 J Clin Aesthet Dermatol. 2021;14(3):32–37.
J Clin Aesthet Dermatol. 2021;14(3):32–37.
by James Q. Del Rosso, DO, and Emil Tanghetti, MD
Dr. Del Rosso is Research Director at JDR Dermatology Research in Las Vegas, Nevada, is with Thomas Dermatology in Las Vegas, Nevada, and is an adjunct clinical professor of dermatology at Touro University Nevada in Henderson, Nevada. Dr. Tanghetti is with the Center for Dermatology and Laser Surgery in Sacramento, California.
FUNDING: This work was funded by Aclaris Therapeutics, Inc. and EPI Health, LLC.
DISCLOSURES: Dr. Del Rosso is a consultant for Almirall, BiopharmX, EPI Health, Evommune, Galderma, Bausch Health (Ortho Dermatologics), Leo Pharma, and Vyne Therapeutics; has served as a consultant for Aclaris and Allergan; is an investigator for Almirall, BiopharmX, Galderma, Bausch Health (Ortho Dermatologics), Leo Pharma, and Vyne Therapeutics; and is on the speaker bureau of Almirall, EPI Health, Galderma, Bausch Health (Ortho Dermatologics), and Vyne Therapeutics. Dr. Tanghetti is an investigator for Allergan and a consultant for Aclaris, Galderma, Cynosure/Hologic, and Accure.
ABSTRACT: Background. Rosacea is a chronic, multisymptom, inflammatory condition that affects the centrofacial skin. Facial erythema associated with rosacea can negatively impact a patient’s quality of life and is often hard to treat.
Objective. We sought to review the literature on the role of alpha-adrenergic receptors (alpha-adrenoceptors) in the context of persistent facial erythema in patients with rosacea and the use of oxymetazoline hydrochloride cream 1% as a topical treatment.
Methods. PubMed was searched; search terms included “alpha adrenoceptor,” “oxymetazoline,” and “rosacea.” Additional articles were identified from the reference lists of the results.
Results. Some alpha-adrenoceptor agonists have vasoconstrictive properties and may be used topically to treat persistent facial erythema in rosacea. Oxymetazoline hydrochloride cream 1% is an alpha1A-adrenoceptor agonist approved for the treatment of persistent facial erythema associated with rosacea. Based on our review, we discuss the role of the alpha-adrenoceptor in persistent facial erythema; provide an overview of the mechanism of action of alpha-adrenoceptor agonists, such as oxymetazoline, in the treatment of persistent facial erythema; and summarize the clinical development and data to date demonstrating the efficacy and safety of oxymetazoline in the treatment of persistent facial erythema associated with rosacea.
Conclusion. The review of available literature suggests that oxymetazoline cream is well-tolerated, safe, and effective for the treatment of persistent facial erythema in rosacea and is an important component of combination treatment regimens, which are likely to become the standard of treatment for rosacea in the future
Keywords: Adrenergic alpha-1 receptor agonists, adrenergic receptor agonists, adrenoceptors, erythema, erythematotelangiectatic rosacea, oxymetazoline, rosacea, topical administration, vasoconstriction, vasoconstrictor agents
Rosacea is a chronic inflammatory condition that affects the centrofacial skin. The primary features of rosacea include persistent facial erythema (PFE), transient erythema or flushing, papules and pustules, and telangiectasia.1–3 Secondary features including phymatous changes, erythematous plaques, feelings of burning or stinging, dryness and scaling, edema, peripheral location, and ocular symptoms, such as blepharitis or conjunctivitis, which may be present in addition to or instead of the primary rosacea manifestations.1–3 While the pathophysiology of rosacea is not completely understood, it is thought that neurovascular dysregulation and abnormalities in the adaptive and innate immune systems predispose individuals to developing rosacea, leading to abnormal, sustained vasodilation in the facial skin.4
Facial erythema is recognized as a frequent and consistent feature of rosacea and also the most difficult one to treat.5 Facial erythema is often symptomatic; most people experiencing erythema associated with rosacea are embarrassed by the condition and feel that they are judged unfairly in people’s first impressions.6,7 While the negative impact of skin diseases on quality of life is often underestimated by physicians,7 effective treatment of rosacea-associated PFE is exceedingly important to patients with rosacea.
