Emmy M. Graber, MD; Jeffrey S. Dover, MD, FRCPC; Kenneth A. Arndt, MD
Emmy M. Graber, MD is Assistant Professor of Dermatology, Boston University, Boston, Massachusetts; Jeffrey S. Dover, MD, FRCPC is from Skin Care Physicians, Chestnut Hill, Massachusetts; Associate Clinical Professor of Dermatology, Yale University, New Haven, Connecticut; Adjunct Professor of Medicine (Dermatology), Dartmouth Medical School, Hanover, New Hampshire; Kenneth A. Arndt, MD is from Skin Care Physicians, Chestnut Hill, Massachusetts; Adjunct Professor of Surgery, Dartmouth Medical School, Hanover, New Hampshire; Adjunct Professor of Dermatology, Brown University, Providence, Rhode Island; Clinical Professor of Dermatology, Emeritus, Harvard Medical School, Boston, Massachusetts
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Two patients under the authors’ care developed facial herpes zoster that erupted soon after cosmetic treatment with botulinum toxin type A (BTA). Both patients received typical doses of BTA in the glabella, forehead, and lateral periorbital areas. Within one week after treatment, each patient began experiencing symptoms of herpes zoster in one of the dermatomes supplied by the trigeminal nerve. Since the resolution of the herpes zoster, both patients have gone on to receive further treatments of BTA with prophylactic oral antivirals without sequelae. (J Clin Aesthet Dermatol. 2011;4(10):49–51.)
Case 1
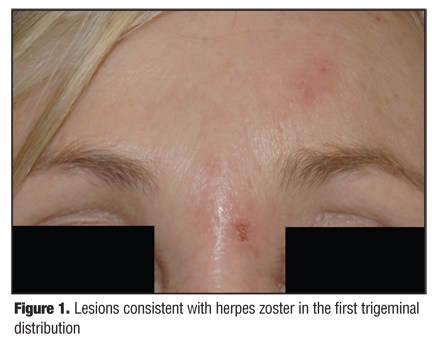
A 55-year-old woman had received at least eight treatments with BTA for lines of facial expression prior to her treatment in March 2008. At that time, she received her usual injections at three sites—glabella, forehead, and lateral periorbital areas. A total of 50 units were injected. She had no prior history of herpes zoster and was not immunosuppressed. Her only medication was citalopram 20mg by mouth once per day. After her treatment in March 2008, she developed swelling, pain, and pruritus of the left forehead and glabella region. She was seen seven days after her treatment and had poorly demarcated erythema and edema with superficial erosions of the left forehead and glabella (Figure 1). The erosions were not at the exact sites where the BTA injections were placed. A diagnosis of herpes zoster in the first branch of the left trigeminal nerve was made and she was treated with valacyclovir hydrochloride 1g three times daily for 10 days. One week after her presentation with herpes zoster, she was seen again, and her signs and symptoms had almost completely resolved. She received repeat treatment with BTA in September 2008 and concomitantly received oral antivirals without recurrence of herpes zoster.
{kind=link}
Case 2
A 48-year-old woman had no prior treatment with BTA until April of 2007. At that time, she was treated with BTA in the glabella, forehead, and lateral periorbital areas. She had no prior history of herpes zoster or immuno-suppression and was not on any medications. Six days following treatment, she noted paresthesias of the right external ear. This progressed over that day to include right ear “throbbing” and a “constant headache” on the right side of the head. Seven days after injection, she developed vesicles on her right forehead and in the glabella area. One day later, she developed right eye swelling, but had no changes in her visual acuity. She was diagnosed with “sinusitis” and a “bacterial skin infection,” according to the patient. Ten days after her treatment with BTA, she described having “horrendous right-sided head pain and itching.” At this point, her right eye was swollen closed and she presented to a local emergency room where several physicians including two opthalmologists evaluated her. She was diagnosed with herpes zoster. The next day, she followed up with another ophthalmologist and a dermatologist who both confirmed the diagnosis of herpes zoster of the first trigeminal dermatome. She was treated with oral valacyclovir and oral pain medication. Her skin lesions lasted for two weeks, but her head pain persisted for months, then eventually subsided.
In June 2009, she was again treated with BTA in the glabella, forehead, and lateral periorbital areas for cosmetic purposes. Given her history, she also took famciclovir 500mg three times per day for seven days beginning on the day of treatment. The BTA treatment was uneventful.
