 J Clin Aesthet Dermatol. 2022;15(10):32–35.
J Clin Aesthet Dermatol. 2022;15(10):32–35.
by Pablo Naranjo, MD, PhD; Mar Llamas, MD; Hen Ifrach, MD; and Rodolfo Andrino, MD
Drs. Naranjo, Llamas and Andrino are with Elite Laser Clinic in Madrid, Spain. Dr. Ifrach is with Hen Ifrach Aesthetic Surgery in Milano, Italy.
ABSTRACT: Background. Non-ablative fractional laser treatments for improving skin tone and rejuvenation have become increasingly popular due to short downtime and fewer side effects compared to ablative treatments.
Objective: We sought to determine the efficacy of a non-ablative 1540-nm fractional erbium: glass laser in improving skin roughness and skin texture.
Methods. The forehead, cheek, and nasal areas of 15 patients were treated for five monthly sessions using a 7×7 pixel tip (1.21cm2 affective area, approximately 300 microns diameter per pixel), fluence of 2,500 to 3,000 mJ/pulse (40–62 mJ/Pixel), and three stacked pulses were emitted at a rate of 1Hz for three passes per treatment session. Measurements of skin roughness, skin roughness area, and maximum skin depth were collected using a 3D imaging system. Improvement in skin parameters was calculated by comparing the measurements prior to treatment and 12 weeks after completion.
Results. All 15 patients showed significant improvement in all three measured parameters (p<0.001) with no significant side effects.
Limitations. The limitations of this study include the small number of patients and the narrow range of skin tone (Fitzpatrick Skin Types II–IV).
Conclusion. Our results suggest that monthly treatments with a non-ablative 1540-nm fractional Erbium:glass laser appear to be safe and effective for skin texture and roughness.
Keywords. Non-ablative fractional laser, skin roughness, skin texture, skin 3D imaging, 1540-nm fractional Erbium:glass laser
One of the major hallmarks of skin aging is a reduction in collagen integrity and a decrease in new collagen formation.1 Lasers have been introduced into aesthetic dermatology procedures for the purpose of skin resurfacing or remodeling and are largely divided into fractional or non-fractional and ablative or non-ablative. The original ablative non-fractional lasers vaporize the dermis and induce collagen formation but have severe side effects, including scarring and significant recovery periods.2 The incorporation of fractional lasers led to the development of the non-ablative fractional laser (NAFL), which entered the market in 20052, and the ablative fractional laser (AFXL), introduced in 2007.2 Collagen and elastin remodeling, both components of the extracellular matrix, can be induced by both NAFLs and AFXLs.3 While AFXLs heat and physically wound the skin, thereby ablating the epidermis, NAFLs apply focused thermal damage, keeping the epidermis intact.4 Therefore, the NAFLs are less painful and result in shorter recovery times. Mid-infrared wavelength NAFLs generate vertical columns of microscopic thermal damage while leaving the intervening skin untouched. Clinical and histologic studies have shown that NAFLs significantly induce new collagen formation, leading to long-lasting improvements in skin tightness and appearance.5–10
NAFLs have been used to treat various skin ailments including periorbital wrinkling,11 striae,12,13 acne scars,14–18 inflammatory acne,19 and skin resurfacing.20 The Food and Drug Administration (FDA) has approved the use of NAFLs to treat pigmented lesions, periorbital rhytides, skin resurfacing, melasma and soft tissue coagulation, acne and surgical scars, and actinic keratosis.21 NAFLs are gaining popularity since they are relatively gentle, have few side effects, a short downtime, and are effective on more skin types.2
This retrospective study analyzed the effect of the non-ablative 1540-nm fractional Erbium:glass laser on skin tone and texture by measuring skin roughness and maximum depth depression.
Methods
Patients. This was a retrospective evaluation of 15 patients. Patients (10 female, 5 male) were 34 to 49 years old (average=42.7 years) and had Fitzpatrick Skin Types II–IV. We excluded patients as following: (a) previously undergone a surgical facelift; (b) previously treated with ablative laser up to one year prior to treatment; (c) previously treated with any laser device up to three months prior to treatment; and (d) applied any topical treatment up to 14 days prior to treatment. Additional exclusion criteria were according to the recommendation of the manufacturer, such as pregnancy, history of facial skin cancer, and others.
