J Clin Aesthet Dermatol. 2025;18(7):35–39.
by Xinge Diana Zhang, PhD; Xuefei Sophie Bai, MBA; Claudia Teng, BA; Suneel Chilukuri, MD, FAAD; Joyce Teng, MD, PhD, FAAD; Glynis Ablon, MD, FAAD; and Michael H. Gold, MD, FAAD
Dr. Zhang and Mses. Bai and Teng are with B.A.I. Biosciences, Inc. in Cambridge, Massachusetts. Dr. Chilukuri is with Refresh Dermatology in Houston, Texas, and the Baylor College of Medicine in Houston, Texas. Dr. Teng is with the Department of Dermatology at Stanford University School of Medicine in Stanford, California. Dr. Ablon is with the Ablon Skin Institute and Research Center in Manhattan Beach, California, and the Department of Dermatology at the University of California, Los Angeles in Los Angeles, California. Dr. Gold is with Gold Skin Care Center in Nashville, Tennessee.
FUNDING: This study was funded by B.A.I. Biosciences.
DISCLOSURES: Dr. Xinge Diana Zhang, Xuefei Sophie Bai, and Claudia Teng are employees of B.A.I. Biosciences. All other authors report no conflicts of interest relevant to the contents of this article.
Abstract: Objective: The authors sought to observe the effect of nanodiamond-zinc oxide (ND-ZnO)-containing skincare preparations on facial erythema and acne-like lesions in subjects with rosacea or rosacea-like symptoms. Methods: An eight-week, real-world case series was compiled, with 35 included patients who exhibited facial redness and/or papulopustular features. Participants were assigned to one of two regimens: (1) ND-ZnO-containing cream applied once daily, or (2) ND-ZnO-containing serum applied twice daily with the cream layered on in the morning. Redness was assessed via expert grading using a standardized scale, while lesion counts (inflammatory and non-inflammatory) were evaluated by a board-certified dermatologist at baseline, Week 4, and Week 8. Participants also completed a self-assessment questionnaire on skin tone and radiance. Results: Of the participants evaluated for redness, 94.7 percent showed improvement by expert grading. Self-assessment revealed that 95 percent reported brighter, more even skin tone. Mean erythema scores decreased from 0.86 at baseline to 0.69 at Week 4 and 0.54 at Week 8. Non-inflammatory lesions declined from 22 to 1, and inflammatory lesions resolved completely by Week 8. Representative case studies confirmed visible improvement in redness, skin texture, and clarity. Limitations: The absence of a placebo control and the short duration limit generalizability and long-term assessment. Results should be confirmed in randomized controlled trials. Conclusion: ND-ZnO-containing skincare preparations were effective in reducing facial redness and acneiform lesions, with improvements observed across multiple skin types. These findings support their potential use in the topical management of rosacea. Keywords: Rosacea, ND-ZnO, sunscreen, serum, erythema, acne-like lesions, case study, anti-aging, wound healing
Introduction
Rosacea is a chronic dermatological condition affecting approximately five percent of the global population,1 characterized by persistent facial redness, visible blood vessels, and, at times, inflammatory acne-like lesions.2 The condition predominantly impacts adults with lighter skin types, though symptom severity and manifestation vary widely. Rosacea can be classified into several subtypes, including erythematotelangiectatic rosacea (ETR), papulopustular (acne) rosacea, and mixed phenotypes, all of which present with varying degrees of erythema, inflammation, and lesion formation.3,4 Erythematotelangiectatic rosacea (ETR) is defined by redness in nose, cheeks, and central facial erythema that can extend to the neck and chest that may also accompanies with skin sting and swelling. Papulopustular rosacea, another common subtype, is characterized by persistent facial redness accompanied by inflammatory papules and pustules that can resemble acne but typically do not respond to conventional acne treatments. Given the significant impact on physical appearance and quality of life, there is a need for effective management of rosacea symptoms.5–7
Nanodiamond-zinc oxide (ND-ZnO) is a novel molecule engineered to enhance skin regeneration and repair.8,9 Recent applications ND-ZnO in topical skin preparations reveals potentials for this novel molecule to act as a multifunctional, effective approach for rosacea management. Oxidative stress, primarily driven by excessive production of reactive oxygen species (ROS), is now recognized as a key contributor to the pathophysiology of inflammatory skin disorders including rosacea. It can directly damage skin barrier and promote inflammatory signaling, which in turn perpetuates erythema, papules, and pustules.8 Interestingly, it is found experimentally that the ND-ZnO’s core-shell structure captures the ROS generated by UV exposure and UV filters upon absorbing UV rays when exposed to solar-simulated radiation.9 Moreover, unlike small-molecule antioxidants, which often fail in clinical studies due to poor reactivity or bioavailability, the unique biophysical properties of ND-ZnO allow for localized, durable ROS neutralization at the skin surface, where oxidative stress plays a prominent role.
