
aJames Q. Del Rosso, DO, FAOCD, FAAD; bEmil A. Tanghetti, MD; cHilary E. Baldwin, MD; dDavid A. Rodriguez, MD; eIlia L. Ferrusi, PhD
aJDR Dermatology Research/Thomas Dermatology, Las Vegas, Nevada
bThe Center for Dermatology and Laser Surgery, Sacramento, California
cThe Acne Treatment and Research Center, Morristown, New Jersey
dDermatology Associates and Research, Coral Gables, Florida; eAllergan plc, Irvine, California
Disclosure: This study was sponsored by Allergan plc, Dublin, Ireland. Manuscript preparation and editorial assistance was provided to the authors by Michael L. Pucci, PhD, of Peloton Advantage, Parsippany, New Jersey, and was funded by Allergan plc. Neither honoraria nor other form of compensation were made to the authors for authorship or any other activities related to preparation or submission of this manuscript. Related to the subject area of rosacea, Dr. Del Rosso serves as a consultant, speaker, and researcher for Allergan, Bayer Dermatology, and Galderma.
Abstract
Objective: Evaluate patients’ perceptions of rosacea symptoms and treatments. Design: Cross-sectional, web-based survey conducted from May 8 to July 1, 2015. Setting: E-mail invitation. Participants: Male and female adults in the United States who self-reported having a physician’s diagnosis of rosacea. Measurements: Sociodemographic and clinical characteristics were collected for eligible respondents using the Self-Assessment of Rosacea Facial Redness scale and the Symptom Assessment for Rosacea Facial Bumps and Pimples questionnaire. Respondents were instructed how to differentiate erythematotelangiectatic rosacea and papulopustular rosacea. Use of different treatments and satisfaction with treatment were assessed, as were coping mechanisms. Results: More than 4,000 individuals responded and 600 completed the survey. The participants’ mean age was 51.7 years and more than 90 percent rated their rosacea severity as mild or moderate. Most practiced stress and/or anxiety management, used makeup to cover rosacea, used sun protection, and changed their exercise regimens to cope with rosacea flare-ups. Participants reported avoiding sun exposure, hot baths and saunas, and specific skin care products to circumvent potential rosacea flare-ups. More than half (55.7%) had used a prescribed topical agent for rosacea in the preceding month, and 26.3 percent had used a prescribed oral antibiotic. Fewer than half were satisfied with treatment outcomes. Conclusion: Despite the chronic nature of rosacea, participants commonly used prescription agents only to treat flare-ups and relied on sun protection and other avoidance mechanisms to reduce their frequency. Education is needed to communicate the long-term nature of rosacea and the need for continued treatment to maintain long-term control. J Clin Aesthet Dermatol. 2017;10(6):17–31.
Rosacea, which is characterized primarily by persistent centrofacial erythema, affects an estimated 16 million adults in the United States.[1–3] The most common subtype is erythematotelangiectatic rosacea (ETR; subtype 1), characterized by persistent centrofacial erythema, intermittent bouts of vasodilation (flushing), and the presence of telangiectasia.[1],[4] Papulopustular rosacea (PPR; subtype 2) is the second most common subtype, manifesting as transient, centrofacial papules or pustules.[1],[4] Rosacea, which is characterized primarily by persistent centrofacial erythema, affects an estimated 16 million adults in the United States.[1–3] The most common subtype is erythematotelangiectatic rosacea (ETR; subtype 1), characterized by persistent centrofacial erythema, intermittent bouts of vasodilation (flushing), and the presence of telangiectasia.[1],[4] Papulopustular rosacea (PPR; subtype 2) is the second most common subtype, manifesting as transient, centrofacial papules or pustules.[1],[4]
The pathophysiology of rosacea is not fully understood, but data support the primary involvement of two pathophysiologic components: 1) abnormality in innate immune detection and 2) neurovascular dysregulation. Triggering of these pathophysiologic mechanisms in rosacea-prone skin induces signaling in inflammatory cascades in response to certain stimuli that lead to specific clinical manifestations of rosacea.[2],[5-15] Vasodilation of facial vasculature, both acute and chronic, has been documented in rosacea, along with impairment of the stratum corneum permeability barrier.4–[6],[8],[9],[11],[16–19]