Discussion
Herpes zoster is caused by reactivation of varicella zoster virus, a member of the herpes virus family. Initial infection with the varicella zoster virus presents with disseminated vesicles (commonly known as chickenpox). Following this primary infection, the varicella zoster virus lies dormant in the dorsal root nerve ganglion. The virus can reactivate at a later time, appearing as vesicles in a unilateral dermatomal distribution. This eruption is preceded by a prodome that may consist of pain, pruritus, dysasthesias, or generalized malaise. When herpes zoster occurs on the face, it may be accompanied by headache, earache, vision changes, or dysgeusia.[1]
Herpes zoster is more common in immunosuppressed patients and in older patients, with an increased occurrence starting at ages 55 to 60.[2] The exact immunological mechanism in which reactivation occurs is unknown, although it is believed to be due to a decline in varicella zoster virus specific cell mediated immune responses.[3] Herpes zoster is not uncommonly seen following major surgeries when the immune system is stressed. Following minor procedures, it is not expected that the immune system will be taxed enough to cause reactivation of the varicella zoster virus, but mechanical trauma and local inflammation may play a role in reactivating the varicella zoster virus. There are anecdotal reports in the literature of herpes zoster outbreaks occurring in a dermatome at or near a recent procedure. One author describes herpes zoster following an axillary nerve block.[4] Others have described herpes zoster following intra-articular corticosteroid injection[5] and after cryosurgery.[6] The authors describe two patients who developed herpes zoster following treatment with BTA. The mechanism by which minor localized procedures triggers herpes zoster is unknown.
Repeated outbreaks of herpes zoster in immuno-competent patients is uncommon. However, the authors prophylactically treated their patients with oral antivirals at subsequent treatments to prevent a recurrence of herpes zoster. Both of the patients had retreatment with BTA in the same anatomic areas without recurrence of herpes zoster. Therefore, it is plausible that these two cases occurred by mere temporal association.
The most common consequence of herpes zoster is postherpetic neuralgia, which is defined as pain persisting 120 days after disease onset.[7] The incidence and duration of postherpetic neuralgia directly correlates with patient age. It has been estimated that 13 to 40 percent of patients older than 60 still have postherpetic neuralgia six months after their outbreak.[8,9] Other less common complications of herpes zoster include encephalitis, myelitis, cranial nerve palsies, peripheral nerve palsies, and vision loss.[10] It is important that herpes zoster be treated promptly so as to lessen the duration and severity of the outbreak and also to lessen the complications.
Because of the pain and potential complications of herpes zoster, it is important that the clinician be astute to its presentation. This is especially important in an older patient who is more at risk for herpes zoster. The patients described in these cases bring to light the possibility that BTA injections may act as a trigger to reactivate the varicella zoster virus. However, these two cases do not prove an association between botulinum toxin type A injections and herpes zoster. These cases raise attention so that the physician will have a heightened index of suspicion of pain after botulinum toxin injection. Particularly severe, neural pain (paroxysmal and sharp) developing after injection should cause alarm for impending herpes zoster. Any patient complaints of prodromal symptoms or a cutaneous eruption after injection with BTA should raise suspicion for herpes zoster. Since herpes zoster reactivation appears to be very uncommon after BTA treatment of the upper face, the authors do not routinely use, nor recommend, antiviral therapy as prophylaxis in their patients undergoing BTA treatments.
References
1. Wareham DW, Breuer J, Wareham DW, Breuer J. Herpes zoster. BMJ. 2007;334(7605):1211–1215.
2. Choo PW, Donahue JG, Manson JE, Platt R. The epidemiology of varicella and its complications. J Infect Dis. 1995;172(3): 706–712.
3. Arvin AM. Humoral and cellular immunity to varicella-zoster virus: an overview. J Infect Dis. 2008;197(Suppl 2):S58–S60.
4. Percival NJ. Shingles following axillary nerve block. A case report. J Hand Surg [Br]. 1986;11(1):115–116.
5. Fernandes NF, Malliah R, Stitik TP, et al. Herpes zoster following intra-articular corticosteroid injection. Acta Dermatovenerol. 2009;18(1):28–30.
6. Lee MR, Ryman W. Herpes zoster following cryosurgery. Australas J Dermatol. 2005 2005;46:42–43.
7. Whitley RJ. A 70-year-old woman with shingles. JAMA. 2009;302(1):73–80.
8. Bowsher D. The effects of pre-emptive treatment of postherpetic neuralgia with amitriptyline: a randomized, double-blind, placebo-controlled trial. J Pain Symptom Manage. 1997;13(6):327–331.
9. McKendrick MW, McGill JI, Wood MJ. Lack of effect of acyclovir on postherpetic neuralgia. BMJ. 1989;298(6671):431.
10. Gilden DH, Kleinschmidt-DeMasters BK, LaGuardia JJ, Mahalingam R, Cohrs RJ. Neurologic complications of the reactivation of varicella-zoster virus [see comment]. [Erratum appears in N Engl J Med. 2000;342(14):1063]. N Engl J Med. 2000;342(9):635–645.