In addition to its antioxidant properties, ND-ZnO supports skin repair and rejuvenation. Wound healing scratch assays reveal that ND-ZnO-treated human dermal fibroblasts demonstrate a 198-percent increase in migration compared to controls, significantly accelerating wound closure and epidermal cell regeneration within 24 hours. In vitro assay showed a 71.3-percent restoration of collagen synthesis in aged fibroblasts treated with ND-ZnO and a 203-percent increase in the transdermal absorption of therapeutic agents like niacinamide.10 Through these combined mechanisms of ROS eradication, inflammation reduction, collagen stimulation, and enhanced delivery, ND-ZnO offers a promising strategy for restoring a healthy skin barrier in rosacea-prone skin.
In this paper, we investigate the efficacy of the ND-ZnO molecule in treating rosacea symptoms through a real-world case series. We evaluate two topical skincare preparations that contain ND-ZnO: Dynamic Age Defense (DAD) cream (B.A.I. Biosciences, Cambridge, Massachusetts) and Bioadaptive Stress Repair (BSR) serum (B.A.I. Biosciences, Cambridge, Massachusetts). The results from this case series demonstrate visible improvements in facial redness and a marked reduction in acne-like lesions. To illustrate these effects, we include investigator-graded redness evaluation and lesion counts from a cohort of 35 patients, comparing baseline and Week 8 data to quantitatively assess improvements in inflammatory rosacea symptoms. We present four representative case studies with before-and-after images highlighting the visible reductions in erythema and lesions. Additionally, we collected participant-reported outcomes using a self-assessment questionnaire that asked whether users experienced a reduction in facial redness and improvement in skin radiance. These responses were analyzed and presented quantitatively as an additional measure of the effectiveness of the ND-ZnO-containing skincare preparations.
Methods
Study design. An eight-week case study series was designed to observe the effect of ND-ZnO-containing products participants with rosacea and aging skin prone to erythema and acne-like lesions. Participants were divided into two groups. In the first group, participants applied DAD cream once daily in the morning, which has an in vivo SPF rating of 30 and a PA++++ (UVA) classification, in accordance with FDA testing standards. In the second group, participants applied DAD cream in the morning and BSR serum twice a day, in the morning and in the evening. The second group’s regimen was designed to assess the combined effects of the ND-ZnO-containing cream and serum on reducing both erythema and acne-like lesions. In both group, participants were required to discontinue the use of all other skincare products for the duration of the study.
Assessment methods. Investigator grading was used to assess redness and acne-like lesions at baseline, Week 4, and Week 8. Twenty (n=20) participants with Fitzpatrick Skin Types I, II, and III were included for investigator grading of redness.11 The evaluator selected this subset of 20 subjects with Fitzpatrick Skin Types I–III in order to perform visual grading with higher accuracy, as erythema is more visually discernible in lighter skin types, whereas redness can be more difficult to evaluate reliably in darker skin tones. Other features, such as lesion counts, were assessed and reported across the full study population, including those with darker skin types. Redness was evaluated using a standardized grading scale, and acne lesions were categorized as either non-inflammatory (whiteheads and blackheads) or inflammatory (papules, pustules, nodules, and cysts).12
Lesion counts were conducted by a board-certified dermatologist, who evaluated each participant’s facial area, divided into four specific zones: forehead, left and right cheeks, and lip/chin. Lesions were categorized into non-inflammatory (open and closed comedones) and inflammatory (papules, pustules, nodules, and cysts), as shown in Figure 1, and the total lesion count was reported for both categories across these zones. This approach ensured consistent evaluation of the ND-ZnO-containing cream and serum’s impact on both non-inflammatory and inflammatory lesions.