Various treatments for the management of PPR are approved in the United States, including topical metronidazole, topical azelaic acid, topical ivermectin, and oral doxycycline (modified 40mg once-daily formulation), which are all reported to have anti-inflammatory properties.[20],[21] Given the central role of persistent erythema across rosacea subtypes, developing treatments that are specifically aimed at reducing erythema is an important goal for effective management of the symptoms and psychosocial impact of rosacea.[7] Two topical pharmacologic agents currently approved in the United States for the treatment of persistent non-transient erythema of rosacea include brimonidine gel, an alpha-2 adrenergic receptor agonist vasoconstrictor,[22-24] and oxymetazoline cream, an alpha-1 adrenergic receptor agonist.[11],[25–27]
In addition to the characteristic physical discomfort associated with rosacea, such as burning, itching, and stinging,[28] the condition may also have a considerable adverse psychosocial impact on quality of life.[29] Negative effects on self-esteem and self-confidence have been documented.[29],[30] While available treatments are primarily targeted at managing the clinical signs and symptoms of rosacea, effective treatment can also reduce the psychosocial impact of rosacea.[31] However, although these treatments are effective, rosacea is a chronic disease that often requires ongoing management. Some patients may temporarily discontinue medication use because their signs and symptoms vary in severity over time, because they consider continuous treatment too costly or inconvenient, or because they consider potential or experienced side effects of treatments too burdensome, resulting in only intermittent therapy to treat flare-ups.[32]
To further investigate the burden that rosacea imposes on patients with the condition, a survey was conducted in the United States in adults with ETR and with PPR to evaluate the perception of rosacea signs and symptoms and available treatments. This analysis reports on the impact of rosacea on patients’ lives as well as their satisfaction with treatment.
Methods
This cross-sectional, web-based survey of adults with rosacea was conducted from May 8 to July 1, 2015. Respondents were screened for inclusion, and eligible respondents were invited to participate in a one-time web-based survey. The Chesapeake Institutional Review Board (Columbia, Maryland) approved the study protocol, and the study was conducted in accordance with regulatory guidelines and with requirements for studies involving human respondents. Study participants provided informed consent via a web-linked opt-in process before beginning the survey. United BioSource Corporation (Bluebell, Pennsylvania) monitored the conduct of the survey, which was administered by Ipsos Observer (Paris, France). Potential survey participants were identified by Ipsos Observer through their partnership with four companies utilizing established panels of volunteers who have agreed to participate in surveys. Panelists were not paid for their participation, but received incentives through loyalty programs with a low dollar value. Adult survey panelists who had been prescreened for rosacea received an invitation via e-mail to participate in this survey. The e-mail contained a hyperlink to the survey website, for those who wished to participate.
Participant eligibility. Prospective participants had completed an eligibility survey designed to identify those with current ETR or PPR. Eligible participants lived in the United States, were at least 18 years of age, and self-reported a physician’s diagnosis of rosacea at any time in the past. Participants were required to be able to read and understand English. Exclusion criteria included self-rated facial redness that was less than mild, based on the validated Self-Assessment of Rosacea Facial Redness (SA-RFR) photographic scale. Additionally, patients with telangiectasia (visible blood vessels) covering more than 25 percent of the area where rosacea occurs, sun-damaged skin (irregular coloring or pigmentation of the skin, with a mottled, wrinkled appearance, and “liver spots” or “age spots”) covering more than 25 percent of the face, or acne covering more than 25 percent of the face were excluded. Participants were requested to respond to the eligibility survey in a well-lit room, to remove any makeup or facial jewelry, and to use a mirror. They were also encouraged (but not required) to complete the survey in the evening, after having eaten a meal.
