Shehla Admani, MD; Stephanie Feldstein, BA;
Ernesto M. Gonzalez, MD, MBA; Sheila Fallon Friedlander, MD
Division of Pediatric and Adolescent Dermatology, Rady Children’s Hospital-San Diego and University of California at San Diego
School of Medicine, San Diego, California; Department of Pediatrics, University of Chicago, Chicago, Illinois
Abstract
Infantile hemangiomas are benign vascular tumors seen in 4.5 percent of neonates and infants. While most infantile hemangiomas can be managed with active nonintervention, a subset of patients will require more aggressive management. Here the authors review the use of beta-blockers in the treatment of infantile hemangiomas, including oral, topical, and multimodal treatment options. They discuss the latest data on propranolol, including criteria for patient selection, dosing recommendations, and appropriate monitoring for side effects and efficacy. Lastly, they review indications for topical timolol treatment and the potential benefits of concomitant laser therapy.
(J Clin Aesthet Dermatol. 2014;7(7):37–45.)
Infantile hemangiomas (IH) are benign vascular tumors composed of endothelial-like cells that can arise in the skin and/or visceral organs. A recent prospective study demonstrated a 4.5 percent incidence of IH in neonates and infants during the first nine months of life.[1,2] IH are more common in females, Caucasians, and premature and low-birth weight infants. There is a potential association between IH and multiple gestations.[3,4] Most IH arise a few weeks after birth and grow over the first 5 to 6 months of life, achieving 80 percent of their size by a mean age of three months. Involution occurs more slowly, over a period of years.[5] While historical literature cites a 10-percent improvement in IH each year (such that 50% complete involution by age 5, 70% by age 7, and 90% by age 9),[6] more recent studies have shown that IH change very little after 3.5 years of age.[7]
Although most IH can be safely managed with active nonintervention, a subset of patients may have a course complicated by ulceration, bleeding, upper airway obstruction, visual compromise, and risk for permanent disfigurement, necessitating the need for a more aggressive treatment approach.[8] Beta-blockers first emerged in the arena of hemangioma treatment in 2008 when a report was published on the potential effectiveness of propranolol for the treatment of these lesions. Léauté-Labrèze et al9 made the incidental observation that a patient being treated for hypertrophic cardiomyopathy with propranolol concurrently experienced significant improvement in his hemangioma. The lesion continued to improve despite steroid tapering, which led to the speculation that propranolol itself was the cause of this dramatic improvement. Léauté-Labrèze et al subsequently reported their experience with this and 10 other patients who were effectively treated using propranolol for their IH, both as a first-line therapy and as a second-line drug in patients who had failed or had contraindications to treatment with corticosteroids.[9] Since the publication of this landmark paper, more than 170 case studies[10] and a randomized controlled trial[11] have validated this association, leading to propranolol’s recent United States Food and Drug Administration (FDA) approval for the treatment of IH. While propranolol is the most commonly used beta blocker for IH, more recent experience has shown that topical timolol may also be effective for small, thin lesions.[12]
Systemic Therapy
Background. Propranolol is a nonselective Beta-adrenergic receptor blocker that has a long history of use in pediatric cardiac disease as an agent that decreases heart rate, blood pressure, and myocardial contractility. Though previously used off label to treat IH, it was FDA approved in March 2014 specifically for this purpose. Propranolol is lipophilic and undergoes extensive first-pass hepatic metabolism such that only 25 percent is released into the systemic circulation.[8] While the exact mechanism of action for beta blockers in the treatment of IH is unknown, several hypotheses have been proposed. Beta blockers may induce vasoconstriction, which reduces blood flow to the hemangioma, causing it to fade and soften.[13] Another theory rests on beta blockers suppressing angiogenesis through the hypoxia-inducible factor 1a vascular endothelial growth factor (HIF-1a-VEGF) pathway.[14] Finally, beta blockers may induce apoptosis of capillary endothelial cells.[15] Likely, a combination of the above effects is responsible for the therapeutic action of beta blockers in the treatment of IH.
Propranolol has replaced the previous gold standard, corticosteroids, as the treatment of choice for problematic cutaneous IH and has also been successfully utilized in treating IH of the airway[16] and liver.[17,18] It is highly efficacious, with a recent meta-analysis of 41 studies including more than 1,200 cutaneous hemangioma patients showing a response rate of 98 percent, with response rate defined as any improvement with propranolol.[19] Propranolol also has a superior side effect profile when compared to previous systemic therapies, such as steroids, vincristine, and interferon.[10] Propranolol, however, is not free of side effects and careful consideration of risks and benefits is warranted prior to initiating treatment.