Results
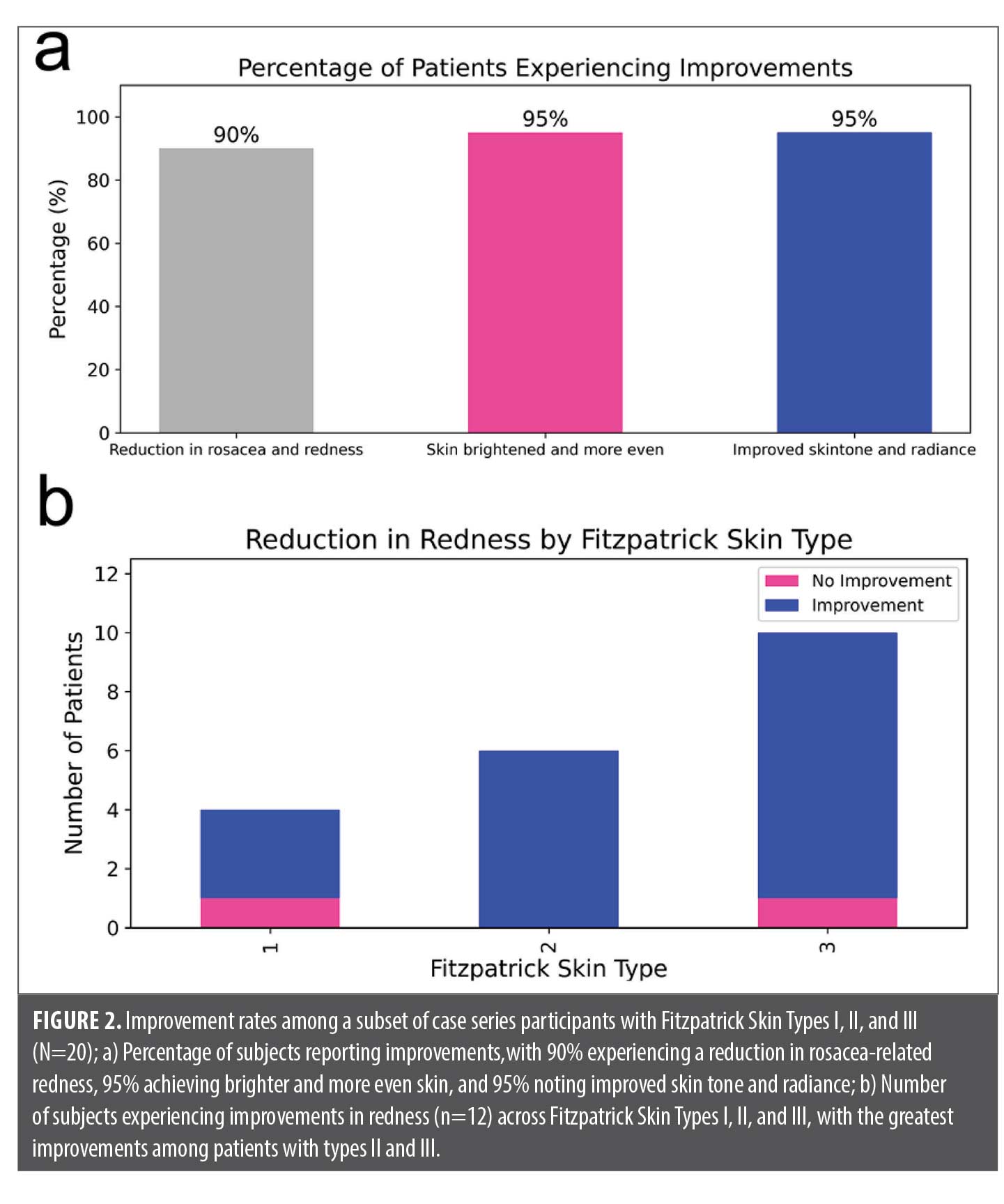
Reduction in redness. To assess the effectiveness of ND-ZnO-containing skincare preparations in reducing redness, investigator grading results from a subset of 20 subjects with Fitzpatrick Skin Types I, II, and III were analyzed. Of these participants, 95 percent showed a clinically significant reduction in facial erythema following treatment. In addition, 95 percent of surveyed subjects reported improvements in overall skin appearance, noting brighter, more even-toned skin and enhanced radiance, as shown in Figure 2A.