Participants who completed the survey and indicated the presence of at least mild facial redness were classified into an ETR or PPR cohort, based on having fewer than four or at least four inflammatory bumps or pimples, respectively, at the time of the survey. Participants were also categorized as having mild, moderate, or severe rosacea. In the ETR cohort, severity was assessed on the basis of facial redness alone using the SA-RFR scale as a photographic guide, while in the PPR cohort, severity was categorized based on the number of facial lesions alone. Subjects who indicated having 4 to 9 facial bumps or pimples were classified as having mild PPR, 10 to 20 as moderate PPR, and 21 or more as severe PPR. Facial redness severity was also assessed for participants in the PPR cohort.
Data collection. The survey included basic demographic questions, including sociodemographics, height and weight, type of medical insurance, and whether or not they had prescription drug coverage. Clinical characteristics, including age when rosacea signs and symptoms were first noticed, type of initial rosacea (ETR vs. PPR), bothersomeness of current symptoms, location of rosacea signs and symptoms, the presence of concomitant skin conditions, and the participant’s skin type, using the Fitzpatrick skin phototype scale, were also assessed.[33] Rosacea was assessed using the SA-RFR and the Symptom Assessment for Rosacea Facial Bumps and Pimples questionnaire, which was based on the SA-RFR. In addition, the survey included questions about coping and avoidance behaviors to prevent rosacea flare-ups, visits to healthcare professionals for their rosacea, use of prescription and over-the-counter (OTC) treatments, scenarios for the use of treatment, and satisfaction with treatment. Questions about treatment satisfaction included the collection of adverse event data. In cases where unwanted effects could be linked to a specific treatment or medication, they were reported to the drug manufacturer within 24 hours.
Statistical analysis. Descriptive statistics were reported for sociodemographics, survey metrics, burden of illness, treatment perceptions, and satisfaction with treatment for each cohort. Limited inferential analyses were conducted for key outcomes, with statistical significance for all comparisons set at p<0.01. For continuous variables, comparisons were conducted using the student t-test. For categorical outcomes, Pearson’s chi-square test was used for categories with expected cell size greater than 5, and Fisher’s exact test was used for categories with expected cell counts of 5 or less; for situations in which the participant was able to choose more than one response, a chi-square test was repeated for each response level. No adjustment was made to correct for multiple testing. Analyses were performed on the population of evaluable participants, which comprised eligible respondents who completed the survey in its entirety.
Results
Participants. A total of 4,174 individuals responded to the e-mail invitation and opt-out link, of whom 659 were eligible to participate; 600 participants completed the survey (Figure 1). Common reasons for ineligibility included having “no signs of unwanted redness,” being “almost clear of unwanted redness,” lack of a physician’s diagnosis, having telangiectasia covering more than 25 percent of the rosacea-affected areas, or having sun-damaged skin covering more than 25 percent of the face. Of the eligible subjects completing the survey, 409 were included in the ETR cohort and 191 in the PPR cohort.
{kind=link}
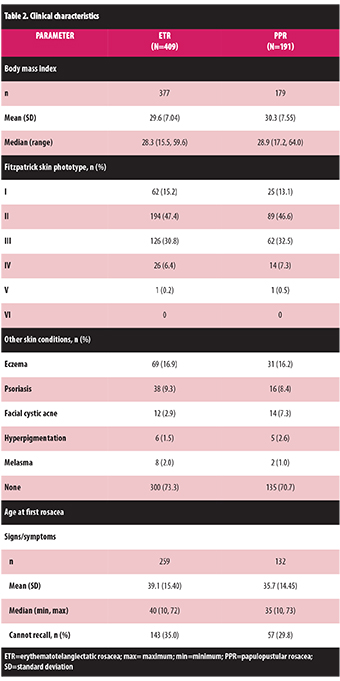
Sociodemographics are shown in Table 1 . The mean age was 51.7 (standard deviation, 13.91) years, with participants in the PPR cohort approximately 4.4 years older on average than those in the ETR cohort (p=0.0003). More than half (69.5%) of participants were female and more than 95 percent were Caucasian. Participants in the PPR cohort had significantly less prescription drug coverage and private medical insurance than those in the ETR cohort (p=0.003). Clinical characteristics of the participants are shown in Table 2. Ninety-three percent of participants had a Fitzpatrick skin phototype of I, II, or III. The most common concomitant skin conditions were eczema and psoriasis, which were reported by 16.7 percent and 9.0 percent of all participants, respectively; 72.5 percent had no other skin condition. Among participants who could recall, they first noticed rosacea signs and symptoms at a mean age of 37.9 years. For eligible participants, a mean of 9.3 years elapsed between diagnosis and screening. Patients in both cohorts gave similar severity ratings; 95.6 percent (391/409) of participants in the ETR cohort and 93.7 percent (179/191) in the PPR cohort rated their rosacea as mild or moderate. Only 8.9 percent of participants could recall the clinical rosacea subtype with which they were diagnosed.