Patient selection. Given the broad spectrum of manifestations and the tendency for spontaneous involution,[5] selecting the appropriate patients for propranolol therapy can be challenging. Factors to consider include lesion size, location, risk for impairment of function, and potential for permanent deformity. The possible adverse psychosocial impact on the patient and/or parents must also be taken into consideration. Patients who are appropriate candidates for propranolol therapy include those with large or complicated lesions that would cause significant morbidity if left to active nonintervention.[8] This is especially true for facial hemangiomas, as many central facial lesions leave significant fibro-fatty residua and deformities that can have a life-long negative impact on the affected child.[10] Children with large segmental IH require an evaluation for possible associated cutaneous and noncutaneous findings, including a constellation of anomalies known as PHACES syndrome (posterior fossa malformations, hemangiomas, arterial anomalies, cardiac defects and coarctation of the aorta, eye abnormalities, and sternal abnormalities or ventral developmental defects).[20] Infants with PHACES may need modified therapy, special monitoring, and potentially collaboration with pediatric cardiology and/or neurology.[8] A thoughtful discussion of this disorder and an appropriate therapeutic approach has previously been published by Denise Metry et al.[21]
IH that are ulcerated, disfiguring, or pose a risk to a vital function are particularly appropriate candidates for propranolol therapy. Lesions on the nasal tip, for example, can cause destruction of nasal cartilage and deformity if left untreated. IH near the eyelid or orbit can cause visual disturbances and amblyopia.[22] Ulcerated lesions on any part of the body can cause bleeding, pain, residual scarring, and difficulty feeding.[6] Locations most prone to ulceration include the anogenital region, lower lip, and neck, likely secondary to maceration and friction in these areas.[22] Large IH, regardless of their location, can cause high output cardiac failure due to shunting of blood.[23] Two other categories of IH that deserve special mention are “beard” area hemangiomas (those on the neck, mandible, or chin) and lumbosacral/anogenital segmental hemangiomas, which can be associated with underlying noncutaneous abnormalities and often benefit from multi-disciplinary team management.[6]
While propranolol should ideally be initiated during the proliferative phase of the hemangioma (generally before 1 year of age), it may also be effective during the involution phase and can be used in older children as well. Although most studies cite 3 to 5 years of age as the upper limit for propranolol,[24,25] children from three days to 10 years old have been treated.[19] A recent randomized, controlled trial demonstrated propranolol to be most effective in children less than six months of age. These younger children had on average greater than 80-percent involution of their IH compared to a mean of 67-percent involution seen in the 6- to 36-month cohort.[26] This underscores the importance of early recognition and intervention for patients with problematic IH.
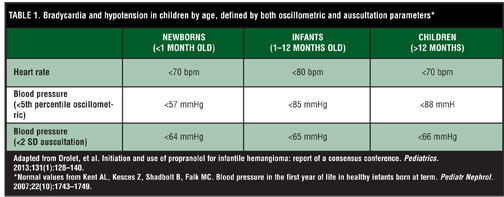
Prescreening and contraindications. Before initiation of propranolol, screening for risks associated with propranolol use should be performed. In accordance with the most recent consensus guidelines,[8] an in-clinic cardiovascular and pulmonary exam should be performed. In patients with a heart rate below normal for their age (Table 1), an electrocardiogram (ECG) is recommended. Patients with a family history of congenital heart disease, maternal history of connective tissue disease, and personal history of past or present arrhythmia should also receive an ECG and potentially a cardiology consultation. Cardiology consultation and/or echocardiogram is not necessary in children without these symptoms or risk factors. Although hypoglycemia can be seen in association with propranolol use, pretreatment screening of serum glucose has not been shown to predict which patients will develop hypoglycemia secondary to propranolol use and is not routinely recommended.[8] Relative contraindications to propranolol use include cardiac abnormalities (e.g., heart failure, second- or third-degree heart block, hypotension, and sinus bradycardia), pulmonary abnormalities (e.g., bronchial asthma), and hypersensitivity to propranolol.[22]