To further evaluate the skin preparations’ efficacy across different skin tones, we analyzed the results by Fitzpatrick Skin Type. As shown in Figure 2B, improvements were observed across all Skin Types I, II and III. This cross-type effectiveness highlights the versatility of ND-ZnO-containing skincare in managing erythema across a diverse range of skin tones.
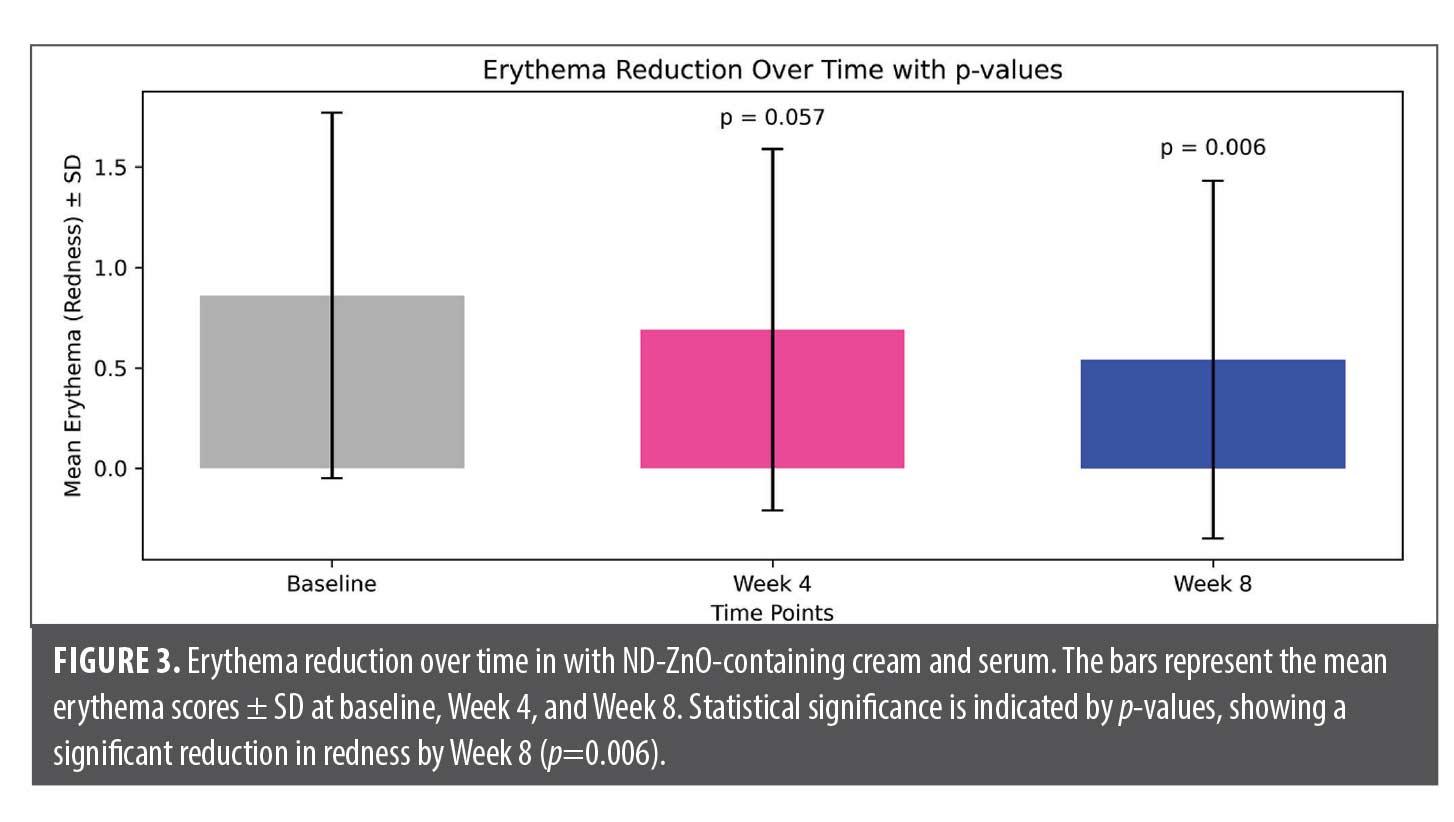
Investigator grading of facial redness was used to quantify the improvement that ND-ZnO containing skin preparation induced. As shown in Figure 3, the mean erythema score decreased from 0.86 at baseline to 0.69 at Week 4, and further to 0.54 by Week 8. The error bars represent standard deviations (±SD) at each time point, illustrating variability among participants. Statistical analysis revealed a significant reduction in redness by Week 8 (p=0.006), with a trend towards improvement already apparent by Week 4 (p=0.057). These results highlight the pronounced effectiveness of the ND-ZnO formulation in reducing erythema over time, with greater improvements observed at the eight-week mark.