{kind=link}
{kind=link}
Rosacea symptoms. The predominant initial rosacea sign and/or symptom in both cohorts was persistent facial redness, reported by 71.5 percent of participants (Figure 2A). As expected, significantly more participants in the PPR cohort reported bumps or pimples as the initial rosacea symptom than those in the ETR cohort (p<0.0001). Temporary facial blushing and/or flushing were reported by approximately half of the participants in both cohorts.
{kind=link}
The most bothersome clinical manifestations at the time of the survey were blushing and/or flushing in the ETR cohort, which was significantly greater than that reported by participants in the PPR cohort (p=0.0001; Figure 2B). In the PPR cohort, the most common bothersome clinical manifestations were facial bumps and/or pimples, reported by a significantly greater proportion of participants versus the ETR cohort (p<0.0001). Burning and/or stinging skin, skin thickening, and skin swelling were also more common in the PPR cohort.
{kind=link}
Findings for the SA-RFR and for the Symptom Assessment for Rosacea Facial Bumps and Pimples questionnaire are shown in Supplementary Figure S1. Almost all participants in both cohorts characterized facial redness as “somewhat red” or “a little red”; similarly, almost all participants in both cohorts described the amount of their face that was red because of rosacea as “some of my face” or “a little of my face.” While 48.7 percent of participants in the ETR cohort reported that their face felt at least a little warm because of facial redness, a greater, although not significantly greater, proportion of participants in the PPR cohort (60.7%; p=0.0107) reported that their faces were a little to very warm because of rosacea facial redness. Significantly more patients in the PPR cohort indicated that at least “a little of my face” burned because of rosacea, with 29.8 percent in the PPR cohort and 13.2 percent in the ETR cohort reporting that “a little of my face,” “some of my face,” “quite a bit of my face,” or “a lot of my face” burned because of rosacea (p<0.001). In both cohorts, facial redness occurred predominantly in the cheeks, followed by the nose. While most of the participants in the PPR cohort reported having “a few” or “some” facial bumps or pimples, only 11.5 percent reported having more than a few bumps or pimples with pus. The main locations of bumps and pimples were the cheeks, forehead, nose, and chin.
Coping and avoidance behaviors. The majority of participants in both the ETR and PPR cohorts indicated that they practiced stress and/or anxiety management and used makeup to cover rosacea, and at least half of participants in each cohort reported that they changed their exercise regimens to cope with rosacea flare-ups (Figure 3A). The majority of all participants also avoided sun exposure, hot baths and/or saunas, certain skin care products, hot beverages, and alcohol (Figure 3B). Significantly more subjects in the PPR cohort avoided specific skin care products than did those in the ETR cohort (p=0.0011). This was also true of avoiding specific foods (p=0.0073).
{kind=link}
{kind=link}
Rosacea treatment. In the ETR and PPR cohorts, respectively, 20.3 percent and 24.1 percent reported having seen a healthcare provider for the assessment and/or treatment of rosacea during the preceding three months. For those participants reporting such visits to one or more providers, 76.7 percent had seen a dermatologist, 32.6 percent had gone to their primary care physician, 10.9 percent had seen a nurse practitioner or physician’s assistant, and 15.5 percent had talked with a pharmacist.