Safety. The currently available data has shown propranolol to have a favorable safety profile in the pediatric population. In a recent meta-analysis of 85 IH articles,[8] 56 percent of the patients had no reported complications. In the patients who did experience significant complications during propranolol use, the most frequently noted were asymptomatic hypotension, followed by pulmonary symptoms (bronchoconstriction or wheezing), hypoglycemia, and asymptomatic bradycardia. The most common non-serious adverse events reported were nightmares, somnolence, cool or mottled extremities, diarrhea, and gastroesophageal reflux.[8] Another meta-analysis of more than 41 studies described an adverse event rate of 31 percent, with sleep disturbances and acrocyanosis as the most common, accounting for 11 and 5 percent, respectively.[19] A more recent poster presentation of a multicenter, randomized, double-blind, trial showed a similarly low risk of serious side effects.[11]
Who to hospitalize. While many infants with IH can be treated with propranolol in the outpatient setting, those who require special monitoring should be admitted for inpatient initiation of treatment. These patients include any infant less than two months gestational age, those with any comorbid conditions affecting the cardiovascular or respiratory systems, those requiring frequent blood glucose monitoring, and those who do not have adequate familial or social support for appropriate observation and at-home care.[8]
Dosing and administration. While propranolol has traditionally been available at concentrations of 20mg/5mL and 40mg/5mL,[8] a new formulation (Hemangeol, Pierre Fabre Dermatologie, 4.28 mg/mL) has recently been developed specifically to treat pediatric hemangiomas. It is FDA approved at a target dose of 3mg/kg/day, though most literature and the consensus guidelines cite 2 to 2.5mg/kg/day as a reasonable endpoint.[8,19] Dosing at 1mg/kg/day may be adequate for some but not most children. In a study of 188 children at the 1mg/kg/day dose, 50 percent showed an excellent response, 30 percent had a good response, and 20 percent responded poorly.[27] This response rate is lower than that cited in studies using a target propranolol dose of 2 to 3mg/kg/day.[19,28–31]
A recent multicenter, randomized, double-blind controlled trial treated infants afflicted with IH with a placebo or one of four propranolol regimens (1 or 3mg/kg/day for 3 or 6 months). In this trial, propranolol demonstrated both a dose duration and dose escalation effect. Of infants treated at 3mg/kg/day for six months, 60.4 percent achieved treatment success (complete/near resolution of their IH), versus only 3.6 percent of infants on placebo. At lower doses and durations, fewer children responded. In fact, less than 10 percent of infants achieved success with a three-month regimen: 9.8 percent at 1mg/kg/day and 7.7 percent at 3mg/kg/day; 37.5 percent of infants responded to a six-month regimen of 1mg/kg/day, far less than those treated at 3mg/kg/day for the same duration.[11] These results demonstrate the importance of both dose amount and treatment duration in maximizing propranolol response.
Traditionally, propranolol has been administered in three daily divided doses,[8] though twice-daily dosing has also been shown efficacious.[11] Children should be fed during or right before propranolol administration to prevent hypoglycemia.[32] Propranolol should be held during illness or any other time when oral intake is low (e.g., pre-surgery).[22]
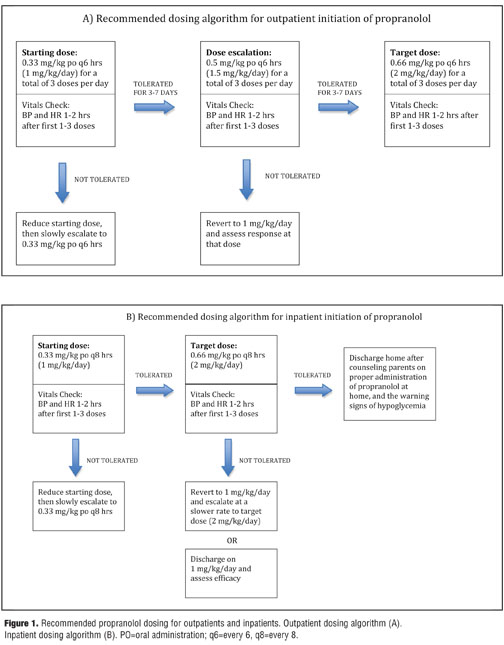
Guidelines for outpatient dosing (Figure 1). While some clinicians start patients immediately at the target dose of 2mg/kg/day[,26,29] the consensus guidelines recommend starting patients at 0.33mg/kg administered every six hours for three total daily doses (1mg/kg/day) and monitoring for side effects prior to escalation of the dose.[8] Although three times a day dosing is usually administered every eight hours, every six-hour dosing allows for three total doses without requiring excessive nighttime awakening and sleep disturbance. The consensus guidelines recommend checking heart rate and blood pressure at baseline and at 1 and 2 hours after receiving the initial dose of propranolol, coinciding with the peak effect of propranolol on the cardiovascular system. However, most experts agree that a baseline read combined with a single check 1 to 2 hours after administration of propranolol is sufficient. Heart rate and blood pressure should also be monitored after significant dose increases (>0.5mg/kg/day) and once after the target dose is reached. Since dose response is most dramatic after the first dose, it is not necessary to re-evaluate vital signs for continued use of the same dose. For patients who tolerate the initial dose for 3 to 7 days, escalation to 1.5mg/kg/day is appropriate. After 3 to 7 days at 1.5mg/kg/day, escalation to the target dose, 2mg/kg/day, is indicated if tolerated. Therefore, a patient who does not have any side effects can reach the target dose of propranolol in two weeks or less.[8]
