Madelaine Haddican, MD; Rita V. Linkner, MD; Giselle Singer, BS;
Shelbi C. Jim On, MD; Matthew Gagliotti, BA; Gary Goldenberg, MD
Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York
Abstract
Background: Staphylococcus aureus has been implicated in the pathogenesis of adult hand/foot dermatitis. Objective: The authors hypothesized that retapamulin 1% ointment and clobetasol propionate 0.05% foam would decrease disease severity in subjects with hand/foot dermatitis and provide a higher clearance of Staphylococcus aureus colonization, when compared to vehicle (placebo) ointment and clobetasol propionate 0.05% foam. Methods: Adult subjects with moderate to very severe hand/foot dermatitis had twice-daily topical application of clobetasol propionate 0.05% foam to hands/feet for 14 days and were randomized to apply either retapamulin 1% ointment or vehicle ointment twice daily to hands/feet and nares for five days. Results: Seventy-three percent of subjects in the retapamulin/clobetasol group were clear/almost clear at Day 15 compared to 47 percent of subjects in the vehicle/clobetasol group (p-value of 0.04). The percentage of subjects who had both negative skin and nares cultures and were clear/almost clear was also statistically significant in favor of the retapamulin/clobetasol group at Day 15 (p-value of 0.05). Limitations: Sample size, study population. Conclusion: At Day 15, retapamulin 1% ointment with clobetasol propionate 0.05% foam was more efficacious than vehicle ointment and clobetasol propionate 0.05% foam for disease improvement and Staphylococcus aureus clearance in adult subjects with hand/foot dermatitis.
(J Clin Aesthet Dermatol. 2014;7(7):32–36.)
Hand/foot dermatitis (HFD) is a chronic disease with both genetic and environmental contributing risk factors.[1] Several studies have implicated bacterial colonization, especially Staphylococcus aureus, as a pathogenic factor for eczematous lesions.[2–4] Different mechanisms have been suggested to account for the increased S. aureus colonization. For example, the defective epidermal barrier in subjects with eczema allows S. aureus to invade these lesions and stimulate keratinocytes to release proinflammatory cytokines.[5–9] In a recent study, which investigated the relationship between S. aureus and hand dermatitis, infection rates with S. aureus were found to be significantly higher in the disease cohort (48%) as compared to controls (8%). Furthermore, the presence of S. aureus correlated closely to disease severity.[10] Another published clinical trial investigated the effect of treating S. aureus infection in children with generalized atopic dermatitis. The concomitant use of intranasal mupirocin and dilute bleach baths significantly decreased the severity of eczema in the treatment arm as compared to placebo. However, S. aureus carriage persisted in both skin and nares cultures.[11] In a randomized, double-blind, placebo-controlled study of nasal carriers of S. aureus who applied retapamulin 1% ointment (Altabax®, Stiefel Laboratories) to both nostrils for five days, cultures carriage four weeks after treatment was negative for 86 percent of subjects.[12] Thus, retapamulin 1% ointment offers the opportunity to effectively treat the presence of S. aureus in HFD. The primary purpose of this study was to investigate the use of retapamulin 1% ointment in combination with clobetasol propionate 0.05% foam for the treatment of HFD in adult subjects.