Collectively, these findings demonstrate the potential of ND-ZnO-containing skincare preparations in effectively reducing redness and enhancing overall skin quality across different skin types and age groups.
Reduction in lesion count. To assess the effectiveness of the ND-ZnO-containing skincare preparations in reducing lesion counts, investigator grading results were analyzed. The case study series involved 35 participants and measured both non-inflammatory and inflammatory lesions at baseline, Week 4, and Week 8.
Over a period of eight weeks, there was a substantial reduction in non-inflammatory lesions as shown in Figure 4. At baseline, the total sum of non-inflammatory lesions was 22, which saw a slight reduction to 21 by Week 4. By Week 8, the sum of non-inflammatory lesions dramatically dropped to just one, representing a significant improvement over the trial period.

Similarly, inflammatory lesions showed a consistent decline throughout the study. Starting with four total inflammatory lesions at baseline, the number reduced to three by Week 4, and by Week 8, all inflammatory lesions had completely resolved, bringing the total to 0.
These findings, summarized in Table 1, highlight the efficacy of the ND-ZnO formulation in managing both non-inflammatory and inflammatory lesions over time. The rapid decline in lesion counts, especially between weeks 4 and 8, demonstrates the product’s potential in reducing acne-like lesions, contributing to an overall improvement in skin condition for patients with rosacea.
Representative case series. To provide a real-world view of the efficacy of the evaluated ND-ZnO-containing skincare preparations, four representative case studies were selected. These cases highlight the impact of ND-ZnO formulations on reducing erythema and improving overall skin quality in diverse subject profiles. By examining subjects of varying ages and Fitzpatrick Skin Types, these case studies illustrate the tangible benefits of ND-ZnO skincare preparations across different skin conditions and demographics, offering insights into their broader potential in managing rosacea.
Case 1 (Figure 5). A 61-year-old male with Fitzpatrick Skin Type II presented with moderate-to-severe facial erythema and clinical features consistent with papulopustular rosacea at baseline. Pronounced redness was observed across the cheeks, nose, upper lip, and chin, accompanied by inflammatory papules and areas of patchy erythema and textural roughness. The subject was not using any prescription or over-the-counter skincare or medications during the study period. He was instructed to apply the DAD cream once daily in the morning after cleansing.
After eight weeks of consistent once-daily application, the subject showed substantial clinical improvement. The follow-up images demonstrate a visibly more uniform skin tone with markedly reduced redness and diminished signs of inflammation. In addition, the overall skin texture appeared smoother, with less scaling and dryness compared to baseline. The observed improvements suggest that daily use of the ND-ZnO-containing cream alone was effective in calming inflammation and restoring skin barrier function in this case of rosacea-like facial erythema.