For patients who cannot tolerate the initial dose, a lower starting dose can be used, with slow escalation to 1mg/kg/day. If a patient cannot tolerate higher doses, the clinician may consider keeping the patient at 1 or 1.5mg/kg/day if the hemangioma is responding.[8] While there are no consensus recommendations regarding treatment of IH not responding to 2mg/kg/day, escalation to 2.5 or 3mg/kg/day is a safe and reasonable approach according to the literature and the FDA.[11,19,28–31]
Guidelines for inpatient dosing. Inpatient dosing is similar to the outpatient regimen with minimal differences, allowing for closer patient monitoring and a more rapid dose acceleration (Figure 1).
Monitoring for adverse effects. Monitoring for heart rate and blood pressure should be performed and has been detailed above. It is important to note, however, that blood pressure can be difficult to measure in infants, and as a result, bradycardia may be a more easily obtained and reliable marker of adverse effects of the medication (Table 1). Children with clinically significant abnormal vital signs are at higher risk of propranolol toxicity and in these patients, dose de-escalation should be considered, and monitoring should be continued until the vital signs normalize.[8]
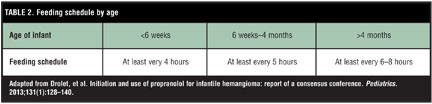
A decrease in blood glucose can also be a side effect of propranolol therapy. This side effect can be unpredictable and does not appear to be dose-related. Patients who are most at risk are low birth weight infants, and those under one year of age with limited glycogen stores and an inability to communicate their symptoms.[22] Parents should be educated on the early and late signs of hypoglycemia. Early signs include sweating, tachycardia, shakiness, anxiety, and hunger.[32] Sweating is the most reliable early sign of hypoglycemia. In a patient with only sweating and none of the other aforementioned symptoms, a hypoglycemic episode should be considered, as all the other signs can be masked by the beta blocker treatment. Late signs are more ominous and include lethargy, stupor, poor feeding, seizures, apnea, hypothermia, and loss of consciousness.[8] Hypoglycemia can be avoided with regular feeding and parents should be advised to stick to a strict feeding schedule ranging from every 4 to 8 hours depending on the age of the patient (Table 2).[32]
Monitoring for efficacy (Figure 2). Serial photography and physical examination documenting color change, size, induration, and depth have been used successfully to monitor for treatment effect.[24,25] Propranolol has a rapid onset of action, and a softening of the lesion with a color change from red to purple may be seen within 24 to 48 hours.[33] Most IH will show a halt in the growth phase between 48 hours and one month of initiation of propranolol treatment, with involution occurring over a period of months.[25] A recent prospective study of children on 2mg/kg/day of propranolol found that 65- to 80-percent involution was obtained in the first eight weeks of treatment, with an additional 2- to 10-percent involution up to 20 weeks, and no significant change in the IH after 20 weeks.[26] This data is in agreement with prior studies that show the most significant effect occurring early, in the first 4 to 16 weeks, and little change after 20 weeks of treatment for the majority of patients.[24,25]
Most patients respond at least partially to propranolol, and complete resistance is uncommon. A recent study of more than 1,000 patients found propranolol resistance (defined as continued growth during the proliferative phase or no decrease in the hemangioma during the post-proliferative phase) to occur in less than one percent of patients.[34] In the aforementioned study, all of the propranolol nonresponders who were given concomitant corticosteroids achieved a rapid response, suggesting that adjunctive corticosteroids may be a useful second-line therapy.