Topical alpha-adrenergic receptor (alpha-adrenoceptor) agonists target an underlying cause of diffuse PFE and have been recommended by the American Acne and Rosacea Society for this indication.8 Oxymetazoline hydrochloride cream 1% (RHOFADE®; EPI Health, Charleston, South Carolina) is an alpha1A-adrenoceptor agonist approved by the United States Food and Drug Administration for the topical treatment of PFE associated with rosacea in adults.9 Here, we provide an overview of the pathophysiology of PFE associated with rosacea, review the development of oxymetazoline as a treatment for PFE, and summarize the current clinical data assessing the pharmacokinetics, efficacy, and safety of oxymetazoline in adult patients with PFE associated with rosacea.
Role of Adrenoceptors in PFE and the Adrenoceptor Agonist Mechanism of Action
Several cutaneous vascular changes that occur with rosacea are mediated by neurovascular dysregulation and abnormalities in the innate and adaptive immune systems.10–12 Toll-like receptor 2 is upregulated in rosacea, which can lead to increased levels of matrix metalloproteinases, kallikrein-5, and cathelicidins such as LL-37.10–14 Increased production of LL-37 can activate and augment pro-angiogenic and pro-inflammatory signaling pathways, trigger mast-cell activation, and lead to macrophage and neutrophil chemotaxis. Chronic inflammation can result in increased superficial cutaneous vascularization and vasodilation, leading to edema and production of pro-inflammatory cytokines. Additionally, trigger factors, such as stress, spices, and heat can lead to the activation of transient receptor potential (TRP) ion channels TRPV1/TRPA1, which amplify the already heightened inflammatory response. This augmentation of pro-inflammatory pathways is thought to ultimately contribute to the chronic vasodilation and dermal matrix degradation responsible for some of the visible manifestations of rosacea, including PFE.10,14
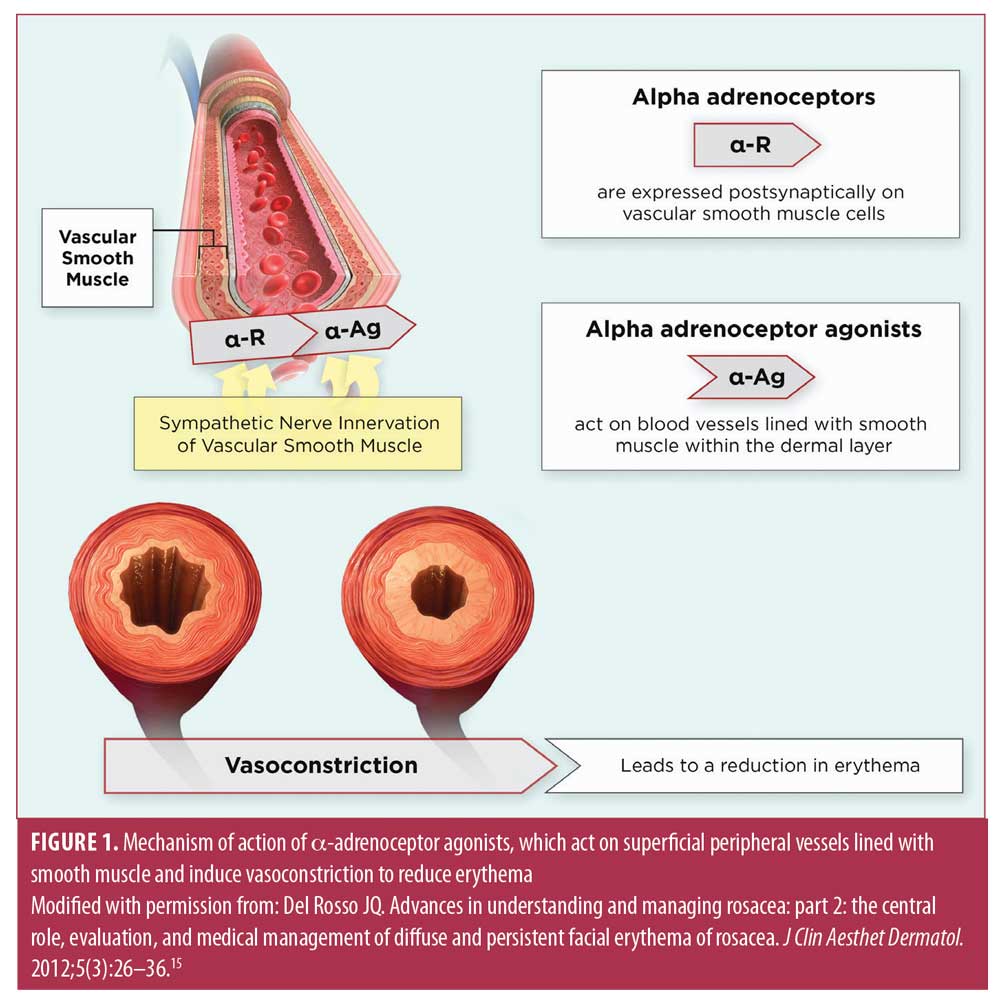
The sympathetic nervous system is the main regulator of the superficial cutaneous vasculature and uses several adrenoceptors, which vary in their tissue distribution and function, to modulate cutaneous circulation.10 The superficial cutaneous blood vessels that are in a sustained dilated state in rosacea contain a smooth muscle layer and remain responsive to adrenergic stimuli (Figure 1).15,16 Peripheral smooth muscle vasoconstriction is primarily mediated by alpha1-adrenoceptors and the subset of alpha2-adrenoceptors that are expressed postsynaptically on vascular smooth muscle cells.10,17,18 An additional subset of alpha2-adrenoceptors are expressed presynaptically on sympathetic nerve terminals and/or postsynaptically in the vascular endothelium, depending on blood vessel type; however, activation of these alpha2-adrenoceptors may promote