengers.[25] The generally recommended patch-test concentration is 10%.[24] With an increase in consumers purchasing natural products the exposure to propolis will continue to rise and patch testing for this allergen will become even more essential.
Conclusion
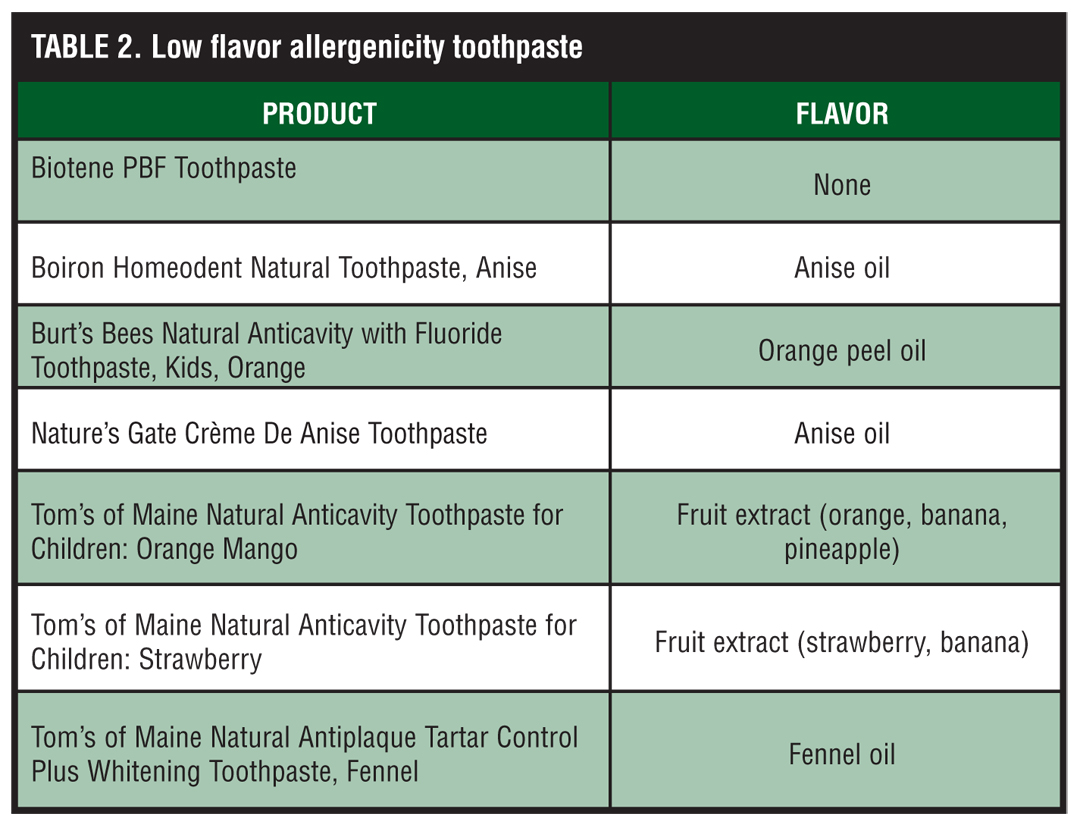
Toothpaste contains many potential allergens that are commonly the cause of allergic contact cheilitis. Many toothpaste ingredients have the potential to cause either an irritant or allergic reaction, making it essential for healthcare providers to be well versed in toothpaste ingredients. The authors’ search of the Walgreens database found flavoring to be the most common allergen, but cocamidopropyl betaine, propoylene glycol, essential oils, parabens, and propolis are also commonly used potential allergens in toothpaste. It can be difficult to determine the actual cause of the allergy, even if flavoring is suspected. Many healthcare providers may want to empirically recommend alternative-flavored toothpaste, but even this can be challenging. Almost all of the mainstream toothpaste brands flavor their toothpaste with either a variation of mint or cinnamon. However, there are a few products that use either no flavoring or alternative flavoring, which can be useful for such patients (Table 2).
{kind=link}
In conclusion, cheilitis can be a challenging issue for healthcare providers and further work-up including advanced patch testing and or a biopsy may be needed.