Duration of treatment. Currently, the ideal duration of treatment is unknown. A recent meta-analysis found that the average length of treatment with propranolol was 6.4 months, but most experts feel this is an underestimate.[19] Many practitioners keep children on propranolol until the proliferative phase has ended or until one year of age.[23–26] This extended treatment course is supported by recent findings that some IH (especially those with a significant subcutaneous component) can proliferate for up to a year, and in the case of segmental IH, for even longer (to a mean age of 17 months).[22,25,35] For children older than one year, most practitioners will treat for at least six months, or until the hemangioma has completely resolved.[19,25] In general, patients should be evaluated on a case-by-case basis, as each hemangioma may respond to treatment differently.
End of treatment and follow up. Once the hemangioma has resolved, propranolol should be discontinued. While the ideal tapering schedule is not known, many practitioners halve the dose for two weeks, and then halve it further for another two weeks before complete cessation.[26,36] This minimizes the theoretic possibility that upregulation of beta-adrenergic receptors from prolonged propranolol use will lead to a hyperadrenergic response.[29] Although propranolol is routinely withdrawn without a weaning period and without adverse effects, gradual reduction enables the practitioner to better monitor for regrowth and avoid any unforeseen problems.[36]
Rebound growth after discontinuation of propranolol is not uncommon. One meta-analysis found that 17 percent of IH experienced rebound growth after propranolol discontinuation in patients treated for a mean of 6.4 months at an average dose of 2.1mg/kg/day.[19] Another meta-analysis found a 21-percent rate of rebound growth in patients treated with propranolol for a mean of 4.3 months at 2 to 3mg/kg/day.[30] Finally, a recent study showed moderate-to-severe regrowth in 9.3 percent of cases and a mild re-growth in 22.5 percent of patients treated with propranolol for six months at a mean dose of 1.7mg/kg/day.[37] Re-initiation of propranolol is the treatment of choice for rebound growth, controlling the recurrence of all[31,37] or nearly all (28 out of 29) of the IH treated.[30]
Though there is no standard length of follow-up, most practitioners will follow patients closely for at least six months after tapering to monitor for regrowth,[26] and then yearly until school age.[31]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Topical Therapy
Timolol (Figure 3) is a therapeutic agent that has recently gained favor with many physicians for the treatment of small or thin IH. It is a nonselective beta blocker that has traditionally been used to treat glaucoma. Timolol is available in a topical solution and a gel-forming solution in concentrations of 0.25% and 0.5%. Its mode of action is similar to that of propranolol and likely due to beta blockade leading to vasoconstriction, inhibition of angiogenesis, and induction of apoptosis.[38] The major advantages of topical timolol are ready availability, cost, ease of administration, and minimal risk of drug-related adverse events. It is especially advantageous over corticosteroids when treatment is required to the face or, in particular, the periorbital area.[39] In addition, there has been one case report of topical timolol being used effectively in the treatment of an ulcerated hemangioma with no adverse effects.[38]
The first published report of timolol for the treatment of IH was published in 2010. Since that time there have been an increasing number of case reports and one multicenter trial evaluating the efficacy and safety of timolol for IH.[38–44] Findings in these recent studies suggest that application of topical timolol can provide a safe and effective alternative treatment for superficial IH and may have fewer systemic side effects than propranolol.[40] There is also some evidence to suggest that topical timolol is effective in both halting hemangioma proliferation and decreasing tumor volume with more regularity than corticosteroids.[41] The use of topical timolol for IH has been specifically described as causing the lesions to fade in color and change in consistency from tense to soft.[42]
Recently some have cautioned that cutaneous pharmocokinetic data on timolol is lacking and systemic absorption of timolol may have adverse effects for the infant being treated.[43] Side effects, such as exacerbation of asthma and abnormal breathing, have been reported with the use of timolol for pediatric glaucoma.[40] In the multi-centered retrospective study that investigated the use of timolol to treat IH in 73 patients, none of the previously reported side effects of systemic propranolol (e.g., hypoglycemia, bronchospasm, and hypotension) were observed, and the only side effect reported was one case of sleep disturbance.[39]
