Michael H. Gold, MD; Judy Y. Hu, MD; Julie A. Biron; bMargarita Yatskayer; Amanda Dahl; Christian Oresajo
Michael H. Gold, MD; Judy Y. Hu, MD; Julie A. Biron are from Tennessee Clinical Research Center, Nashville, Tennessee. Margarita Yatskayer; Amanda Dahl; and Christian Oresajo are from L’Oreal Recherche, Clark, New Jersey
Disclosure: The authors report no relevant conflicts of interest. This study was funded by L’Oreal USA Products, Clark, New Jersey.
Abstract
Objective: All-trans retinoic acid is a well-established topical treatment of photodamaged skin. This study assessed the tolerance and efficacy of all-trans retinoic acid after full-face treatment with a chemical peel. Design: This was a split-face, randomized study. One side of each face was treated with peel and the other side with peel and all-trans retinoic acid (3%). Four treatments were given during the 10-week study period. Setting: Physician office. Participants: Fifteen female subjects 39 to 55 years of age. Measurements: Results were evaluated at Baseline; Weeks 4, 7, and 10; and at a 13-week follow-up visit by dermal grading of visual symptoms of irritation, subjective experiences of irritation, clinical grading of skin condition, and self-assessment questionnaires. Results: Both peel and peel plus all-trans retinoic acid treatments achieved significant improvement in fine lines, radiance, roughness, skin tone clarity, skin tone evenness, and hyperpigmentation appearance. Improvement in wrinkles and firmness was not observed in the peel plus all-trans retinoic acid arm, while pore appearance failed to improve in either treatment arm. Improvement in overall facial appearance was greater in the peel alone arm. Peel alone and the addition of all-trans retinoic acid did not cause dryness, edema, or peeling, and the frequency of peel-induced erythema did not increase with the addition of all-trans retinoic acid. Subject-perceived improvements with the peel treatment did not differ significantly from subject-perceived improvements of the peel plus all-trans retinoic acid treatment. Adverse events requiring intervention or discontinuing treatment were not observed in either treatment arm. Conclusion: The addition of all-trans retinoic acid after peel treatment does not significantly enhance peel-induced improvement in photoaging parameters, peel-induced adverse effects, and subject-perceived improvements.
(J Clin Aesthet Dermatol. 2011;4(10):40–48.)
Patients with aged skin present with one or more of the following: wrinkles, fine lines, hyperpigmentation, loss of radiance, smoothness, firmness, skin tone clarity and evenness, and alterations in pore appearance. They may also present with spider veins (telangiectasias). These manifestations are due to the natural aging process and exposure to the sun (photodamage). They are commonly treated by skin resurfacing procedures, such as chemical peeling, dermabrasion, and exposure to laser radiation.
As a facial rejuvenation procedure, chemical peels are popular with patients and inexpensive for physicians.[1] Superficial lesions are removed and skin texture is improved by wounding the epidermis and dermis with a chemical exfoliant known to cause destruction and/or inflammation of the skin in a controlled manner. Extensive photodamage may call for stronger peeling agents and repeat treatments to obtain acceptable improvement.[2] Chemical peels are classified as superficial, medium, and deep.