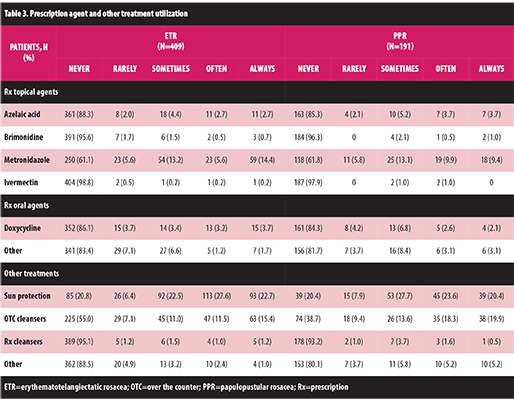
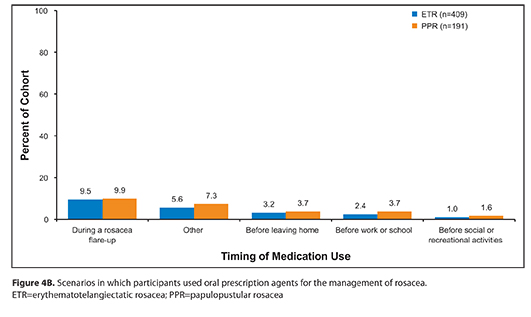
Treatment utilization patterns for topical and oral prescription agents did not differ significantly between the ETR and PPR cohorts (Table 3). More than half (55.7%) of the participants had used a prescribed topical agent for rosacea in the preceding month, and 26.3 percent had used a prescribed oral antibiotic. Metronidazole was the most commonly used topical agent, being used sometimes, often, or always by 33.3 percent of the ETR cohort and by 32.5 percent of the PPR cohort. The most common scenario for the use of a topical prescription agent or an oral antibiotic was to manage a rosacea flare-up (Figure 4A and Figure 4B). Other commonly used treatments included sun protection, used by 79.2 percent and 79.6 percent of participants in the ETR and PPR cohorts, respectively, and non-prescription facial cleansers, used by 45.0 percent in the ETR cohort and 61.3 percent in the PPR cohort (p=0.0057) (Table 3).
{kind=link}
{kind=link}
{kind=link}
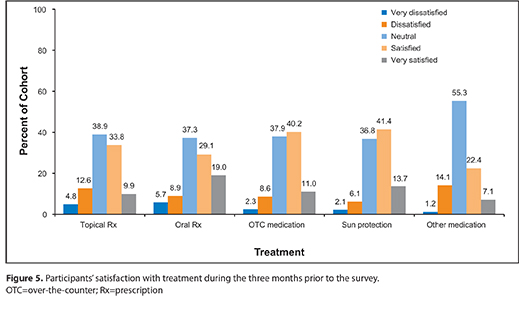
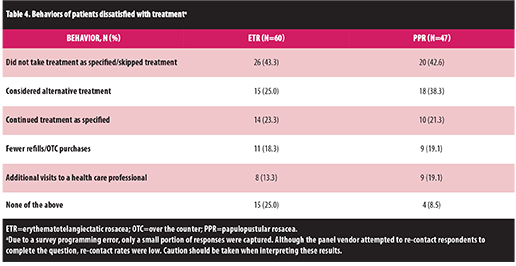
Fewer than half of participants were satisfied with their prescription treatments, and slightly more than half were satisfied with OTC agents. The proportion of those who were satisfied or very satisfied with topical prescription treatments was 43.7 percent, with oral antibiotics was 48.1 percent, and with OTC agents was 51.2 percent (Figure 5). For those participants who reported being dissatisfied or very dissatisfied with one or more of their treatments, the most common reasons for dissatisfaction were that the agent did not meet the respondent’s expectations for treatment of signs or symptoms, that the treatment was too expensive, and that it took too long to achieve noticeable results. Dissatisfaction commonly resulted in participants not using the treatment as specified or skipping treatment (43.0%) (Table 4).
{kind=link}
{kind=link}
Discussion
The results of this survey indicate that there is a considerable burden of illness associated with rosacea, despite the survey participants with ETR and PPR reporting that the severity of their rosacea was mild or moderate. Participants reported a variety of bothersome rosacea-associated signs, including facial erythema and telangiectasia, and symptoms, such as cutaneous burning and/or stinging (in both the ETR and PPR cohorts), and papules and pustules (primarily in the PPR cohort). This array of bothersome clinical manifestations was in line with the classical definitions for ETR and PPR.[4] To manage these signs and symptoms during rosacea flare-ups, participants employed an array of coping and avoidance mechanisms, including stress management, changing exercise regimens, and avoiding sun exposure, hot baths/saunas, and certain skin products.