Though there is increasing evidence that timolol may be an effective treatment option in a subset of hemangioma patients, some researchers suggest using caution when prescribing topical timolol for IH. It is recommended that clinicians be on the alert for the known side effects of beta-blockers and thus monitor infants accordingly and limit timolol treatment to only small, localized, and superficial IH.[42] Systemic side effects of beta blocker use can include irritability, lethargy, poor feeding, mottling, and hypothermia. As a result, some experts suggest that caregivers be instructed to use no more than 1 to 2 drops twice daily to avoid potential systemic absorption.[43]
{kind=link}
Multimodal Therapy
Pulsed-dye laser (PDL) (Figure 4) has been used for the treatment of cutaneous vascular anomalies for more than 30 years and is especially effective for port-wine stains.[21] Its use in IH remains somewhat controversial due to the risk of side effects, such as ulceration and scarring,[45] as well as mixed clinical reports on efficacy. Batta et al,46 for example, reported no difference in IH of children treated with PDL versus active nonintervention in a controlled trial. However, suboptimal fluences and lack of appropriate cooling methods may have weakened the validity of their assessment. Indeed, many other studies have found this modality to be a useful part of IH treatment, especially for superficial and ulcerated lesions.[47,48]
Multimodal therapy using a combination of propranolol and PDL has also been shown to be an effective treatment option in select patients. Some practitioners use PDL as a “mop up” therapy to treat residual telangiectasias or erythema.[10] Other studies advocate early use of PDL prior to the end of the proliferative phase.[49] A recent study by Reddy et al12 found that IH treated with propranolol and PDL concurrently achieved complete clearance more often and more quickly than IH treated with propranolol and then PDL sequentially or propranolol alone. Other practitioners have started to use timolol and PDL as combination therapy,[50] and corticosteroid use has previously been reported as an effective adjunctive treatment option in propranolol-resistant IH.[34] Given the often incomplete clearance of hemangiomas with propranolol or timolol, leaving residual atrophy and/or telangiectasias, combination therapy may become more common in the future as a potential treatment option.
{kind=link}
Conclusion
The use of beta blockers has revolutionized the treatment of IH, leading to decreased proliferation, more rapid involution, and better cosmetic outcomes. Its superior safety profile warrants consideration as first-line treatment in patients with IH. Propranolol can be used for patients who have large and/or more complicated IH under the supervision of a healthcare provider who is able to provide close monitoring for safety. Smaller, more superficial lesions may benefit from topical timolol use, with a decreased concern for systemic side effects. Beta blockers can be used both alone and in conjunction with other treatment modalities, such as lasers, to allow for the best possible outcome for the patient. Increasing experience with these therapies will hopefully lead to a better understanding of the optimal therapeutic approach for treating IH.
References
1. Kanada KN, Merin MR, Munden A, Friedlander SF. A prospective study of cutaneous findings in newborns in the United States: correlation with race, ethnicity, and gestational status using updated classification and nomenclature. J Pediatr. 2012;161(2):240–245.
2. Kilcine C, Frieden IJ. Infantile hemaniomas: how common are they? A systematic review of the medical literture. Pediatr Dermatol. 2008;25(2):168–173.
3. Haggstrom AN, Drolet BA, Baselga E, et al. Prospective study of infantile hemangiomas: clinical characteristics predicting complications and treatment. Pediatrics. 2006;118(3):882–887.
4. Munden A, Butschek R, Tom WL, et al. Prospective study of infantile haemangiomas: incidence, clinical characteristics and association with placental anomalies. Br J Dermatol. 2014;170(4):907–913.
5. Chang LC, Haggstrom AN, Drolet BA. Growth characteristics of infantile hemangiomas: implications for management. Pediatrics. 2008;122(2):360–367.
6. Paller AS, Mancini AJ. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. Philadelphia: Elsevier Saunders; 2011.
7. Couto RA, Maclellan RA, Zurakowski D, Greene AK. Infantile hemangioma: clinical assessment of the involuting phase and implications for management. Plast Reconstr Surg. 2012;130(3): 619–24.
8. Drolet BA, Frommelt PC, Chamlin SL, et al. Initiation and use of propranolol for infantile hemangioma: report of a consensus conference. Pediatrics. 2013;131(1):128–140.
