 J Clin Aesthet Dermatol. 2020;13(12):27–28.
J Clin Aesthet Dermatol. 2020;13(12):27–28.
by Margit Juhasz, MD, MSc; Nathan Fackler, MSc; Christine Pham, BS; and Natasha Atanaskova Mesinkovska, MD, PhD
Drs. Juhasz and Mesinkovska are with the Department of Dermatology at the University of California-Irvine in Irvine, California. Mr. Fackler is also with Georgetown University’s School of Medicine in Washington, D.C. Ms. Pham is with the University of California-Irvine School of Medicine in Irvine, California.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
ABSTRACT: Dysregulated scar formation can cause hypertrophic scarring, a difficult entity to treat. Although fractionated lasers are a popular therapy for hypertrophic scars, laser-induced epidermal damage might cause pigmentary changes in individuals with darker skin tones. Radiofrequency microneedling delivers ablative energy directly to the dermis and is safe for use in such patients. We present a case of hypertrophic scarring in a patient with Fitzpatrick Skin Type IV treated with a combination of radiofrequency microneedling, topical and intralesional corticosteroids, and intralesional onabotulinumtoxinA. Three weeks posttreatment, scars were significantly improved in both color and texture. The patient did not report any side effects. Based on these results, this novel combination therapy appears to be a promising treatment modality for hypertrophic scars in patients with Fitzpatrick Skin Types IV to VI. However, further large-scale studies will need to be completed to determine long-term efficacy and possible adverse events.
KEYWORDS: Hypertrophic scar, combination therapy, radiofrequency microneedling, topical corticosteroids, onabotulinumtoxinA
Proper scar formation requires a delicate balance between buildup and breakdown of extracellular matrix, including collagen. Dysregulation of cytokines or growth factors during wound healing cause abnormal collagen deposition and formation of hypertrophic scars.1 Numerous techniques have been used to treat hypertrophic scars. Fractionated lasers are growing in popularity due to their ability to remodel dermal collagen, causing flattening of hypertrophic scars.2 However, laser-induced damage to the epidermis leads to pigmentary changes, such as hypo- or hyperpigmentation, in individuals with Fitzpatrick IV to VI skin tones. Therefore, modalities that deliver energy directly to the dermis have been sought for the treatment of hypertrophic scars in patients with darker skin.3
Radiofrequency (RF) microneedling (RFMN) is a relatively new therapeutic modality that delivers heat in the form of RF. The microneedle is made of a nonconductive material, except for the tip, thus delivering ablative energy to the dermis alone. Therefore, RFMN is considered safe for use in darker skin types.3–5 INTRAcel (Jeisys Corporation, Seoul, Korea) is a RFMN device that can be used to treat scars. The 1cm2 tip contains 49 microneedle electrodes that can vary in depth and energy delivered to the tissue.4 Although INTRAcel has been used to treat acne scars with success, literature on its use in treatment of hypertrophic scarring is limited. Here, we describe a case of hypertrophic scarring demonstrating marked improvement following treatment with RFMN, topical and intralesional corticosteroid, and intralesional onabotulinumtoxinA.
Case Report
A 24-year-old male patient with Fitzpatrick Skin Type IV presented to the clinic with hypertrophic scars of the forehead, bilateral ventral forearms and wrists, as well as bilateral medial, lateral, and frontal thighs secondary to self-harm. All scars were present since adolescence, except the forehead scar, which was acquired from trauma two years prior. Initial treatment with fractional ablative laser and intralesional triamcinolone (IL-TAC, 10 and 20mg/mL) yielded poor clinical results without scar flattening. Therefore, it was advised not to proceed further. Instead, treatment with a combination therapy of dual and triple-depth RFMN, IL-TAC depending on body site (10, 20, or 40mg/mL) and onabotulinumtoxinA was used.