Treatment. Treatments were conducted at the Elite Laser Clinic in Madrid, Spain, by a single physician. Patients were treated with a high power, high fluence 1540-nm fractional Erbium:glass laser (ClearSkin Pro, Alma Lasers LTD) every four weeks for a total of five sessions. Column size of the treated skin is estimated to be up to 1000 microns deep and 400 microns wide (unpublished data). Treatment area, including the cheek, forehead, and nasal area, was disinfected prior to each treatment and treated with topical anesthesia (lidocaine 6% + tetracaine 6%) for 45 minutes. Protective eyewear was utilized during treatments. Laser was applied using a 7*7 pixel tip (1.21cm2 affective area, 300 microns diameter per pixel), fluence of 2500-3000 mJ/pulse (40-62 mJ/Pixel), and three stacked pulses were emitted at a rate of 1Hz for three passes per treatment session. The above laser protocol has been shown to be effective in reducing rhytids’ appearance with no adverse effects.20
Outcome quantification. Quantification of skin texture was done using ANTERA 3D® imaging system and software (Miravex, Ireland) which relies on multidirectional illumination obtained by LEDs of different wavelengths from different directions. It allows visual ratings of mean pore volume, mean pore area, and max depth, especially for the small and medium filters22 and has been verified as accurate for wrinkle and roughness measurements23,24 and measuring the volume of pore and acne scars.25 In this study, average roughness volume, roughness affected area, and maximum depth depression measurements were obtained. Average roughness volume is the average dimension (three dimensional) of the micro-relief23 skin depression measured in mm3. Roughness affected area is the roughness portion of the measured skin area (two dimensional, measured in mm2). Maximum depth depression is the maximal depth measured within the area measured in mm. Improvement was calculated as the percent change between the images taken prior to treatments and 12 weeks after the final treatment. Paired student t-test was used to test the significance of measurement improvement.
Results
Fifteen patients, ten females and five males, ages 36–49, mean age 42.7±5, were included in this study (Table 1). All patients were categorized as Fitzpatrick Skin Type II (n=2), III (n=8), or IV (n=2). All 15 patients showed improvement in the three measured parameters: average roughness volume (mm3), roughness affected area (mm2), and maximum depth depression (mm). 49.5 percent reduction in the roughness volume; from 4.7±0.9 mm3 to 2.6±0.6mm3, (p<0.001, Figure 1). Fourty-six percent reduction in the roughness affected area; from 146.5±23.5mm2 to 86.8±17.5 mm2, (p<0.001, Figure 2). 24.6 percent reduction in the maximum depth depression; from 0.09±0.01mm to 0.06±0.007mm, (p<0.001, Figure 3). Statistical analysis was performed using MedCalc statistical software (version 19.4.1), by 2-tailed paired t-test tests, a p-value of <0.05 or less was considered statistically significant. Results are presented as Average±SEM. Downtime was 24 to 48 hours for all patients in all five treatments and no serious side effects were noted.



Discussion
Laser treatments to improve skin tone and quality have become increasingly popular. Fractionated lasers are categorized as either ablative (AFXL) or non-ablative (NAFL), both of which induce neocollagenesis.3 AFXL laser treatment shows significant improvements in treating photoaging, wrinkles, and scarring.26 However, ablative skin resurfacing is associated with prolonged recovery times (up to 3 months), potential scarring and dyspigmentation, pain, and discomfort.2,26 On the other hand, NAFLs have fewer side effects and a shorter downtime, usually hours to days.2,4 The treatment described herein has a downtime of 24 to 48 hours, compared to the 3 to 7 days following AFXL treatment.2 However, since NAFLs are much gentler than AFXLs, results may be milder and require several treatments for optimal outcomes. Here, we show that the 1540-nm fractional Erbium:glass NAFL efficiently improves skin texture in both male and female patients following five monthly treatments, and lasts up to three months post procedure.
AFXL lasers exert significant thermal damage to the epidermis, leading to ablation and wounding. NAFL treats the skin in small segments, creating microscopic treatment zones (MTZ) or microscopic ablation zones (MAZ)4 which can be seen in Figure 4. The immediate effect is of MTZ reaching up to 1000μm deep (Figure 4A) in which a wound-healing response is initiated, resulting in neocollagenesis and reorganization of elastin fibers. Epidermis will crust and heal within up to 72 hours (Figure 4B) and be completely unnoticeable within seven days post treatment, presenting a completely intact epidermis (Figure 4C). While both AFXL and NAFL treatments induce collagen and elastin turnover, one ablative treatment will produce similar collagen related histological results as will 3 to 5 non-ablative treatments. However, the significantly fewer side effects, shorter down-time, and lower associated pain of NAFL will often make it the preferred choice.