vasodilation.17,18 Oxymetazoline is an alpha1A-adrenoceptor agonist that causes cutaneous vasoconstriction by postsynaptic activation of alpha1A adrenoceptors.9,18 Although alpha-adrenoceptor subtypes are targets for drug therapy of PFE in rosacea, the effects of selective receptor subtype stimulation or inhibition on clinically relevant differences between therapies remain theoretical. Preclinical models have demonstrated comparable reductions in erythema mediated via alpha1– and alpha2-adrenoceptor agonists.18 Further research might elucidate the clinical implications of therapeutic activity according to different alpha-adrenoceptor subtypes.
Evidence from preclinical models also suggests that alpha-adrenoceptor agonists might have effects other than vasoconstriction. Anti-inflammatory effects have been attributed to alpha-adrenoceptor agonist treatment, including a reduced production of pro-inflammatory cytokines, modulation of arachidonic acid and arachidonic acid-derivative protein activity, reduction in the T-cell stimulatory capacity of dendritic cells, and inhibition of respiratory burst activity.5,19–21 Alpha-adrenoceptor agonists also affect other aspects of immune function, including T-cell activation and proliferation, mast cell infiltration, antibody responses, heat shock protein signaling, and mitogen-activated protein kinase pathway signaling.19,22–26 Studies have also linked alpha-adrenoceptor agonist exposure to the inhibition of neovascularization through reduced vascular endothelial growth factor expression.27,28 Further studies are needed to determine whether these functions mediate the PFE reduction associated with alpha-adrenoceptor agonist use.
History of the Development of Oxymetazoline
Alpha-adrenoceptor agonists were traditionally used in over-the-counter therapies to treat congestion.29 Due to their vasoconstrictive and anti-inflammatory properties, locally applied alpha1-adrenoceptor agonists effectively decrease mucous membrane erythema and edema.29 Oxymetazoline was first approved as a decongestant intranasal spray in 1964 and was made available as an over-the-counter medication in 1976.30
The first use of oxymetazoline as a topical treatment for PFE associated with rosacea was reported in 2007.29 Topical application of oxymetazoline hydrochloride 0.05% solution once daily greatly improved the PFE, stinging/burning, and episodic flushing experienced by two patients with treatment-resistant erythematotelangiectatic rosacea. The treatment effects were sustained through the last follow-up visits for each patient, which were eight and 17 months after treatment initiation, respectively. Neither patient experienced adverse effects or a return of symptoms during that time. Based on these results, oxymetazoline use for the treatment of PFE associated with rosacea was investigated.