Treatment utilization findings suggest limited use of topical and oral prescription agents, especially for long-term management to reduce exacerbations. Rather, most respondents reported reliance on sun protection. The most commonly used prescription agent was topical metronidazole, which was used by 33 percent of participants. Overall, the use of prescription agents was low, with most participants reporting no use within the previous month of metronidazole, azelaic acid, brimonidine, ivermectin, doxycycline, or other oral agents, or of prescription topical cleansers. The limited and perhaps inconsistent use of these prescription agents may be attributable to the perceptions of many patients of poor long-term efficacy in the real-world management of rosacea, since only about half of the participants who reported using them were satisfied or very satisfied with these treatments. By contrast, participants indicated a high rate of sun protection usage, which is in line with rosacea management guidelines and recommendations.[1],[2]
The most common usage of prescription treatments among the study participants was to treat a rosacea flare up. It is difficult to discern from these data whether the patients actually used their prescription medication for a sufficient period of time to result in the expected outcome. The chronic nature of rosacea often necessitates the use of a continued therapeutic regimen once remission is achieved in order to sustain effective control of the disorder.[20],[34-36] The low levels of treatment satisfaction reported in this study contrast with much higher treatment satisfaction results, such as those reported immediately following four weeks of treatment with doxycycline.[37] Taken together, these results suggest that prescription treatments are effective, but are not consistently used. Consequently, there is a need for patient education about the chronic nature of rosacea and the necessity for continued maintenance treatment to achieve optimal outcomes. This may help to set reasonable expectations for treatment success.[20],[31] Implementation of such a patient education program may result in increased utilization of prescription treatments, which could be expected to improve satisfaction with treatment.
This study is unique in that it obtained a wide range of data from a single, large cohort of adults with rosacea. It should be noted, however, that the results should be interpreted in the context of certain study limitations. This cohort tended to be better educated and had a higher median income than most Americans. In the Current Population Survey conducted by the US Census Bureau in 2015, 58.9 percent of individuals reported having at least some college education38; in the current survey, more than 90 percent reported education beyond a high school diploma. The percentage of individuals with household income below $50,000, between $50,000 and $99,999, and $100,000 or above was 46.8 percent, 28.5 percent, and 24.7 percent, respectively, in the US 2014 Current Population Reports[39] and was 29.5 percent, 34.9 percent, and 29.2 percent in the current study, with 6.5 percent not reporting income. Although the reasons for these differences have not been determined, they could possibly be attributable to selection bias that may have been introduced by the web-based recruitment methodology.[38],[40] It is possible that responses in this study may not be comparable to responses collected using paper questionnaires. However, the sociodemographic characteristics of the population were consistent with previously published data on patients with rosacea.[38],[40],[41] In agreement with these prior studies, this study included survey respondents typically aged in their early 50s who first noticed signs and symptoms of rosacea in their mid-30s.[41] In the current study, the ETR cohort was predominantly female, while the PPR population was predominantly male, again in line with previously reported observations.[41]
Internet-based methodology is attractive because it allows for the rapid collection of data from a large cohort of individuals. This web-based survey allowed for a comprehensive assessment of the overall burden of illness for those with ETR and PPR. However, one limitation to this approach is the reliance on self-reported data. While of value, participant assessments may differ from those of experienced medical professionals involved in clinical studies. This may be particularly important when considering the psychosocial effects of rosacea, which do not necessarily correlate with the severity of the disease.[42] Although this survey was large, most participants reported having only mild or moderate disease severity, resulting in a low number of patients with severe ETR and PPR. Another limitation of this type of study is that it collects response data during a narrow window of the participants’ experience with rosacea. This necessarily restricted responses regarding participants’ usage and experience with rosacea treatments. In addition, it is possible that some PPR patients may have had rosacea that was adequately controlled by topical metronidazole treatment so did not present with more than four papules at the time of the survey. As a result, it is possible that a number of controlled PPR patients were included in the ETR cohort. This potential discrepancy may have had an effect on the comparisons between the ETR and PPR cohorts.