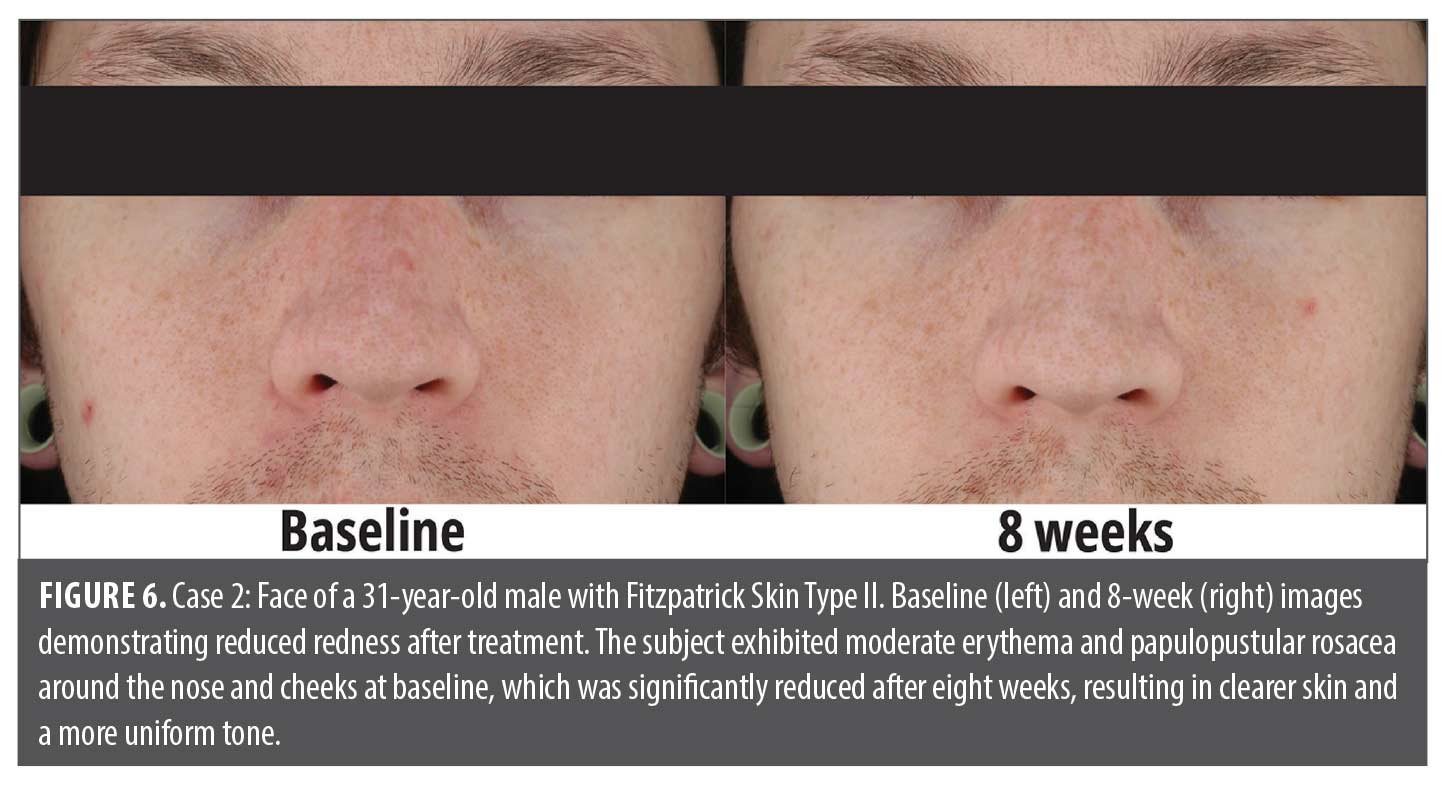
Case 2 (Figure 6). A 31-year-old male with Fitzpatrick Skin Type II presented with moderate facial erythema and papulopustular rosacea, primarily concentrated around the nasal folds and upper cheeks. Baseline images revealed diffuse redness with mild textural irregularities and an uneven skin tone, along with occasional blemishes. The subject followed a regimen of applying the DAD cream once daily for eight weeks, without the use of other active treatments during this period.
Following eight weeks of consistent once-daily use, the subject showed a visible improvement in skin appearance. Post-treatment images demonstrate a reduction in facial redness, particularly around the nose, with a more even and balanced skin tone. The complexion appeared noticeably clearer, with minimal residual erythema and improved overall texture. These results suggest that the ND-ZnO-containing cream was effective in calming inflammation and improving visible signs of rosacea-related redness in this subject.