Pharmacokinetic data. The pharmacokinetic profile of oxymetazoline was evaluated in a Phase II, dose-ranging, multicenter, randomized, double-blind, parallel-group study (NCT01735201). Eligible patients with moderate to severe PFE associated with rosacea were randomized to receive topical oxymetazoline cream 0.5%, 1.0%, or 1.5% or vehicle once or twice daily for 28 days.31 Consistent, predictable pharmacokinetic parameters were observed after oxymetazoline administration, even at the highest level of exposure. Mean maximum plasma concentrations were generally comparable across all groups. Systemic exposure was low overall and increased in an approximately dose-proportional manner. Additionally, the effective half-life was 18 to 28 hours across groups, demonstrating a long duration of action.31 These results suggested that oxymetazoline treatment may be compatible with long-term, chronic use.
Clinical data. The efficacy and safety of oxymetazoline treatment of moderate to severe PFE associated with rosacea has been evaluated in several trials (Table 1).32–36 The aforementioned Phase II study also evaluated the efficacy and safety of the three doses of oxymetazoline hydrochloride cream (0.5%, 1.0%, and 1.5%; N=356).32 Significantly higher proportions of patients who received any oxymetazoline dose once daily versus vehicle once daily and who received oxymetazoline 1.5% and 1.0% twice daily versus vehicle twice daily demonstrated a response, defined as at least a two-grade improvement from baseline on the Clinician Erythema Assessment (CEA) and Subject Self-assessment of Erythema (SSA) scales at Day 28.32 At most time points, the proportions of responders were comparable in the oxymetazoline 1.5% and oxymetazoline 1.0% treatment groups and were lower in the oxymetazoline 0.5% treatment group for both once-daily and twice-daily dosing regimens. Treatment-related treatment-emergent adverse events (TEAEs) were reported by 9.8 percent of patients; most were mild or moderate in severity. Dermal tolerability ratings were similar between the oxymetazoline and vehicle treatment groups with once- or twice-daily dosing.

Based on these efficacy, safety, and tolerability findings, oxymetazoline hydrochloride cream 1.0% daily was selected for evaluation in Phase III studies. Specifically, the efficacy and safety of oxymetazoline were further evaluated in the pivotal, identically designed, multicenter, double-blind, parallel-group, vehicle-controlled Phase III trials REVEAL 1 (NCT02131636; N=440) and REVEAL 2 (NCT02132117; N=445).33,34 Eligible patients with moderate to severe PFE associated with rosacea were randomized 1:1 to receive topical oxymetazoline hydrochloride cream 1% or vehicle once daily for 29 days and were then followed for an additional 28 days. In both studies, significantly greater proportions of patients treated with oxymetazoline versus vehicle achieved at least a two-grade improvement in both CEA and SSA scores at three, six, nine, and 12 hours postdose and overall on Day 29 (all p<0.05).33,34 Pre- and posttreatment images of a patient from the REVEAL 2 study are shown in Figure 2. Treatment-related TEAEs were reported in 6.3 percent and 8.5 percent of oxymetazoline-treated patients versus in 0.5 percent and 5.0 percent of patients receiving the vehicle in REVEAL 1 and REVEAL 2, respectively. Increased itching was reported by 23.4 percent of oxymetazoline-treated versus 15.6 percent of vehicle-treated patients in REVEAL 1; incidence rates of stinging/burning, dryness, and scaling were comparable between treatment groups in both studies. Additionally, low proportions of patients experienced a rebound effect at the end of the posttreatment period (REVEAL 1: oxymetazoline, 2.2% and vehicle, 1.1%; REVEAL 2: oxymetazoline, 1.2% and vehicle, 0%), which is encouraging, as rebound effects have been observed after alpha2-adrenoceptor agonist brimonidine 0.33% gel use.37,38 Overall, these results confirmed the safety and efficacy of oxymetazoline for PFE associated with rosacea in adults.