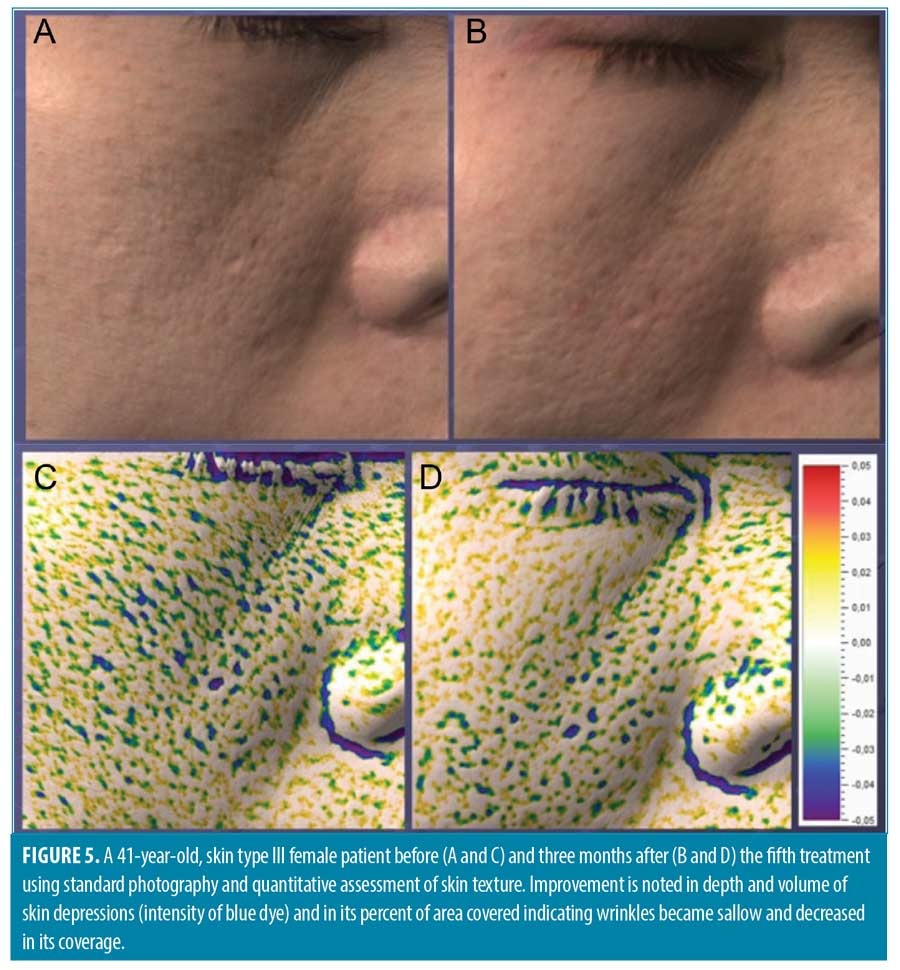
Laser treatment outcomes were measured using an imaging module, which has been verified for accuracy in quantifying pore volume25 and skin roughness.23,24 Treatment efficacy was calculated by comparing skin roughness and depth depression before the treatments and 12 weeks after the final treatment. Using the measurements of the imaging system, as compared to photo evaluations, eliminates human error and provides quantitative parameters for analyses (Figure 5). Indeed, treatment with a 1540-nm fractional Erbium:glass laser significantly improved roughness area and volume by approximately 50 percent and depth depression by 25 percent. Treatment was equally efficacious in both genders.
Conclusion
The data provided shows that the 1540-nm fractional Erbium:glass laser non-ablative fractional laser is safe and efficient in improving skin tone. Longer follow-ups are required to assess the treatment’s long-term benefits.
References
- Kohl E, Steinbauer J, Landthaler M, et al. Skin ageing. J Eur Acad Dermatol Venereol. 25(8). 2011 Aug; 873–884.
- Preissig J, Hamilton K, Markus R. Current laser resurfacing technologies: A review that delves beneath the surface. Seminars in Plastic Surgery. 2012 Aug;26(3):109–116.
- Paasch U and Said T. Stimulation of collagen and elastin production in-vivo using 1,540 nm Er:Glass laser: assessment of safety and efficacy. Journal of Cosmetic and Laser Therapy. 2020 Feb;22(2):77–83.
- Goldberg DJ. Lasers for facial rejuvenation. American Journal of Clinical Dermatology. 2003;4(4): 225–234.
- Hong JS et al. Long pulsed 1064 nm Nd:YAG laser treatment for wrinkle reduction and skin laxity: Evaluation of new parameters. International Journal of Dermatology. 2015 Sep;54(9): e345–e350.