Alpha hydroxyl acids (AHAs), such as glycolic acid, lactic acid, malic acid, and pyruvic acid, are among the most widely used superficial peeling agents. Intermediate concentrations (25%) increase skin thickness, thus improving skin surface irregularities, minor wrinkles, and dyschromias,[3] and with less irritation than tretinoin (all-trans retinoic acid, RA). AHAs, especially glycolic acid, are ingredients of a wide variety of skin care products including moisturizers and commonly used chemical peeling solutions.[4] For example, topical glycolic acid (8%) and lactic acid (8%) help to improve signs of chronic cutaneous photodamage.[5] Higher concentrations (70%) of glycolic acid have been used as a short-contact peel for the treatment of photodamage.[4]
RA is a topical form of vitamin A used to treat acne and to improve the appearance of fine wrinkles, hyperpigmentation, and roughness of facial skin. The potential use of topical RA for the treatment of photodamage was reported by Cordero[6] and Kligman et al.[7,8] Subsequent studies showed conclusively that RA improves the manifestations of photoaging in human skin, that clinical improvement was secondary to RA-induced skin irritation,[9] and that maximum improvement could be achieved with RA concentrations low enough to minimize retinoid dermatitis.[8]
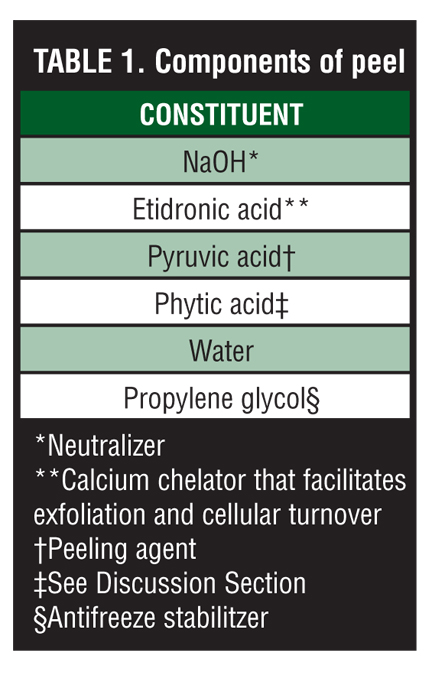
In two uncontrolled studies,[10,11] Kligman reported that combining topical RA and glycolic acid appeared to improve photodamaged skin and acne more than either one alone. Weiss and Shavin[12] showed that RA could be used in combination with glycolic acid solution to reduce the signs of acne vulgaris in human skin. Kim et al[13] reported that pretreatment of guinea pig skin with RA prolonged the effects of a trichloroacetic acid (TCA) peel and enhanced wound healing. This 13-week study evaluates the tolerance and efficacy of RA given after full-face treatment with a peel with the ingredients shown in Table 1.
{kind=link}
MATERIALS AND METHODS
Subjects. This study included 15 healthy female subjects 39 to 55 years of age (47.1±4.8, mean±SD) with Fitzpatrick skin types II to IV and photodamaged skin. Subjects had mild-to-moderate hyperpigmentation as well as fine lines and wrinkles on both sides of the face, had no dermatological disorders that would interfere with the test results or increase risk of adverse reaction, and were willing to avoid extended periods of sun exposure for the duration of the study (including artificial tanning). They were instructed to discontinue use of any other facial cleanser, facial moisturizers, and sunscreens, and to not introduce cosmetic or toiletry products during the study. Subjects were also instructed to arrive at the testing facility for each scheduled clinical visit free of all facial makeup, skin care products, or both, and to apply no other topical products to the face until the study visit had been completed.
Exclusion criteria included pregnancy, nursing, self-perceived sensitive skin, and the presence of conditions that would interfere with the evaluation of the test materials. Recipients of sympathomimetics, antihistamines, vasoconstrictors, nonsteroidal anti-inflammatory agents, immunosuppressants, antibiotics, and corticosteroids within one week before the study began were also excluded. Allergies to soap, cosmetic and toiletry products, topical medications, sunscreens, or RA; having received a facial peel or laser treatment or any cosmetic procedure (e.g., botulinum toxin A) within one month preceding study initiation; current or past use of isotretinoin or similar product; and use of waxing product, tanning product, or tanning bed within one week before initiation of the study; and receiving chemotherapy or radiation treatment were also grounds for exclusion. All subjects provided signed informed consent forms. The study was approved by Independent Investigational Review Board, Plantation, Florida.
Study protocol. The study began in July 2009 and was completed in November 2009. One side of each face was treated with peel and the other side with peel followed by RA (3%). A computer-generated randomization code determined the test material application (e.g., which side of the face received peel and which side received peel + RA). A board-certified dermatol-ogist or his or her designee performed a total of four peel treatments over a 10-week period. Investigators, designees, and subjects were blinded as to treat-ment received by each side of the face and the forearms.
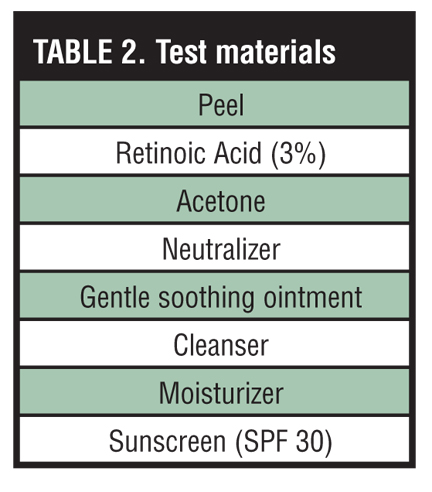
Approximately one week before the first peel treatment, each subject was given an “open” patch test on the volar surface of both forearms to determine potential sensitivity to test materials (Table 2). The RA treatment was high (3%) because treatment was given once every three weeks rather than daily. Objective and subjective tolerances were evaluated 30 to 60 minutes, 24 hours, and one week later. Results were evaluated by clinical grading of facial skin attributes, visual symptoms of irritation, subjective experiences of irritation, and self-assessment questionnaires at designated study intervals.