Methods
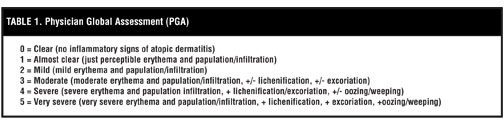
Study design. Figure 1 In a single-center, Institutional Review Board (IRB)-approved, randomized, double-blind, vehicle-controlled study at the Icahn School of Medicine at Mount Sinai, subjects with moderate to very severe HFD were randomized (1:1) to receive retapamulin 1% ointment and clobetasol propionate 0.05% foam or vehicle (placebo) ointment and clobetasol propionate 0.05% foam. Eligibility criteria for subjects included the following: >18 years of age, written and informed consent, clinical diagnosis of HFD affecting at least one hand or foot, Physician Global Assessment (PGA) of at least 3 (moderate) for HFD (Table 1), negative urine pregnancy test for females of childbearing potential, and approved method of birth control for females of childbearing potential. Exclusion criteria included the following: pregnant or breastfeeding females; known or suspected intolerance to retapamulin 1% ointment or clobetasol propionate 0.05% foam; any overt signs of skin atrophy, telangiectasias, and/or striae in the treatment area; any known history of active skin malignancy; use of any topical corticosteroids, topical antibiotics, topical immunosuppressants, other topical therapies (tar, calcineurin inhibitors), or phototherapy within eight weeks of the baseline visit; and use of any systemic corticosteroids, systemic antibiotics, or systemic immunosuppressants therapies within eight weeks of the baseline visit. Enrolled patients were randomized (1:1) to Group 1 (clobetasol propionate 0.05% foam twice-daily application to either the hands or feet for two weeks and retapamulin 1% ointment twice-daily application to anterior nares and the hands or feet for five consecutive days) or Group 2 (clobetasol propionate 0.05% foam twice-daily application to either the hands or feet for two weeks and vehicle [placebo] ointment application twice-daily to anterior nares and the hands or feet for five consecutive days). After the initial two weeks, both groups entered a treatment-free, two-week period. Efficacy and safety assessments were made at baseline (Visit 1), Day 6 (Visit 2), Day 15 (Visit 3), and Day 28 (Visit 4). Bilateral nares and the most severely affected target area of the hands or feet were cultured at baseline (Visit 1), Day 15 (Visit 3), and Day 28 (Visit 4). Enrolled subjects were given a randomization number generated by a computer pro-gram. During the study, only a designated pharmacist was aware of study drug assignment for individual patients. All study drug was distributed in unlabeled containers. Access to the randomization schedule was permitted after both the database was locked and the study unblinded to patients and study physicians.
Study assessment. The primary efficacy endpoint was the proportion of patients in each treatment group with a PGA of clear (0)/almost clear (1) at Day 6, Day 15, and Day 28 compared to baseline. Secondary endpoints were assessed at the baseline visit and included the following: the portion of subjects with intranasal and hand/foot S. aureus carriage rates, the portion of subjects with methicillin-resistance in S. aureus isolates, and comparison of the mean PGA score for subjects with and without S. aureus present in target lesion. Supportive efficacy endpoints included the proportion of subjects in each treatment group who were culture-positive for either S. aureus on the skin, nares, or both at baseline who were also culture-negative on both the skin and nares and clear/almost clear based on PGA at follow-up visits.
Study oversight. The study was conducted in accordance with the ethical principles specified in the Declaration of Helsinki and in compliance with requirements of local regulatory committees. All patients provided written and informed consent.
Statistical analysis. Sample size. To detect a statistically significant difference between the two groups, the sample size was determined to be 30 subjects for each group for a total of 60 subjects.
Analyses based on PGA (proportions of patients clear/ almost clear). P-values for categorical analyses based on PGA of 0 or 1 (proportions of patients clear/almost clear) from baseline compared to Day 6, Day 15, and Day 28 were calculated based on Chi-squared test, unless a patient’s PGA score was less than 5, then the p-value was calculated based on Fisher’s exact test. Analysis of mean change from baseline to each time point was based on the analysis of covariance (ANCOVA) model with baseline PGA as a covariate. For patients who terminated early, the early termination value was used for each of the time points with missing data.
Correlation between proportions of patients clear/almost clear based on PGA and culture-negative. Only patients culture-positive for S. aureus on either skin or nares (or both) at baseline were included in this analysis. The proportion of subjects both S. aureus culture-negative at Day 15 and Day 28 and who were also clear/almost clear based on PGA were compared between treatment groups using a chi-squared test.