Case 3 (Figure 7). A 38-year-old female with Fitzpatrick Skin Type I presented with mild-to-moderate facial erythema at baseline, primarily affecting the cheeks and nose. The subject demonstrated visible inflammatory features consistent with rosacea-spectrum facial redness. The redness was patchy and accompanied by scattered acneiform lesions, suggestive of early-stage or mild papulopustular rosacea.
The subject applied the DAD cream once daily for eight weeks, without using any other topical or systemic treatments. Follow-up images revealed a noticeable reduction in both erythema and acne-like lesions. The skin appeared smoother, with less visible inflammation and a more balanced, even tone. These results suggest that the ND-ZnO-containing cream effectively calmed inflammation and improved overall skin clarity, even in cases with milder or mixed rosacea presentations.

Case 4 (Figure 8). A female subject in her mid-50s with Fitzpatrick Skin Type III presented with moderate facial erythema, primarily affecting the central face, including the nose, cheeks, and nasolabial folds. The erythema was diffuse and consistent with vascular inflammation typically associated with rosacea. The subject followed a skincare regimen consisting of twice-daily application of the BRS serum, once in the morning after cleansing and again in the evening, and an additional application of the DAD cream each morning layered over the serum.
After four weeks of consistent use, the subject exhibited a visible reduction in facial redness, particularly across the nose and cheeks. The skin tone appeared more even, and background inflammation was noticeably reduced. Improvements were also observed in overall skin texture, with the skin appearing smoother, more refined, and healthier compared to baseline.

Limitations. This study was limited by the absence of a placebo control, which could provide a more rigorous evaluation of the serum’s effects. Additionally, the study’s eight-week duration may not capture the serum’s long-term effects. Future studies could address these limitations by including a control group and extending the observation period.
Conclusion
The results from the case series suggest efficacy of ND-ZnO-containing skincare preparations in rosacea. Reductions in redness were observed, among participants with Fitzpatrick Skin Types I, II, and III.
References
- Gether L, Overgaard LK, Egeberg A, et al. Incidence and prevalence of rosacea: a systematic review and meta-analysis. Br J Dermatol. 2018;179(2):282–289.
- Picardo M, Eichenfield LF, Tan J. Acne and rosacea. Dermatol Ther (Heidelb). 2017;7(Suppl 1):43–52.
- Two AM, Wu W, Gallo RL, et al. Rosacea: part I. Introduction, categorization, histology, pathogenesis, and risk factors. J Am Acad Dermatol. 2015;72(5):749–758; quiz 759–760.
- Two AM, Wu W, Gallo RL, et al. Rosacea: part II. Topical and systemic therapies in the treatment of rosacea. J Am Acad Dermatol. 2015;72(5):761–770; quiz 771–772.
- Thiboutot D, Anderson R, Cook-Bolden F, et al. Standard management options for rosacea: the 2019 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2020;82(6):1501–1510.
- Layton A, Thiboutot D. Emerging therapies in rosacea. J Am Acad Dermatol. 2013;69(6 Suppl 1):S57–65.
- Del Rosso JQ. Management of facial erythema of rosacea: what is the role of topical alpha-adrenergic receptor agonist therapy? J Am Acad Dermatol. 2013;69(6 Suppl 1):S44–56.
- Forman HJ, Zhang H. Targeting oxidative stress in disease: promise and limitations of antioxidant therapy. Nat Rev Drug Discov. 2021;20(9):689–709. Erratum in: Nat Rev Drug Discov. 2021;20(8):652.
- Bai X, Yan J, Gilchrest BA. Next-generation zinc oxide-based sunscreens: molecular characteristics and advantages. J Invest Dermatol. 2024;144(2):430–434.e1.
- Zhang XD, Teng C, Bai X, et al. Enhanced skin regeneration and therapeutic delivery using novel diamond-augmented zinc oxide. J Cosmet Dermatol. 2024;23(12):4043–4050.
- Gupta V, Sharma VK. Skin typing: fitzpatrick grading and others. Clin Dermatol. 2019;37(5):430–436.
- Frew J, Penzi L, Suarez-Farinas M, et al. The erythema Q-score, an imaging biomarker for redness in skin inflammation. Exp Dermatol. 2021;30(3):377–383.