9. Leaute-Labreze C, Dumas de la Roque E, Hubiche T, et al. Propranolol for severe hemangiomas of infancy. N Engl J Med. 2008;358(24):2649–2651.
10. Chen TS, Eichenfield LF, Friedlander SF. Infantile hemangiomas: update on pathogenesis and therapy. Pediatrics. 2013;131(1):99–108.
11. Leaute-Labreze, et al. Propranolol in infantile hemangiomas: results from an international randomized, placebo-controlled, multidose adaptive phase 2/3 study. Late-breaking abstract. Presented at the 71st Annual Meeting of the American Academy of Dermatology (AAD); February 28, 2013; Miami Beach, Florida.
12. Reddy KK, Blei F, Brauer JA. Retrospective study of the treatment of infantile hemangiomas using a combination of propranolol and pulsed dye laser. Dermatol Surg. 2013;39(6): 923–933.
13. Storch CH, Hoeger PH. Propranolol for infantile haemangiomas: insights into the molecular mechanisms of action. Br J Dermatol. 2010;163(2):269–274.
14. Chim H, Armijo BS, Miller E, et al. Propranolol induces regression of hemangioma cells through HIF-1?-mediated inhibition of VEGF-A. Ann Surg. 2012;256(1):146–156.
15. Ji Y, Li K, Xiao X, et al. Effects of propranolol on the proliferation and apoptosis of hemangioma-derived endothelial cells. J Pediatr Surg. 2012;47(12):2216–2223.
16. Vlastarakos PV, Papacharalampous GX, Chrysostomou M, et al. Propranolol is an effective treatment for airway haemangiomas: a critical analysis and meta-analysis of published interventional studies. Acta Otorhinolaryngol Ital. 2012;32(4):213–221.
17. Mhanna A, Franklin WH, Mancini AJ. Hepatic infantile hemangiomas treated with oral propranolol—a case series. Pediatr Dermatol. 2011;28(1):39–45.
18. Mazereeuw-Hautier J, Hoeger PH, Benlahrech S, et al. Efficacy of propranolol in hepatic infantile hemangiomas with diffuse neonatal hemangiomatosis. J Pediatr. 2010;157(2):340–342.
19. Marqueling AL, Oza V, Frieden IJ, Puttgen KB. Propranolol and infantile hemangiomas four years later: a systemic review. Pediatr Dermatol. 2013;30(2):182–191.
20. Metry D, Heyer G, Hess C, et al. Consensus statement on diagnostic criteria for PHACE syndrome. Pediatrics. 2009;124(5):1447–1456.
21. Metry D, Frieden IJ, Hess C, et al. Propranolol use in PHACE syndrome with cervical and intracranial arterial anomalies: collective experience in 32 infants. Pediatr Dermatol. 2013;20(1):71–89.
22. Holland KE, Drolet BA. Approach to the patient with an infantile hemangioma. Dermatol Clin. 2013;31(2):289–301.
23. Neri I, Balesteri R, Patrizi A. Hemangiomas: new insight and medical treatment. Dermatol Ther. 2012;25(4):322–334.
24. Bagazgoitia L, Torrelo A, Lopez-Gutierrez JC, et al. Propranolol for infantile hemangiomas. Pediatr Dermatol. 2011;28(2):108–114.
25. Hogeling M, Adams S, Wargon O. A randomized controlled trial of propranolol for infantile hemangiomas. Pediatrics. 2011;128(2):e259–e266.
26. Sondhi V, Patnaik SK. Propranolol for Infantile Hemangioma (PINCH): an open-label trial to assess the efficacy of propranolol for treating infantile hemangiomas and for determining the decline in heart rate to predict response to propranolol. J Pediatr Hematol Oncol. 2013 Aug 7. [Epub ahead of print].
27. Phillips RJ, Penington AJ, Bekhor PS, Crock CM. Use of propranolol for treatment of infantile haemangiomas in an outpatient setting. J Paediatr Child Health. 2012;48(10): 902–906.
28. Hasan M, Rahman M, Hoque S, et al. Propranolol for hemangiomas. Pediatr Surg Int. 2013;29(3):257–262.
29. Cushing SL, Boucek RJ, Manning SC, et al. Initial experience with a multidisciplinary strategy for initiation of propranolol therapy for infantile hemangiomas. Otolaryngol Head Neck Surg. 2011;144(1):78–84.