{kind=link}
{kind=link}
Results
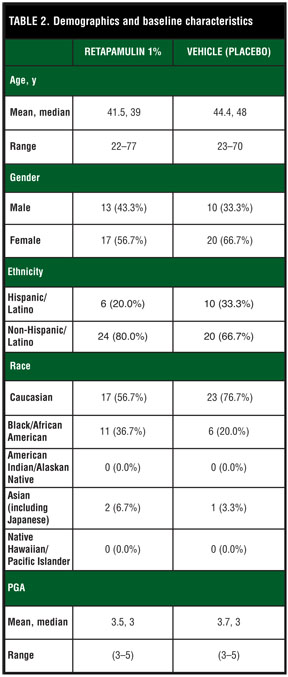
Patients. There were 60 subjects with HFD randomized at one site. The study was conducted from January 2012 to August 2012 (ClinicalTrials.gov number NCT01591785). At baseline, the mean age of the subjects was 43 years. Sixty percent of the study population was female. The majority of the patients were Caucasian (43%). The mean PGA score was 3.6. Table 2 includes the demographic and baseline characteristics for each group. Overall, 54 of 60 (90%) subjects completed the four-week study. A total of six subjects were discontinued due to worsening condition (3 subjects), use of prohibited antibiotics for nonrelated adverse events (2 subjects), and lost to follow-up (1 subject). Two of the three subjects who discontinued due to worsening condition were in the placebo/clobetasol treatment group.
Efficacy. Primary efficacy endpoint. Seventy-three percent of subjects in the retapamulin/clobetasol treatment group had a PGA of 0 or 1 at Day 15 compared to 47 percent of subjects in the vehicle/clobetasol group (p-value of 0.035). At Day 28, 50 percent of subjects in the retapamulin/clobetasol treatment group had a PGA of 0 or 1 compared to 37 percent of subjects in the vehicle/clobetasol group (p-value of 0.28). Figure 2A and Figure 2B shows photographs from two subjects in the retapamulin/clobetasol treatment group.
Secondary and supportive efficacy endpoints. Fifty percent of skin and 54 percent of nares cultures tested positive for S. aureus at baseline. Five percent of skin and 3.3 percent of nares cultures tested positive for methicillin-resistance S. aureus at baseline. The mean baseline PGA of subjects’ skin who were culture-positive for S. aureus was 3.8 compared to 3.4 for subjects who were negative for S. aureus on target lesion (p-value of 0.05). The percentage of subjects who had both negative S. aureus skin and nares cultures with a PGA of clear/almost clear at Day 15 was 61 percent for the retapamulin/clobetasol treatment group compared to 30 percent for the vehicle/clobetasol group at Day 15 (p-value of 0.0495) compared to 28 and 13 percent, respectively, at Day 28 (p-value of 0.27). Only patients culture-positive for S. aureus on either skin or nares (or both) at baseline were included in this analysis.
Safety. Adverse events were experienced by eight subjects. None of the adverse events were deemed related to study drug. These adverse events included urinary tract infection (1 subject), upper respiratory infection (3 subjects), eczema flare (2 subjects), dryness (1 subject), and pruritus (1 subject).
{kind=link}
{kind=link}
{kind=link}
Discussion
The presence of S. aureus is a well-known contributing factor in the pathogenesis of atopic dermatitis.[2–4] Hand dermatitis is a common finding in adult patients with atopic dermatitis and can be the sole manifestation of the disease. A recent study provided evidence that S. aureus colonization was an important factor for the persistence of hand eczema.[10] Our data further supports the importance of S. aureus colonization in the pathogenesis of hand eczema. Our major finding in this study was that the treatment of S. aureus colonization improved PGA of subjects with HFD, for subjects in the retapamulin/clobetasol group had a statistically significant improvement of PGA score at Day 15 and were also more likely to have a PGA score of 0 or 1 and negative skin and nares culture at Day 15, compared to the vehicle/clobetasol group. It is important to note that at Day 28 (two weeks post-treatment), the difference between the two groups, for both improvement in PGA and proportions of patients clear/almost clear based on PGA and being culture-negative, was no longer statistically significant. One possible reason for the findings involves the difficulty in preventing S. aureus reoccurrence in patients with HFD. The reoccurrence of S. aureus in eczematous lesions has been previously documented.[13] Future studies should investigate the use of intermittent treatment with retapamulin 1% ointment or another antibacterial agent for longer therapeutic benefit. S. aureus colonization of target skin lesions was 50 percent at baseline in our study, which was similar to a previous study, which showed a 48-percent colonization rate for patients with hand dermatitis.[10] Our study also found that subjects with S. aureus colonization on the target lesion at baseline had a higher PGA than those without S. aureus (average PGA of 3.8 compared to 3.4, respectively; p-value of 0.05). The rate of methicillin-resistant S. aureus was low in our study population (5% of skin and 3.3% of nares cultures) and was similar to prior published rates.[11] Our study has several limitations. The study size was small, with 54/60 subjects completing the study. Our study was also only four weeks in duration, which is a snap-shot of a chronic life-long disease. The fact that our study was a single-center study is also a limitation because our study population might not be representative of the general population. A replication of this study would help further evaluate the generalizability of our findings.