In a post-hoc analysis of the REVEAL studies (N=885), the timing of oxymetazoline effects was assessed.39 Significantly greater proportions of patients treated with oxymetazoline versus vehicle achieved at least a one-grade composite and individual CEA and SSA improvements at all time points on Day 1 (p<0.001 for all comparisons).39 These results indicated that oxymetazoline significantly reduces PFE as soon as one hour after application and maintains this effect for up to 12 hours.
The long-term effects of oxymetazoline were assessed in the Phase III, open-label REVEAL long-term study (NCT02095158).35 Patients with moderate to severe PFE in rosacea (N=440) applied oxymetazoline hydrochloride cream 1% topically daily for 52 weeks, followed by a two-week posttreatment period in which no medication was applied. Treatment-related TEAEs were reported by 8.2 percent of patients; most were mild or moderate in severity.35 The incidence of treatment-related TEAEs was highest during the first 90 days of treatment (5.9%) and progressively decreased over the three subsequent 90-day periods (1.5%, 0.7%, and 0.3%, respectively). Low proportions of patients exhibited at least a one-grade worsening in dermal tolerability assessments at Week 52 (3.7%–9.3%) and two patients each (0.7%) at Weeks 52 and 54 experienced posttreatment rebound effects. Additionally, increasing proportions of patients achieved at least a two-grade composite CEA and SSA improvement from baseline from Day 1 (six hours posttreatment, 17.8%) to Week 52 (six hours posttreatment, 43.4%). These results further indicated that oxymetazoline was safe and maintained efficacy for the long-term treatment of PFE associated with rosacea.
In a post-hoc analysis of the REVEAL long-term study, increasing proportions of oxymetazoline-treated patients had at least a one-grade composite CEA and SSA improvement from baseline over time (Day 1, 77.5%; Week 52, 88.5%).40 Among patients who did not respond at a given time point, the probability of a response at a later time point was approximately 60 percent. The probability of remaining a responder was approximately 90 percent. These results further support the sustained efficacy of oxymetazoline treatment.
Finally, a Phase IV study used the REVEAL data to assess whether reference to baseline photographs improves PFE evaluation accuracy.41 Based on dermatologist-blinded assessments of photographs from baseline and each postdose time point, significantly greater proportions of patients treated with oxymetazoline versus vehicle achieved at least a one-grade CEA improvement at each time point. The proportion of oxymetazoline-treated patients who achieved at least a one-grade CEA improvement by photographic evaluation was not significantly different from the proportion who achieved at least a one-grade CEA improvement as assessed via live, static grading during the Phase III trials; however, a significantly lower proportion of vehicle-treated patients achieved at least a one-grade CEA improvement by photographic evaluation. These results indicate that reference to a baseline photograph may improve PFE assessment accuracy.
Following the REVEAL studies, a Phase IV, open-label study evaluated the safety and efficacy of oxymetazoline as an adjunctive treatment with energy-based therapy for patients with moderate to severe PFE of rosacea (NCT03380390).36 Patients received one of four energy-based therapies (potassium titanyl phosphate laser, intense pulsed light therapy, or pulsed-dye laser [PDL; Vbeam Perfecta® from Candela Medical, Wayland, Maryland, or PDL Cynergy™ from UPMC, Pittsburgh, Pennsylvania]) on Day 1 and Day 29 and once-daily oxymetazoline hydrochloride cream 1% on Days 3 through 27 and Days 31 through 56 (N=46). All patients demonstrated improvements from baseline in CEA, with 90.7 percent of patients demonstrating improvements at six hours posttreatment on Day 56. Treatment-related TEAEs were reported by 8.7 percent of patients; all were mild or moderate in severity. No patients experienced severe dermal tolerability symptoms. Although this study was not designed to evaluate potential synergistic effects, these results demonstrate that combined energy-based and oxymetazoline therapy was safe, well-tolerated, and effective in reducing PFE associated with rosacea.