{kind=link}
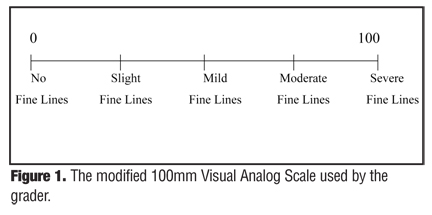
Clinical grading. Facial fine lines, wrinkles, radiance, skin roughness, skin tone (evenness), skin tone (clarity), skin firmness, and pore appearance of the right and left sides of the face were visually examined by an expert grader at specified study intervals. The grader assessed each facial parameter using a modified 100mm Visual Analog Scale (VAS) (Figure 1).
{kind=link}
The evaluator selected a location on the VAS that corresponded with the perception of the subject’s skin in relation to the labeled vertical positions on the scale. The distance between the mark recorded and the left origin of the line was subsequently measured in millimeters to allow for assignment of a numerical score for the extent and/or severity of the evaluated parameter.
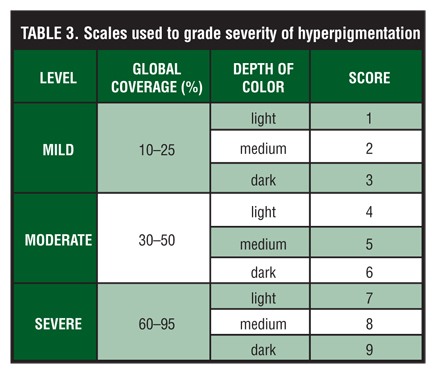
A 90mm VAS was used to collect evaluator perceptions of the extent, severity, or both, of facial hyperpigmentation. Table 3
was used to further evaluate facial hyperpigmentation.
{kind=link}
Objective tolerance. A board-certified dermatologist or designee assessed the extent, severity, or both, of erythema, edema, dryness, and peeling on the volar surface of each forearm. A dermatologist graded the extent, severity, or both of erythema, edema, dryness, and peeling on the right and left sides of the face. The following dermal irritation scale was used to collect evaluator perceptions of erythema, edema, dryness, and peeling at the appropriate study intervals: 0=none, 1=mild, 2=moderate, 3=severe.
Subjective tolerance. Subjects were questioned regarding experiences of subjective irritation (tolerance) and were asked to rate the degree of stinging, tingling, itching, and burning on the volar surface of each forearm, and the right and left sides of the face. The extent, severity, or both, of each were recorded at the appropriate intervals using the following scoring scale: 0=none, 1=mild, 2=moderate, 3=severe.
Questionnaires. The sponsor provided self-assessment questionnaires. Subjects completed the provided question-naires at Baseline, Week 4, Week 7, Week 10, and Week 13.
Statistics. Analysis of variance (ANOVA), Kruskal-Wallis Test, Mann-Whitney test, Wilcoxon Signed-Rank test, and Z test were used to analyze results, with p<0.05 as the cutoff level.
Open patch test procedure. Each subject was given an open patch test on the volar surface of both forearms to determine potential sensitivity to test materials. After thorough cleansing of the test area, three thin layers of the peel (~1mL) were applied to the two test areas followed by neutralizer, three thin layers of RA (~0.5ml), and moisturizer. Tolerance was evaluated 30 to 60 minutes later, 24 hours later, and one week later.
Facial peel procedure. Before peel applications, subjects washed their faces under supervision by massaging cleanser onto the face for one minute before rinsing with water and patting dry. After subjects washed their faces with cleanser, they completed a self-assessment question-naire while acclimating to ambient laboratory conditions for 15 minutes before study evaluations. Tolerance (objective and subjective) evaluations and facial skin attributes were graded for both sides of the face.
The subjects laid down and their eyes were protected with goggles. The subject’s entire face was degreased using acetone applied with rough gauze. A thin layer of gentle soothing ointment was applied with a cotton swab applicator to the skin surrounding the eye, nasolabial folds, entire lip area, and erupted or broken skin as needed.