Conclusion
The combination therapy of topical retapamulin 1% ointment and clobetasol propionate 0.05% foam was more efficacious than vehicle ointment and clobetasol propionate 0.05% foam for both disease improvement and S. aureus clearance in adult subjects with hand/foot dermatitis. Although, the connection between S. aureus and eczematous severity is known, its importance should be further considered and understood within clinical practice when treating subjects with the disease.
Acknowledgment
This was an investigator-initiated study funded by Stiefel, a GSK company.
References
1. Thyssen JP, Johansen JD, Linneberg A, et al. The epidemiology of hand eczema in the general population—prevalence and main finding. Contact Dermatitis. 2010;62(2):75–87.
2. Williams RE, Gibson AG, Aitchison TC, et al. Assessment of a contact-plate sampling technique and subsequent quantitative bacterial studies in atopic dermatitis. Br J Dermatol. 1990;123(4):493–501.
3. Hanifin JM, Rogge JL. Staphylococcal infections in patients with atopic dermatitis. Arch Dermatol. 1977;113(10):1383–1386.
4. Leyden JJ, Marples RR, Kligman AM. Staphylococcus aureus in the lesions of atopic dermatitis. Br J Dermatol. 1974;90(5):525–530.
5. Jensen JM, Fölster-Holst R, Baranowsky A, et al. Impaired sphingomyelinase activity and epidermal differentiation in atopic dermatitis. J Invest Dermatol. 2004;122(6):1423–1431.
6. Arikawa J, Ishibashi M, Kawashima M, et al. Decreased levels of sphingosine, a natural antimicrobial agent, may be associated with vulnerability of the stratum corneum from patients with atopic dermatitis to colonization by Staphylococcus aureus. J Invest Dermatol. 2002;119(2):433–439.
7. Komatsu N, Saijoh K, Kuk C, et al. Human tissue kallikrein expression in the stratum corneum and serum of atopic dermatitis patients. Exp Dermatol. 2007;16(6):513–519.
8. Sandilands A, Terron-Kwiatkowski A, Hull PR, et al. Comprehensive analysis of the gene encoding filaggrin uncovers prevalent and rare mutations in ichthyosis vulgaris and atopic eczema. Nat Genet. 2007;39(5):650–654. Epub 2007 Apr 8.
9. Nomura T, Akiyama M, Sandilands A, et al. Specific filaggrin mutations cause ichthyosis vulgaris and are significantly associated with atopic dermatitis in Japan. J Invest Dermatol. 2008;128(6):1436–1441.
10. Haslund P, Bangsgaard N, Jarlov JO, et al. Staphylococcus aureus and hand eczema severity. Br J Dermatol. 2009;161(4):772–777. Epub 2009 Jul 3.
11. Huang JT, Abrams M, Tlougan B, et al. Treatment of Staphylococcus aureus colonization in atopic dermatitis decreases disease severity. Pediatrics. 2009;123(5):e808–e814.
12. Naderer OJ, Anderson M, Roberts K, et al. Nasal Decolonization of Persistent Staphylococcus aureus Carriers with Twice Daily Retapamulin Treatment for 3 or 5 Days. Presentation Number L-1492. 48th ICAAC/46th IDSA Annual Meeting; October 25–28, 2008; Washington, DC.
13. Guzik TJ, Bzowska M, Kasprowicz A, et al. Persistent skin colonization with Staphylococcus aureus in atopic dermatitis: relationship to clinical and immunological parameters. Clin Exp Allergy. 2005;35(4):448–455.