Combination Treatment Regimens
Several studies have evaluated the efficacy of combination treatments for rosacea that include alpha-adrenoceptor agonists. The additive effects of oxymetazoline and PDL treatment on cutaneous blood flow were examined in a preclinical mouse model.42 Mice treated with oxymetazoline alone demonstrated persistent blood flow and mice treated with PDL plus saline demonstrated an initial decrease in blood flow followed by reperfusion over the seven-day study period. Persistent vascular shutdown was only observed in mice treated with oxymetazoline plus PDL, indicating an additive vascular effect with combination treatment.
The effects of PDL and oxymetazoline combination treatment on PFE and telangiectasia were also investigated in a retrospective analysis using pre- and posttreatment images of patients who had undergone PDL treatment at least once and used oxymetazoline hydrochloride cream 1% daily for at least one month.43 Most patients experienced improvements from baseline in CEA grade and substantial clearance of telangiectasias, with greater improvements realized in patients with elevated baseline disease severity. These results suggest that combination therapy can treat multiple rosacea symptoms simultaneously; however, lack of a control group limits the conclusions that can be drawn.
A multicenter, randomized, double-blind study evaluated the efficacy of combinations of ivermectin 1% cream and the alpha2-adrenoceptor agonist brimonidine 0.33% gel, which have individually shown efficacy in reducing inflammatory lesions and reducing PFE, respectively.44 Patients with moderate to severe PFE and inflammatory lesions were treated with ivermectin and brimonidine for 12 weeks (IV+BR12); brimonidine vehicle for four weeks, then brimonidine for eight weeks with ivermectin for 12 weeks (IV12+BR8); or brimonidine vehicle and ivermectin vehicle for 12 weeks (vehicle). A significantly greater percentage of IV+BR12 patients achieved Investigator’s Global Assessment (IGA) success, defined as clear/almost clear overall including background erythema and inflammatory lesions at three hours postdose at Week 12, relative to the vehicle group (61.2% vs. 36.8%; p=0.003). The proportion achieving IGA success with IV12+BR8 was not statistically greater than with vehicle (50% vs. 36.8%; p=0.135) and was lower than that with IV+BR12. While this study did not evaluate oxymetazoline, it demonstrates that combination topical treatment incorporating agents that specifically target both papulopustular lesions (such as ivermectin) and PFE (an alpha-adrenoceptor agonist), can improve overall therapeutic results in reducing visible manifestations of rosacea that are common to most affected patients.
Conclusion
PFE is the most common visible sign of rosacea and also the most difficult to treat.5 Oxymetazoline is an alpha1A-adrenoceptor agonist with vasoconstrictive properties approved for the topical treatment of PFE associated with rosacea in adults.9 Oxymetazoline hydrochloride cream 1% is well-tolerated, safe, and effective for the treatment of PFE of rosacea without a significant risk of apparent worsening of facial erythema and rebound, or the paradoxical erythema sometimes associated with topical brimonidine. Combination treatment regimens have demonstrated promising efficacy in simultaneously treating multiple clinical manifestations of rosacea. Consequently, combination regimens incorporating medical therapies and physical devices will likely become a recognized standard of rosacea management, especially as more data are presented in the future.
Acknowledgments
Editorial and medical writing support was provided by Peloton Advantage, LLC, an OPEN Health company (Parsippany, New Jersey), and was funded by Aclaris Therapeutics, Inc. and EPI Health, LLC.
References
- Tan J, Almeida LM, Bewley A, et al. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017;176(2):431–438.
- Odom R, Dahl M, Dover J, et al. Standard management options for rosacea, part 1: overview and broad spectrum of care. Cutis. 2009;84(1):43–47.
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol. 2002;46(4):584–587.
- Woo YR, Lim JH, Cho DH, Park HJ. Rosacea: molecular mechanisms and management of a chronic cutaneous inflammatory condition. Int J Mol Sci. 2016;17(9):1562.
- Piwnica D, Rosignoli C, de Menonville ST, et al. Vasoconstriction and anti-inflammatory properties of the selective alpha-adrenergic receptor agonist brimonidine. J Dermatol Sci. 2014;75(1):49–54.
- Dirschka T, Micali G, Papadopoulos L, et al. Perceptions on the psychological impact of facial erythema associated with rosacea: results of international survey. Dermatol Ther (Heidelb). 2015;5(2):117–127.