Three consecutive coats of the peel (5–6mL) were applied with a soft gauze to the entire face of each subject. Two minutes later, the neutralizer was applied and then rinsed with water. Three consecutive coats of the RA (~1.5mL) were applied to the designated side of the face in accordance with the computer-generated randomization code. Moisturizer was applied to the entire face approximately five minutes later. Thirty to 60 minutes later, tolerance evaluations were obtained and subjects completed a post-treatment questionnaire.
Subjects returned to the testing facility for 4-, 7-, and 10-week facial peel treatments and evaluations with a clean and make-up free face (except for SPF 30 sunscreen). After subjects washed their faces with cleanser, they completed a self-assessment questionnaire while acclimating to ambient laboratory conditions for 15 minutes before study evaluations. Tolerance (objective and subjective) evaluations and facial skin attributes were graded for both sides of the face. The peel treatment procedures were performed. Thirty to 60 minutes later, tolerance evaluations were obtained and subjects completed a post-treatment questionnaire.
Subjects returned to the testing facility for a 13-week evaluation with a clean and make-up free face. Daily diaries and all remaining test materials were collected and subjects completed a self-assessment questionnaire. After the 15-minute acclimation period, tolerance evaluations and facial skin attributes were graded for the right and left sides of the face. Adverse events were recorded and analyzed for each subject at each visit.
RESULTS
Patch test. The severities of erythema, edema, dryness, and peeling were graded by the investigator in both the right and left forearms of all subjects at 30 to 60 minutes, 24 hours, and one week after the patch test. The severities of stinging, tingling, itching, and burning were graded by all subjects at each time point. All subjects experienced no adverse reactions with the test materials and all were eligible to participate in the study.
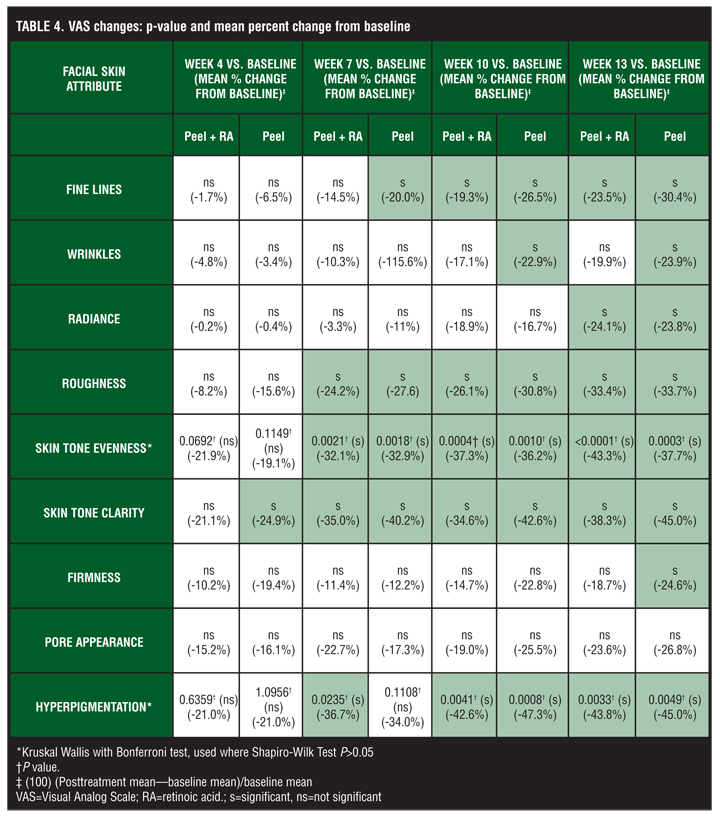
VAS changes. ANOVA with Dunnett’s test was used to compare VAS scores for clinical grading of facial skin attributes, or more specifically, to compare differences between baseline pre-peel assessments and pre-peel assessments at Weeks 4, 7, 10, and 13. If data were not normally distributed as shown by Shapiro-Wilk test (p<0.05), the Kruskal-Wallis test with Bonferroni test was used rather than ANOVA. Results are summarized in Table 4.
{kind=link}
For the peel alone arm, significant differences from baseline begin earliest for skin tone clarity (4 weeks), followed by fine lines, roughness, and skin tone evenness, (7 weeks); wrinkles and hyperpigmentation (10 weeks); and radiance and firmness (13 weeks). Pore appearance showed no significant change at any time point.
For the peel + RA arm, significant differences began earliest for roughness, skin tone evenness, skin tone clarity, and hyperpigmentation (7 weeks), followed by fine lines (10 weeks) and radiance (13 weeks).