- Goldberg DJ. Non-ablative subsurface remodeling: Clinical and histologic evaluation of a 1320-nm Nd:YAG lase. Journal of Cosmetic and Laser Therapy. 1999;1(3):153–157
- Tanzi EL, Williams CM, Alster, TS. Treatment of facial rhytides with a nonablative 1,450-nm diode laser: A controlled clinical and histologic study. Dermatologic Surgery. 2003 Feb;29(2): 124–128
- Fournier N et al. Nonablative remodeling: A 14-month clinical ultrasound imaging and profilometric evaluation of a 1540 nm Er:glass laser. Dermatologic Surgery. 2002 Oct;28(10): 926–931.
- Fournier N, et al. Nonablative remodeling: Clinical, histologic, ultrasound imaging, and profilometric evaluation of a 1540 nm Er:glass laser. Dermatologic Surgery. 2001;27(9): 799–806.
- Jung JY, Cho SB, Chung HJ, et al. Treatment of periorbital wrinkles with 1550- and 1565-nm Er:glass fractional photothermolysis lasers: A simultaneous split-face trial. Journal of the European Academy of Dermatology and Venereology. 2011 Jul;25(7):811–818.
- Horovitz T, Clementoni MT, Artzi O. Nonablative laser skin resurfacing for periorbital wrinkling—A case series of 16 patients. Journal of Cosmetic Dermatology. 2021 Jan;20(1):99–104.
- Wang K, Ross N, Osley K, et al. Evaluation of a 1540-nm and a 1410-nm nonablative fractionated laser for the treatment of striae. Dermatologic Surgery. 2016;42(2):225–231.
- Yang YJ and Lee GY. Treatment of Striae Distensae with Nonablative Fractional Laser versus Ablative CO2 Fractional Laser: A Randomized Controlled Trial. Annals of dermatology. 2011 Nov;23(4):481–489.
- Politi Y, Levi A, Enk CD, et al. Integrated cooling-vacuum-assisted 1540-nm erbium:glass laser is effective in treating mild-to-moderate acne vulgaris. Lasers in Medical Science. 2015 Dec;30(9):2389–2393.
- Chrastil B, Glaich AS, Goldberg LH, et al. Second-generation 1,550-nm fractional photothermolysis for the treatment of acne scars. Dermatologic Surgery. 2008 Oct;34(10):1327–1332
- Hedelund L, Moreau KER, Beyer DM, et al. Fractional nonablative 1,540-nm laser resurfacing of atrophic acne scars. A randomized controlled trial with blinded response evaluation. Lasers in Medical Science. 2010 Sep;25(5): 749–754
- Chae WS, et al. Comparative study on efficacy and safety of 1550 nm Er: Glass fractional laser and fractional radiofrequency microneedle device for facial atrophic acne scar. Journal of Cosmetic Dermatology. 2015 Jun;14(2): 100–106.
- Politi Y, Levi A, Lapidoth M. Integrated cooling-vacuum-assisted non-fractional 1540 nm erbium: Glass laser is effective in treating acne scars. Journal of Drugs in Dermatology. 2016 Nov;15(11): 1359–1363,
- Bogle MA, Dover, JS, Arndt KA, et al. Evaluation of the 1,540-nm erbium:glass laser in the treatment of inflammatory facial acne. Dermatologic Surgery. 2007 Jun;33(7): 810–817.
- Solomon-Cohen E, et al. 1540-nm fractional erbium: Glass laser is a safe and effective modality for nonablative facial rejuvenation. Journal of Cosmetic Dermatology. 2021 Jun;20(6):1679–1683.
- Allemann IB and Kaufman J. Fractional photothermolysis. Current Problems in Dermatology. Aug 2011;42: 56–66.
- Messaraa et al. Antera 3D capabilities for pore measurements. Skin Research and Technology. 2018 Nov;24(4): 606–613.
- Messaraa C et al. Wrinkle and roughness measurement by the Antera 3D and its application for evaluation of cosmetic products. Skin Research and Technology. 2018 Aug;24(3): 359–366.
- Linming F et al. Comparison of two skin imaging analysis instruments: The VISIA® from Canfield vs the ANTERA 3D®CS from Miravex. Skin Research and Technology. 2018 Feb;24(1): 3–8.
- Park CS, Park JH, Kim CR, Lee JH. Objective analysis of volume restoration in atrophic acne scars and skin pores: a split study using human stem cell-conditioned media. Journal of Dermatological Treatment. 2021;32(1): 73–77
- Verma N, Yumeen S, Raggio BS. Ablative Laser Resurfacing. 2021.