- van der Linden MM, van Rappard DC, Daams JG, et al. Health-related quality of life in patients with cutaneous rosacea: a systematic review. Acta Derm Venereol. 2015;95(4): 395–400.
- Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 5: a guide on the management of rosacea. Cutis. 2014;93(3):134–138.
- Rhofade [package insert]. Charleston, SC: EPI Health; 2019.
- Del Rosso JQ. Management of facial erythema of rosacea: what is the role of topical alpha-adrenergic receptor agonist therapy? J Am Acad Dermatol. 2013;69(6 Suppl 1):S44–S56.
- Steinhoff M, Buddenkotte J, Aubert J, et al. Clinical, cellular, and molecular aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011;15(1):2–11.
- Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77–81.
- Schauber J, Dorschner RA, Coda AB, et al. Injury enhances TLR2 function and antimicrobial peptide expression through a vitamin D-dependent mechanism. J Clin Invest. 2007;117(3):803–811.
- Steinhoff M, Schmelz M, Schauber J. Facial erythema of rosacea – aetiology, different pathophysiologies and treatment options. Acta Derm Venereol. 2016;96(5):579–586.
- Del Rosso JQ. Advances in understanding and managing rosacea: part 2: the central role, evaluation, and medical management of diffuse and persistent facial erythema of rosacea. J Clin Aesthet Dermatol. 2012;5(3): 26–36.
- Tanghetti E, Del Rosso JQ, Thiboutot D, et al. Consensus recommendations from the American acne & rosacea society on the management of rosacea, part 4: a status report on physical modalities and devices. Cutis. 2014;93(2):71–76.
- Guimaraes S, Moura D. Vascular adrenoceptors: an update. Pharmacol Rev. 2001;53(2): 319–356.
- Hsia E, Tian M, Gil D. Reduction in ultraviolet B light-induced erythema by oxymetazoline and brimonidine is mediated by different alpha-adrenoceptors. Exp Dermatol. 2018;27(7): 763–768.
- Tuettenberg A, Koelsch S, Knop J, Jonuleit H. Oxymetazoline modulates proinflammatory cytokines and the T-cell stimulatory capacity of dendritic cells. Exp Dermatol. 2007;16(3):171–178.
- Beck-Speier I, Dayal N, Karg E, et al. Oxymetazoline inhibits proinflammatory reactions: effect on arachidonic acid-derived metabolites. J Pharmacol Exp Ther. 2006;316(2):843–851.
- Beck-Speier I, Oswald B, Maier KL, et al. Oxymetazoline inhibits and resolves inflammatory reactions in human neutrophils. J Pharmacol Sci. 2009;110(3):276–284.
- Kang BY, Lee SW, Kim TS. Stimulation of interleukin-12 production in mouse macrophages via activation of p38 mitogen-activated protein kinase by alpha2-adrenoceptor agonists. Eur J Pharmacol. 2003;467(1–3):223–231.
- Lacoste A, De Cian MC, Cueff A, Poulet SA. Noradrenaline and alpha-adrenergic signaling induce the hsp70 gene promoter in mollusc immune cells. J Cell Sci. 2001;114(Pt 19):3557–3564.
- Sanders VM, Munson AE. Role of alpha adrenoceptor activation in modulating the murine primary antibody response in vitro. J Pharmacol Exp Ther. 1985;232(2):395–400.
- Heilig M, Irwin M, Grewal I, Sercarz E. Sympathetic regulation of T-helper cell function. Brain Behav Immun. 1993;7(2): 154–163.
- Kim M, Kim J, Jeong SW, Jo H, et al. Inhibition of mast cell infiltration in an LL-37-induced rosacea mouse model using topical brimonidine tartrate 0.33% gel. Exp Dermatol. 2017;26(11):1143–1145.
- Kusari J, Padillo E, Zhou SX, et al. Effect of brimonidine on retinal and choroidal neovascularization in a mouse model of retinopathy of prematurity and laser-treated rats. Invest Ophthalmol Vis Sci. 2011;52(8):5424–5431.
- Kusari J, Zhou SX, Padillo E, et al. Inhibition of vitreoretinal VEGF elevation and blood-retinal barrier breakdown in streptozotocin-induced diabetic rats by brimonidine. Invest Ophthalmol Vis Sci. 2010;51(2):1044–1051.