30. Menezes MD, McCarter R, Greene EA, Bauman NM. Status of propranolol for treatment of infantile hemangioma and description of a randomized clinical trial. Ann Otol Rhinol Laryngol. 2011;120(10):686–695.
31. Shehata N, Powell J, Dubois J, et al. Late rebound of infantile hemangioma after cessation of oral propranolol. Pediatr Dermatol. 2013;30(5):587–591.
32. Martin K, Bleib F, Chamlin SL, et al. Propranolol treatment of infantile hemangiomas: anticipatory guidelines for parents and caretakers. Pediatr Dermatol. 2013;30(1):155–159.
33. Lee KC, Bercovitch L. Update on infantile hemangiomas. Semin Perinatol. 2013;37(1):49–58.
34. Caussé S, Aubert H, Saint-Jean M, et al. Propranolol-resistant infantile hemangiomas. Br J Dermatol. 2013;169(1):125–129.
35. Bagazgoitia L, Hernandez-Martin A, Torrelo A. Recurrence of infantile hemangiomas treated with propranolol. Pediatr Dermatol. 2011;28(6):658–662.
36. Sanchez-Carpintero I, Ruiz-Rodriguez R, Lopez-Gutierrez JC. Propranolol in the treatment of infantile hemangioma: clinical effectiveness, risks, and recommendations. Actas Dermosifiliogr. 2011;102(10):766–779.
37. Vercellino N, Romanini MV, Pelegrini M, et al. The use of propranolol for complicated infantile hemangiomas. Int J Dermatol. 2013;52(9):1140–1146.
38. Thomas J, Kumar, P, Kumar DD. Ulcerated infantile haemangioma of buttock successfully treated with topical timolol. J Cutan Aesthet Surg. 2013;6(3):168–169.
39. Chakkittakandiyil A, Phillips R, Frieden IJ, et al. Timolol maleate 0.5% or 0.1% gel-forming solution for infantile hemangiomas: a retrospective, multicenter, cohort study. Pediatr Dermatol. 2012;29:28–33.
2012;29:28–33.
40. Ni N, Langer P, Wagner R, Guo S. Topical timolol for periocular hemangioma: report of further study. Arch Ophthalmol. 2011;129(3):373–379.
41. Weissenstein A, Straeter A, Villalon G, Bittmann S. Topical timolol for amall infantile hemangioma: a new therapy option. Turk J Pediatr. 2012;54(2):156–158.
42. Semkova K, Kazandjieva J. Topical timolol maleate for treatment of infantile haemangiomas: preliminary results of a prospective study. Clin Exper Dermatol. 2013;38:143–146.
43. McMahon P, Oza V, Frieden IJ. Topical timolol for infantile hemangiomas: putting a note of caution in “cautiously optimistic.” Pediatr Dermatol. 2012;29:127–130.
44. de Graaf M, Breur JM, Raphaël MF, et al. Adverse effects of propranolol when used in the treatment of hemangiomas: a case series of 28 infants. J Am Acad Dermatol. 2011;65:320–327.
45. Witman PM, Wagner AM, Scherer K, et al. Complications following pulse dye laser treatment of superficial hemangiomas. Lasers Surg Med. 2006;38(2):116–123.
46. Batta K, Goodyear HM, Moss C, et al. Randomised controlled study of early pulsed dye laser treatment of uncomplicated childhood haemangiomas: results of a 1-year analysis. Lancet. 2002;360(9332):521–527.
47. David LR, Malet MM, Argenta LC. Efficacy of pulse dye laser therapy for the treatment of ulceratd haemagiomas: a review of 78 patients. Br J Plast Surg. 2003;56(4):317–327.
48. Morelli JG, Tan OT, Yohn JJ, et al. Treatment of ulcerated hemangiomas of infancy. Arch Pediatr Adolesc Med. 1994;148(10):1104–1105.
49. Admani S, Krakowski AC, Nelson JS, et al. Beneficial effects of early pulsed dye laser therapy in patients with infantile hemangiomas. Dermatol Surg. 2012;38(10):1739–1740.
50. Brauer JA, Geronemus R. Laser treatment in the management of infantile hemangiomas and capillary vascular malformations. Tech Vasc Interv Radiol. 2013;16(1):51–54.