Conclusion
This cross-sectional, survey-based study obtained a wide range of data on individuals with ETR and PPR. Not surprisingly, rosacea signs and symptoms were bothersome to study participants. Yet, despite the chronic nature of the condition, they commonly used prescription agents only to treat rosacea flare-ups and relied instead on sun protection and other avoidance mechanisms to manage their rosacea on a long-term basis. Many participants were not using their prescription therapies, and among those who did, many were not satisfied with the results. Individuals with rosacea are likely to benefit from more education about the different clinical manifestations of rosacea, its chronic and recurrent nature, the need for long-term treatment to decrease the frequency and severity of flare-ups, and the importance of setting reasonable expectations for treatment success.
References
1. Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 1: a status report on the disease state, general measures, and adjunctive skin care. Cutis. 2013;92(5):234–240.
2. Baldwin HE. Diagnosis and treatment of rosacea: state of the art. J Drugs Dermatol. 2012;11(6):725–730.
3. National Rosacea Society. Rosacea riddle now threatens more than 16 million Americans [press release]. 2010. http://www.rosacea.org/ press/archive/20100401.php. Accessed on March 9, 2016.
4. Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol. 2002;46(4):584–587.
5. Steinhoff M, Buddenkotte J, Aubert J, et al. Clinical, cellular, and molecular aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011;15(1):2–11.
6. Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007;13(8):975–980.
7. Del Rosso JQ. Advances in understanding and managing rosacea: part 2: the central role, evaluation, and medical management of diffuse and persistent facial erythema of rosacea. J Clin Aesthet Dermatol. 2012;5(3):26–36.
8. Del Rosso JQ. Advances in understanding and managing rosacea: part 1: connecting the dots between pathophysiological mechanisms and common clinical features of rosacea with emphasis on vascular changes and facial erythema. J Clin Aesthet Dermatol. 2012;5(3):16–25.
9. Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77–81.
10. Fleischer AB Jr. Inflammation in rosacea and acne: implications for patient care. J Drugs Dermatol. 2011;10(6):614–620.
11. Del Rosso JQ, Gallo RL, Kircik L, et al. Why is rosacea considered to be an inflammatory disorder? The primary role, clinical relevance, and therapeutic correlations of abnormal innate immune response in rosacea-prone skin. J Drugs Dermatol. 2012;11(6):694–700.
12. Dahl MV, Ross AJ, Schlievert PM. Temperature regulates bacterial protein production: possible role in rosacea. J Am Acad Dermatol. 2004;50(2):266–272.
13. Jarmuda S, O’Reilly N, Zaba R, et al. Potential role of Demodex mites and bacteria in the induction of rosacea. J Med Microbiol. 2012;61(Pt 11):1504–1510.
14. Bevins CL, Liu FT. Rosacea: skin innate immunity gone awry? Nat Med. 2007;13(8):904–906.
15. Egeberg A, Hansen PR, Gislason GH, Thyssen JP. Patients with rosacea have increased risk of dementia. Ann Neurol. 2016;79(6):921–928.
16. Crawford GH, Pelle MT, James WD. Rosacea: I. Etiology, pathogenesis, and subtype classification. J Am Acad Dermatol. 2004;51(3):327–341; quiz 342–324.
17. Guzman-Sanchez DA, Ishiuji Y, Patel T, et al. Enhanced skin blood flow and sensitivity to noxious heat stimuli in papulopustular rosacea. J Am Acad Dermatol. 2007;57(5):800–805.
18. Rosina P, Zamperetti MR, Giovannini A, et al. Videocapillaroscopic alterations in erythematotelangiectatic rosacea. J Am Acad Dermatol. 2006;54(1):100–104.
19. Dirschka T, Tronnier H, Folster-Holst R. Epithelial barrier function and atopic diathesis in rosacea and perioral dermatitis. Br J Dermatol. 2004;150(6):1136–1141.
20. Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 5: a guide on the management of rosacea. Cutis. 2014;93(3):134–138.
21. Cardwell LA, Alinia H, Moradi Tuchayi S, Feldman SR. New developments in the treatment of rosacea—role of once-daily ivermectin cream. Clin Cosmet Investig Dermatol. 2016;9:71–77.
22. Fowler J Jr, Jackson M, Moore A, et al. Efficacy and safety of once-daily topical brimonidine tartrate gel 0.5% for the treatment of moderate to severe facial erythema of rosacea: results of two randomized, double-blind, and vehicle-controlled pivotal studies. J Drugs Dermatol. 2013;12(6):650–656.
23. Jackson JM, Fowler J, Moore A, et al. Improvement in facial erythema within 30 minutes of initial application of brimonidine tartrate in patients with rosacea. J Drugs Dermatol. 2014;13(6):699–704.
24. Mirvaso [package insert]. Fort Worth, TX: Galderma Laboratories; 2016.
25. Rhofade [package insert]. Irvine, CA: Allergan; 2017.
26. Gold LM, Draelos ZD. New and emerging treatments for rosacea. Am J Clin Dermatol. 2015;16(6):457–461.
27. Chang BP, Kurian A, Barankin B. Rosacea: an update on medical therapies. Skin Therapy Lett. 2014;19(3):1–4.
28. Drake L. Survey shows physical discomfort with visible signs of rosacea. Rosacea Review 2012. http://rosacea.org/rr/2012/summer/article_3.php. Accessed on March 9, 2016.
29. van der Linden MM, van Rappard DC, Daams JG, et al. Health-related quality of life in patients with cutaneous rosacea: a systematic review. Acta Derm Venereol. 2015;95(4):395–400.
30. Drake L. Survey shows rosacea’s emotional toll, positive effects of medical therapy. 2007. http://www. rosacea.org/rr/2007/spring/article_3.php. Accessed on March 9, 2016.
31. Huynh TT. Burden of disease: the psychosocial impact of rosacea on a patient’s quality of life. Am Health Drug Benefits. 2013;6(6):348–354.
32. Elewski BE. Results of a national rosacea patient survey: common issues that concern rosacea sufferers. J Drugs Dermatol. 2009;8(2):120–123.
33. Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124(6):869–871.
34. Powell FC. Rosacea. N Engl J Med. 2005;352(8):793–803.
35. Dahl MV, Katz HI, Krueger GG, et al. Topical metronidazole maintains remissions of rosacea. Arch Dermatol. 1998;134(6):679–683.
36. Thiboutot DM, Fleischer AB, Del Rosso JQ, Rich P. A multicenter study of topical azelaic acid 15% gel in combination with oral doxycycline as initial therapy and azelaic acid 15% gel as maintenance monotherapy. J Drugs Dermatol. 2009;8(7):639–648.
37. Johnson SM, LeVine P. Self-reported treatment impressions and satisfaction of papulopustular rosacea patients treated with doxycycline, USP, 40mg capsules. J Drugs Dermatol. 2011;10(12):1376–1381.
38. Ryan CL, Bauman K. Educational attainment in the United States: 2015. 2016. https://www.census.gov/content/dam/Census/library/publications/2016/demo/p20–578.pdf. Accessed on April 12, 2016.
39. DeNavas-Walt C, Proctor BD, U.S. Census Bureau. Income and Poverty in the United States: 2014. Current Population Reports, P60–252. Washington, DC: U.S. Government Printing Office; 2015.
40. Table H-1. Income limits for each fifth and top 5 percent of all households: 1967 to 2014. 2015. https://www.census.gov/hhes/www/income/data/historical/household/. Accessed on April 12, 2016.
41. Chosidow O, Cribier B. Epidemiology of rosacea: updated data. Ann Dermatol Venereol. 2011;138(Suppl 3):S179–S183.
42. Bohm D, Schwanitz P, Stock GS, et al. Symptom severity and psychological sequelae in rosacea: results of a survey. Psychol Health Med. 2014;19(5):586–591.