- Shanler SD, Ondo AL. Successful treatment of the erythema and flushing of rosacea using a topically applied selective alpha1-adrenergic receptor agonist, oxymetazoline. Arch Dermatol. 2007;143(11): 1369–1371.
- Consumer Healthcare Products Association. Ingredients & dosages transferred from Rx-to-OTC status (or new OTC approvals) by the Food and Drug Administration since 1975. Available at: https://www.chpa.org/sites/default/files/media/docs/2020-11/switch%20list%20updated%20November%202_2020.pdf. Accessed February 24, 2021.
- Kuang AW, duBois J, Attar M, Ahluwalia G. Clinical pharmacokinetics of oxymetazoline cream following topical facial administration for the treatment of erythema associated with rosacea. J Drugs Dermatol. 2018;17(2): 213–220.
- DuBois J, Dover JS, Jones TM, et al. Phase 2 randomized, dose-ranging study of oxymetazoline cream for treatment of persistent facial erythema associated with rosacea. J Drugs Dermatol. 2018;17(3):611–619.
- Kircik LH, DuBois J, Draelos ZD, et al. Pivotal trial of the efficacy and safety of oxymetazoline cream 1.0% for the treatment of persistent facial erythema associated with rosacea: findings from the first REVEAL trial. J Drugs Dermatol. 2018;17(1):97–105.
- Baumann L, Goldberg DJ, Stein-Gold L, et al. Pivotal trial of the efficacy and safety of oxymetazoline cream 1.0% for the treatment of persistent facial erythema associated with rosacea: findings from the second REVEAL trial. J Drugs Dermatol. 2018;17(3):611–619.
- Draelos ZD, Gold MH, Weiss RA, et al. Efficacy and safety of oxymetazoline cream 1.0% for treatment of persistent facial erythema associated with rosacea: findings from the 52-week open label REVEAL trial. J Am Acad Dermatol. 2018;78(6):1156–1163.
- Tanghetti EA, Goldberg DJ, Dover JS, et al. Oxymetazoline and energy-based therapy in patients with rosacea: evaluation of the safety and tolerability in an open-label, interventional study. Lasers Surg Med. 2020 May 6. Epub ahead of print.
- Del Rosso JQ. Topical alpha-agonist therapy for persistent facial erythema of rosacea and the addition of oxmetazoline to the treatment armamentarium: where are we now? J Clin Aesthet Dermatol. 2017;10(7):28–32.
- Mirvaso [package insert]. Fort Worth, TX: Galderma Laboratories; 2017.
- Tanghetti E, Dover JS, Goldberg DJ, et al. Clinically relevant reduction in persistent facial erythema of rosacea on the first day of treatment with oxymetazoline cream 1.0%. J Drugs Dermatol. 2018;17(6):621–626.
- Gold MH, Lebwohl M, Biesman BS, et al. Daily oxymetazoline cream demonstrates high and sustained efficacy in patients with persistent erythema of rosacea through 52 weeks of treatment. J Am Acad Dermatol. 2018;79(3):e57–e59.
- Eichenfield LF, Del Rosso JQ, Tan JKL, et al. Use of an alternative method to evaluate erythema severity in a clinical trial: difference in vehicle response with evaluation of baseline and postdose photographs for effect of oxymetazoline cream 1.0% for persistent erythema of rosacea in a phase 4 study. Br J Dermatol. 2019;180(5):1050–1057.
- Kelly A, Pai A, Lertsakdadet B, et al. Microvascular effects of pulsed dye laser in combination with oxymetazoline. Lasers Surg Med. 2020;52(1):17–22.
- Suggs AK, Macri A, Richmond H, et al. Treatment of erythematotelangiectatic rosacea with pulsed-dye laser and oxymetazoline 1.0% cream: a retrospective study. Lasers Surg Med. 2020;52(1):38–43.
- Gold LS, Papp K, Lynde C, et al. Treatment of rosacea with concomitant use of topical ivermectin 1% cream and brimonidine 0.33% gel: a randomized, vehicle-controlled study. J Drugs Dermatol. 2017;16(9):909–916.