Wrinkles, firmness, and pore appearance showed no significant change from baseline at any time point.
Only in hyperpigmentation does a significant difference occur earlier in the peel + RA than peel alone (7 weeks vs. 10 weeks). A significant difference appears earlier in peel than in peel + RA for skin tone clarity (4 weeks vs. 7 weeks) and fine lines (7 weeks vs. 10 weeks). A significant difference was evident in peel but not peel + RA for wrinkles (10 weeks) and firmness (13 weeks). A significant difference from baseline was not observed with peel or peel + RA for pore appearance.
Depending on the normality of the data distribution, the paired t-test or Wilcoxon signed-rank test was used to determine the differences between the two treatments at each time interval. The results are shown in Table 5.
{kind=link}
When peel was compared to peel + RA, VAS score changes from baseline (baseline—post-treatment score) were significantly different only for skin tone clarity (p=0.0085) and radiance (p =0.0479), both at seven weeks. For skin tone clarity, mean differences from baseline for peel and peel + RA at Week 7 were -28.7 and -24.4, respectively, suggesting that RA does not enhance the peel-induced improvement in clarity. For radiance, median differences were -6.8 and -2.0, respectively, suggesting that RA does not enhance improvement in skin radiance.
Overall facial appearance. The average of percent changes from baseline for fine lines, wrinkles, radiance, roughness, evenness, clarity, firmness, pores, and hyperpigmentation for 4, 7, 10, and 13 weeks was defined as the overall facial appearance. The mean percent changes for all skin parameters are shown in Table 6.
{kind=link}
Objective tolerance. The pre- and post-peel severities of erythema, edema, dryness, and peeling on both sides of the faces were graded by the investigator at Baseline and Weeks 4, 7, 10, and 13. At all time points, pre- and post-peel severity grades greater than 0 were limited to erythema for both peel and peel + RA treatment arms, suggesting that the peel alone and the addition of RA do not cause dryness, edema, or peeling.
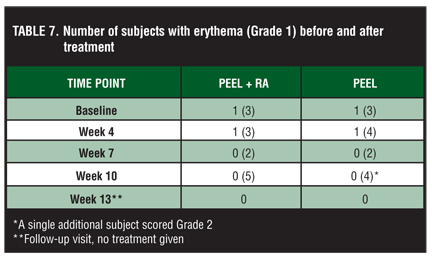
As shown in Table 7, at baseline, a single pre-peel subject in both treatment arms was graded 1 for erythema. Three post-peel subjects were graded 1 for erythema in both treatment arms.
{kind=link}
In Weeks 4 and 10, pre-peel severity grades for erythema never exceeded grade 1. Erythema of grade 1 was noted only in one subject at Week 4 in each treatment arm. Erythema was graded 0 in both arms at Week 10. At Week 7, all pre-peel parameters were graded 0 in both treatment arms.
Post-peel severity grades for erythema never exceeded grade 1, except for a single subject graded 2 at Week 10 for the peel treatment arm. At Week 4, the number of subjects with erythema was 3 for the peel + RA arm and 4 for the peel arm. Two subjects had erythema in both arms at Week 7. At Week 10, the number increased to 5 in the peel + RA arm and 5 in the peel arm (including one subject graded 2).
Subject 2 experienced erythema at Baseline and Weeks 4, 7, and 10. Subject 3 had erythema at Baseline and Weeks 7 and 10. Subjects 1, 10, and 11 experienced erythema at Week 10 in both arms. No other subjects experienced erythema in either treatment arm. Erythema was graded 0 in all subjects in both treatment arms at Week 13.
In Weeks 4, 7, 10, and 13, the total number of subjects with post-peel erythema was 10 for the peel + RA treatment arm compared to 11 for the peel arm, suggesting that the addition of RA to the peel does not increase the frequency of erythema.
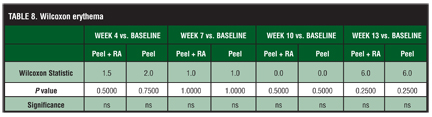
The Wilcoxon signed-rank test was used to determine differences within each treatment from baseline visit to post-peel treatment to each post-peel treatment study interval. For dryness, edema, and peeling, all cells were graded zero, so the Wilcoxon signed-rank statistic could not be calculated. For erythema, the differences between the peel + RA and peel alone at each time point were not significant (Table 8). These results suggest that the addition of RA to the peel treatment does not enhance the dryness, erythema, edema, and peeling associated with peeling at each time point.