References
1. American Academy of Periodontology. Consumer Survey. www.perio.org/consumer/cosmetic_data.htm. Accessed November 23, 2009.
2. Nielsen A. (2008) Delivering consumer clarity. Consumer Insight. http://en-usnielsen.com/main/ insight/consmer_insight. Accessed November 23, 2009.
3. Francalaci S, Sertoli A, Giorgini S, et al. Muticentre study of allergic contact cheilitis from toothpastes. Contact Dermatitis. 2000;43:216–222.
4. Jardim J, Alves L, Martz M. The history and global market of oral home-care products. Brazilian Oral Research. 2009;23(1):17–22.
5. Scheman A, Jacob S, Zirwas M, et al. Contact allergy: alternatives for the 2007 North American Contact Dermatitis Group (NACDG) standard screening tray. Dis Mon. 2008;54(1-2):7–156.
6. Tremblay S, Avon S. Contact allergy to cinnamon: case report. Journal of the Canadian Dental Association. 2008;74(5):445–448.
7. Magnusson B, Wilkinson DS. Cinnamic aldehyde in toothpaste. 1. Clinical aspects and patch tests. Contact Dermatitis. 1975;1(2):70–76.
8. Mowad CM. Cocamidoproproply betaine allergy. Am J Contact Dermatol. 2001;1:223–224.
9. Mowad CM. Allergens of new and emerging significance. Dermatol Nurs. 2006;18(6):545–548.
10. Jacob SE, Amini, S. Cocamidopropyl betaine. Dermatitis. 2008;19(3)157–160.
11. Fowler JF, Zug KM, Taylor JS, et al. Allergy to cocamidopropyl betaine and amidoamine in North America. Dermatitis. 2004;15:5–6.
12. Zug KA, Rietschel RL, Warshaw EM, et al. The value of patch testing patients with a scattered generalized distribution of dermatitis: retrospective cross-sectional analyses of North American Contact Dermatitis Group data, 2001 to 2004. J Am Acad Dermatol. 2008;59(3):426–431.
13. Lessmann H, Schnuch A, Geier J, et al. Skin-sensitizing and irritant properties of propylene glycol. Contact Dermatitis. 2005;53:247–259.
14. Funk JO, Maibach HI. Propylene glycol dermatitis: re-evaluation of an old problem. Contact Dermatitis. 1994;31:236–241.
15. Scheinman PL. Allergic contact dermatitis to fragrance: a review. Am J Contact Dermat. 1996:7:65–76.
16. Trattne A, David, M, Lazrov A. Occupational contact dermatitis due to essential oils. Contact Dermatitis. 2008;58:282–284.
17. Rutherford T, Nixon R, Tam M, et al. Allergy to teat tree oil: retrospective review of 41 cases with positive patch tests over 4.5 years. Australas J Dermatol. 2007;48(2):83–87.
18. Coloe J, Zirwas M. Allergens in corticosteroid vehicles. Dermatitis. 2008;19(1):38–42.
19. Cashman A, Warshaw E. Parabens: a review of epidemiology, structure, allergenicity, and hormonal properties. Dermatitis. 2005;16(2):57–66.
20. Fisher AA. Paraben dermatitis due to a new medicated bandage: the “paraben paradox.” Contact Dermatitis. 1979;5:273–274.
21. Basketter D, McFadden J, Evans P, et al. Identification and classification of skin sensitizers: identifying false positives and false negatives. Contact Dermatitis. 2006;55;268–273.
22. Burdock GA. Review of the biological properties and toxicity of bee propolis. Food and Chemical Toxicology. 1998:36:347–363.
23. Langan SM, English JS. Occupational contact dermatitis from propolis in a dental technician. Contact Dermatitis. 2007;56;43–57.
24. Walgrave SE, Warshaw EM, Glesne LA. Allergic contact dermatitis from propolis. Dermatitis. 2005;16(4);209–215.
25. Hsu CU, Chiang WC, Weng TI, et al. Laryngeal edema and anaphylactic shock after topical propolis use for acute pharyngitis. Am J Emerg Med. 2004;22;432–433.