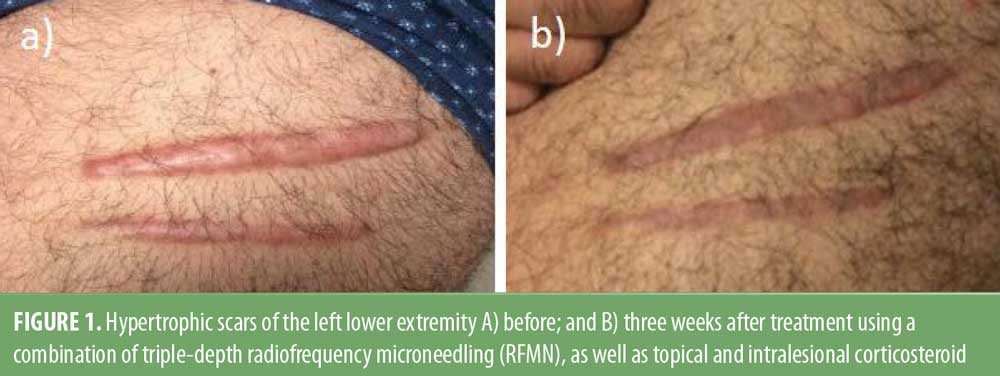
The forehead scar was treated with RFMN, 2mJ, 0.8mm, and 1.5mm, along with four units intralesional onabotulinumtoxinA and 1cc, 10mg/mL topical triamcinolone solution post-RFMN. The wrist and thigh scars were treated with RFMN, 2mJ, 0.8mm, 1.5mm and 2.0mm. Post-RFMN bilateral thigh scars received a total of 3cc, 40mg/mL topical triamcinolone, and a total of 3cc, 20mg/mL intralesional triamcinolone to the scars on the right thigh and 0.9cc to scars on the left. The patient was instructed on appropriate postcare instructions, including sun avoidance, and returned three weeks later for a routine follow up with noticeably improved appearance of hypertrophic scars, including flattening and reduced erythema (Figure 1). No adverse events were reported.
Discussion
In normal wound healing, activation of the coagulation cascade leads to formation of an extracellular scaffold for organized collagen deposition. Scar formation requires balanced collagen formation and degradation. Hypertrophic scars result from a disruption of this balance favoring proliferation. Current treatments for hypertrophic scars include topical agents, such as corticosteroids, silicone gels, and 5-fluorouracil, ablative and nonablative laser procedures, and surgical reduction or excision. Currently, topical corticosteroids and silicone gels are considered first-line therapy, but results vary significantly.2
Ablative fractional laser therapy is a popular treatment for hypertrophic scars. The laser beam is fractioned into microbeams that enter the skin, cause coagulation of blood vessels supplying the scar, and reactivate the wound healing process. This results in expression of cytokines and growth factors promoting normal collagen deposition and neocollagenesis.2 Thermal energy travels through the epidermis to reach dermal vessels and collagen, often causing necrosis of the epidermis and subsequent postinflammatory pigmentary changes in individuals with Fitzpatrick Skin Types IV to VI. In contrast, RFMN uses insulated needles inserted through the epidermis with the exposed tip delivering energy directly to the dermis.3
Fractional ablative and nonablative lasers as well as microneedling are used to enhance penetration of drugs across the epidermal barrier, especially high molecular weight molecules. The use of microneedling in combination with topicals, such as corticosteroids, has been described in multiple studies for acne scars, burn scars, and hypertrophic scars, resulting in a reduction of scar size and repigmentation.5 The use of RFMN with topical and intralesional agents, as in this case, expands on previous literature regarding combination therapy for scars.
Conclusion
The results observed in our patient suggest RFMN is an effective treatment for hypertrophic scar formation when combined with triamcinolone, both topical and intralesional, as well as intralesional onabotulinumtoxinA. In our patient, triamcinolone was used as an adjuvant therapy due to its ability to decrease inflammation and inhibit dystrophic collagen formation. OnabotulinumtoxinA was used to decrease surrounding muscle and myofibril activation, thus relieving tension on the wound and decreasing the risk of further hypertrophic scar formation.1 Large-scale studies will be needed to determine if this combination therapy is truly effective in all populations of patients, but results from this case are promising.
References
- Berman B, Maderal A, Raphael B. Keloids and hypertrophic scars: pathophysiology, classification, and treatment. Dermatol Surg. 2017;43 Suppl 1:S3–S18,
- Poetschke J, Gauglitz GG. Current options for the treatment of pathological scarring. J Dtsch Dermatol Ges. 2016;14:467–477.
- Cohen BE, Elbuluk N. Microneedling in skin of color: a review of uses and efficacy. J Am Acad Dermatol. 2016;74: 348–355.
- Cho SI, Chung BY, Choi MG, et al. Evaluation of the clinical efficacy of fractional radiofrequency microneedle treatment in acne scars and large facial pores. Dermatol Surg. 2012;38(7 Pt 1):1017–1024.
- Ramaut L, Hoeksema H, Pirayesh A, et al. Microneedling: where do we stand now? A systematic review of the literature. J Plast Reconstr Aesthet Surg. 2018;71(1):1–14.