{kind=link}
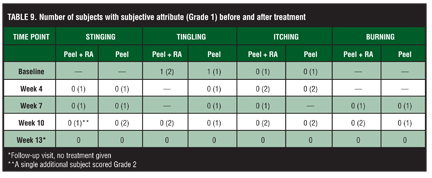
Subjective tolerance. The severities of stinging, tingling, itching, and burning on both sides of the faces were graded by subjects at Weeks 4, 7, 10, and 13. The results of these subjective evaluations are shown in Table 9.
{kind=link}
At Baseline, a single pre-peel subject in both treatment arms was graded 1 for tingling. All other attributes were graded 0. Two post-peel subjects were graded 1 for tingling and one post-peel subject was graded 1 for itching in the peel + RA treatment arm. In the peel arm, one post-peel subject was graded 1 for tingling and one was graded 1 for itching. All other attributes were graded 0.
In Weeks 4 and 10, pre-peel severity grades were graded 0 for all skin sensations in both treatment arms. Pre-peel data were not available for Week 13. At Week 4, post-peel stinging (n=1) and itching (n=2) were noted in the peel + RA treatment arm, whereas stinging (n=1), tingling (n=1), and itching (n=2) were observed in the peel arm. In Week 7, pre-peel severity grades were graded 0 for all skin sensations in both treatment arms.
At Week 7, post-peel stinging (n=1), itching (n=1), and burning (n=1) were observed in the peel + RA arm while stinging (n=1), tingling (n=1), and burning (n=1) were noted in the peel treatment arm. At Week 10, all skin sensations were graded 0. Post-peel stinging (n=1), tingling (n=2), itching (n=2), and burning (n=2) were observed in the peel + RA arm while stinging (n=2), tingling (n=1), itching (n=2), and burning (n=1) were noted in the peel treatment arm. All sensations were graded 0 in both treatment arms at Week 13.
Skin sensations appeared to reach a small maximum (n=2) at Week 10 for tingling, itching, and burning in the peel + RA arm and for tingling and itching in the peel treatment arm. All were resolved at Week 13. These results suggest that the peel alone treatment may occasionally cause stinging, tingling, itching, and burning, and that the addition of RA does not enhance these sensations.
For stinging (13 weeks) and burning (4 weeks, 13 weeks) all cells were graded zero, so the Wilcoxon signed-rank statistic could not be calculated. For the remaining time points, differences between the peel + RA and peel treatments were not significant for stinging and burning. For tingling and itching, differences between the peel + RA and peel treatments were not significant at each time point.
These results suggest that the addition of RA to the peel treatment does not significantly enhance the tingling, stinging, itching, and burning associated with peel treatment at each time point.
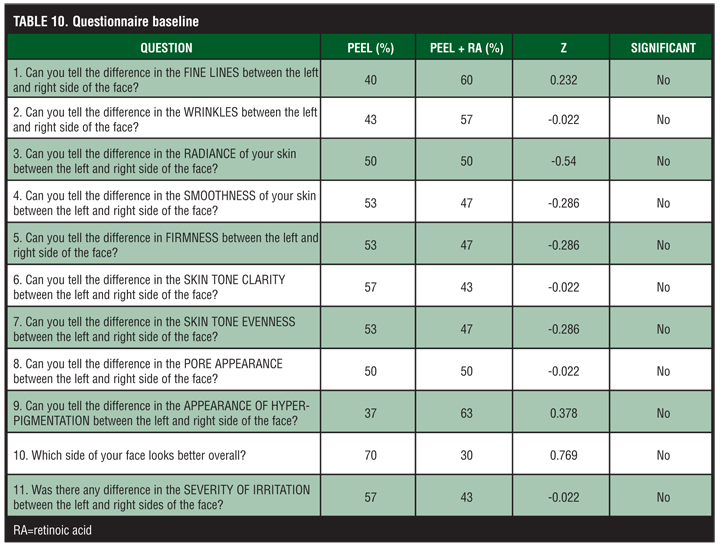
Questionnaire data. The Z test was used to analyze questionnaire responses. The proportions of subjects choosing the central (neutral) responses was split equally and added to the response proportion of the top and bottom choices. Statistical significance existed for Z scores greater than or equal to the absolute value of 1.96 at the 95% confidence level. Table 10 shows the questions (used at all time points) with data at Baseline.
{kind=link}
The Z values associated with comparing the peel + RA and peel treatment arms were not significant for fine lines, wrinkles, radiance, smoothness, firmness, skin clarity, skin evenness, pore appearance, appearance of hyperpigment-ation, and severity of irritation throughout the entire study period.
Adverse Events
Adverse event (AE) forms were completed. No AEs were serious. A total of 18 AEs were recorded. Seven were “possibly” related to treatment (Table 11
). These seven AEs were all continuous, of mild severity, and required no action. All AEs were either resolved (n=16) or improved (n=2). None required intervention or discontinuing of peel or peel + RA treatment.
{kind=link}
Adverse events not related to study treatment were exacerbation of acid reflux, breakthrough menstrual bleeding, sinus infection, worsening of gastric reflux disease, irritable bowel syndrome, benign hemangioma of liver, benign colon polyps, nausea after colonoscopy, stomach flu, exacerbation of depression, and rhinitis. All were observed on a single occasion except rhinitis, which occurred twice.
DISCUSSION
This study compared the tolerance and efficacy of RA used as a post-treatment product on subjects receiving a full-face peel treatment. Among the objective facial treatment parameters, VAS scores indicate that both the peel and peel + RA treatments achieved significant improvement in fine lines, radiance, roughness, skin tone clarity, skin tone evenness, and hyperpigmentation appearance over the study period. Improvements in wrinkles and firmness were not observed in the peel + RA arm while pore appearance failed to improve in either treatment arm. Only skin tone clarity improved as early as four weeks, and this was observed in the peel treatment arm. In the peel + RA arm, clarity was not significantly improved until Week 7, when improvement was noted in the most parameters in both treatment arms. The peel alone performed statistically significantly better at Week 7 in skin tone clarity. Improvement was the least in wrinkles, pore appearance, radiance, and firmness. These results suggest that the addition of RA to peel treatment does not significantly enhance the peel-induced improvement in any of the nine facial attributes. Only in hyperpigmentation did a significant difference occur earlier in the peel + RA than peel alone (7 weeks vs. 10 weeks), suggesting that the addition of RA may slightly enhance the effect of the peel for this attribute.
There was no statistically significant difference between the peel and peel + RA at Week 13 for any attribute. The only significant differences were in radiance and clarity at Week 7, indicating the RA does not enhance peel-induced improvement in either facial attribute. Improvements in fine lines, wrinkles, radiance, roughness, skin tone evenness, firmness, pore appearance, and hyperpigmentation did not differ significantly between the peel and peel + RA treatment arms. Improvement in overall facial appearance was greater in the peel alone arm, indicating further that RA does not enhance peel-induced improvement.
Irritation results show that peel alone and the addition of RA do not cause dryness, edema, or peeling, and that the frequency of peel-induced erythema does not increase with the addition of RA. Regarding subjective parameters, the results suggest that the peel alone treatment may occasionally cause stinging, tingling, itching, and burning, and that the addition of RA does not enhance these effects.
The questionnaire data show that the subject-perceived improvements with the peel treatment did not differ significantly from subject-perceived improvements of the peel + RA treatment for fine lines, wrinkles, radiance, smoothness, firmness, skin clarity, skin evenness, pore appearance, and appearance of hyperpigmentation.
A total of 18 AEs were recorded. Seven were “possibly” related to treatment. These seven AEs were all continuous and of mild severity. All were either resolved (n=16) or improved (n=2). None required intervention or discontinuing of peel or peel + RA treatment.
Although improvement in most facial attributes was observed, the addition of RA did not enhance the effects. The results of this study are similar to those of Humphreys et al[14] who compared the efficacy of 40% trichloroacetic acid, a medium-depth chemical peel, on photodamaged skin, with and without RA cream before and after treatment. The present study, however, did not include pretreatment with RA.
The peel used in the present study was a combination of ingredients (Table 1) blended to optimize efficacy and minimize irritation to the skin. Similar combinations reported in the literature include hydroquinone, tretinoin, and mometasone furoate with glycolic acid peels for the treatment of melasma[15] and a salicylic acid and mandelic acid combination for the treatment of acne.[16]
Pyruvic acid is a well-established peeling agent. Not as well known as pyruvic acid, phytic acid is a large molecule that is not an AHA. Phytic acid has been studied for many years due to its chelating potential for metal ions of calcium, zinc, and iron. Oral phytic acid is effective against acne and improves skin color, blood circulation, and fingernail growth. It is also a component of antidandruff hair lotions, rinses, and shampoos, and of skin care lotions[.17] Like glycolic acid, phytic acid inhibits tyrosinase,[17,18] thus decreasing the rate of melanin synthesis and reducing pigmentation.[19]
Phytic acid is also an excellent oxidant.17,18 This is important because peeling procedures produce free radicals of oxygen, which can damage structures that participate in skin regeneration after the peel. Free radicals of oxygen also play a major role in cell degeneration in aging.18 Limitations of this study are the small number of patients.
CONCLUSION
The addition of RA after peel treatment does not significantly enhance the following: 1) peel-induced improvement in fine lines, wrinkles, radiance, roughness, evenness, clarity, firmness, pore appearance, and hyperpigmentation; 2) peel-induced erythema, dryness, edema, peeling, stinging, tingling, itching, and burning; and 3) subject-perceived improvement in fine lines, wrinkles, radiance, smoothness, firmness, skin clarity, skin evenness, pore appearance, and appearance of hyperpigmentation.
References
1. Monheit GD, Chastain MA. Chemical peels. Facial Plast Surg Clin North Am. 2001;2:239–255.
2. Monheit GD. Chemical peels. Skin Therapy Lett. 2004;2:6–11.
3. Ditre CM, Griffin TD, Murphy GF, et al. Effects of alpha-hydroxy acids on photoaged skin: a pilot clinical, histologic, and ultrastructural study. J Am Acad Dermatol. 1996;2: 187–195.
4. Piacquadio D, Dobry M, Hunt S, et al. 70% glycolic acid peels as a treatment for photodamaged skin. A pilot study. Dermatol Surg. 1996;5:449–452.
5. Stiller MJ, Bartolone J, Stern R, et al. Topical 8% glycolic acid and 8% L-lactic acid creams for the treatment of photodamaged skin. A double-blind vehicle-controlled clinical trial. Arch Dermatol. 1996;6:631–636.
6. Cordero A Jr. La vitamina a acida en la piel senil. Actualizaciones Terapéuticas Dermatológicas. 1983;6: 49–54.
7. Kligman AM, Grove GL, Hirose R, Leyden JJ. Topical tretinoin for photoaged skin. J Am Acad Dermatol. 1986;4:836–859.
8. Kang S, Voorhees JJ. Photoaging therapy with topical tretinoin: an evidence-based analysis. J Am Acad Dermatol. 1998;2:S55–S61.
9. Griffiths CE, Kang S, Ellis CN, et al. Two concentrations of topical tretinoin (retinoic acid) cause similar improvement of photoaging but different degrees of irritation. A double-blind, vehicle-controlled comparison of 0.1% and 0.025% tretinoin creams. Arch Dermatol. 1995;9:1037–1044.
10. Kligman A. Results of a pilot study evaluating the compatibility of topical tretinoin in combination with glycolic acid. Cosmetic Dermatol. 1993;6:28–32.
11. Kligman A. Compatability of a glycolic acid cream with topical tretinoin for the treatment of photo damaged face of older women. J Geriatr Dermatol. 1993;1:179–181.
12. Weiss JS, Shavin JS. An evaluation of the compatibility of tretinoin cream 0.05% and a glycolic acid 8% solution for acne-prone skin. Cosmetic Dermatol. 1996;9:26–38.
13. Kim IH, Kim HK, Kye YC. Effects of tretinoin pretreatment on TCA chemical peel in guinea pig skin. J Korean Med Sci. 1996;4: 335–341.
14. Humphreys TR, Werth V, Dzubow L, Kligman A. Treatment of photodamaged skin with trichloroacetic acid and topical tretinoin. J Am Acad Dermatol. 1996;4:638–644.
15. Godse KV. Triple combination of hydroquinone, tretinoin and mometasone furoate with glycolic acid peels in melasma. Indian J Dermatol. 2009;54:92–93.
16. Garg VK, Sinha S, Sarkar R. Glycolic acid peels versus salicylic-mandelic acid peels in active acne vulgaris and post-acne scarring and hyperpigmentation: a comparative study. Dermatol Surg. 2009;35:59–65.
17. Graf E. Applications of phytic acid. JAOCS. 1983;11: 1861–1867.
18. Deprez P. Easy phytic solution: a new alpha hydroxyl acid peel with slow release and without neutralization. Int J Cosmet Surg Aesthetic Dermatol. 2003;1:45–51.
19. Moy LS, Murad H, Moy RL. Glycolic acid peels for the treatment of wrinkles and photoaging. J Dermatol Surg Oncol. 1993;3:243–246.