aKavita Darji, MD; bReena Varade, MD; bDaniel West, MD; cEric S. Armbrecht, PhD; bMary A. Guo, MD
aSaint Louis University School of Medicine, Saint Louis, Missouri
bDepartment of Dermatology, Saint Louis University School of Medicine, Saint Louis, Missouri
cCenter for Health Outcomes Research, Saint Louis University, Saint Louis, Missouri
Disclosure: The authors report no relevant conflicts of interest. This study has been previously presented as a poster at the 2016 Annual AAD Meeting.
Abstract
Background: Acne vulgaris is a common, often socially distressing skin condition primarily seen in young adults. Quality of life studies have shown that people with acne are more introverted with increased social setting anxiety compared to a control group. Unfortunately, patients with acne may have residual postinflammatory hyperpigmentation, amplifying impaired psychosocial effects. Objective: To quantify the impact of postinflammatory hyperpigmentation in patients with acne using a psychometric scale. Design: A clinic-based survey was conducted among US adults with facial acne and postinflammatory hyperpigmentation. Outcomes included age, race, gender, and acne-related quality of life. A board-certified dermatologist rated each patient’s acne severity and postinflammatory hyperpigmentation. Setting: Dermatology clinic, Anheuser Busch Institute and Des Peres Hospital, Saint Louis, Missouri. Participants: 48 subjects (25 patients with acne and postinflammatory hyperpigmentation; 23 with acne only). Measurements: Acne Quality of Life survey, dermatologist rating of acne and postinflammatory [Abstract continued on next page] [Abstract continued] hyperpigmentation severity. Results: Subjects with postinflammatory hyperpigmentation reported statistically significant poorer mean scores on the Acne Quality of Life survey than subjects with acne only. Sixty percent of patients with postinflammatory hyperpigmentation had a “very markedly” impact to at least one aspect of the Acne Quality of Life survey scale compared to none of the acne only patients. There was no association between provider-reported hyperpigmentation severity and psychosocial impact. No differences in psychosocial impact were noted between males and females. Conclusion: Patients with acne and postinflammatory hyperpigmentation had poorer quality-of-life scores compared to patients with only acne. Having postinflammatory hyperpigmentation with acne negatively impacted self-perceptions and social/emotional functioning, especially in groups. J Clin Aesthet Dermatol. 2017;10(5):18–23.
Acne vulgaris, a chronic inflammatory skin disorder involving androgen predominance, keratinocyte proliferation, lipogenesis, and bacterial colonization by Propionibacterium acnes, is a social handicap that is estimated to affect more than 90 percent of adolescent patients and 15 percent of the general population.[1–5] Acne continues into adulthood in 12 to 14 percent of patients, often causing severe psychosocial impairment.[2] Patients with acne have been found to have lower self-esteem, depression, anxiety, feelings of social isolation, impaired relationships with others, and weakened ability to focus on work and school.[1],[3],[6],[7] All of these factors highlight how acne reduces quality of life in patients. Unfortunately, in addition to acne itself, a common complication of acne is residual postinflammatory hyperpigmentation (PIH), which causes further psychological and social distress in affected patients. PIH can be defined as inflammation-induced melanin release that appears after skin injury, occurring more frequently and appearing more noticeably in patients with darker skin color (Fitzpatrick skin types III/IV–VI) compared to Caucasian patients.[8],[9] Although many patients with PIH will have natural healing, recovery may take several months to years. Proper treatment can take 6 to 12 months and even longer. In several cases, PIH may be permanent, causing amplified distress for affected patients.[9] Therefore, it is important to note that PIH after acne can be as disturbing as the acne itself and lead to a lower quality of life for several affected patients. The primary purpose of this study was to utilize a psychometric scale to measure differences in quality of life between patients with acne and PIH and those with only acne. Secondary goals included evaluating gender differences and creating a comparative study of PIH severity and its psychosocial impact.
METHODS
At Saint Louis University Hospital (SLUH), US adults with facial acne and PIH were categorized into two groups: acne only or acne with PIH. The inclusion criteria involved 18 to 90 year olds and new patients seeking treatment for acne. Exclusion criteria involved established acne patients, for they may have already had treatment for the acne. All patients were recruited to complete a nine-item Acne Quality of Life (AQOL) scale developed by Gupta et al, which included questions about psychosocial situations that may be impacted by acne.10 The nine questions asked about the following: feeling self-conscious in the presence of others (Q1), decrease in socialization with others (Q2), difficulties in relationship with spouse/partner (Q3), difficulties in relationship with close friends (Q4), difficulties in relationship with immediate family (Q5), feeling like an “outcast” most the of time due to effect of acne on appearance (Q6), being “made fun of” due to appearance (Q7), feeling rejected in romantic relationship due to effect of acne on appearance (Q8), and feeling rejected by friends due to effect of acne on appearance (Q9). The patients rated their answers with 0 (not at all), 1 (mildly), 2 (moderately), and 3 (very markedly). Results of the patient survey evaluated age, race, gender and acne-related quality of life. In addition, using the Acne Global Assessment Severity Scale, a board-certified dermatologist at SLUH assessed acne severity and PIH in each patient at the time of the clinic visit. Acne severity was rated on a scale from 0 (none) to 4 (severe). Post-acne hyperpigmentation index categorized severity based on median lesion size, median lesion intensity and the number of lesions. Data was collected and statistically analyzed to draw conclusions and note trends. Analysis of variance (ANOVA) testing was used to analyze the results and determine statistical significance.
RESULTS
A total of 48 patients (30 females and 18 males) participated in the survey and were analyzed. The study included 25 patients with acne and PIH and 23 patients with only acne. Patients from different ethnicities were included: 34 Caucasian, four Hispanic or Latino, three African American, six Asian/ Pacific Islander, and one other. Using ANOVA testing, it was noted that all subjects with PIH reported statistically significant higher mean scores in the AQOL survey than subjects with only acne, indicating that PIH patients reported decreased quality of life compared to patients with only acne (p<0.05). The mean AQOL scores per question between the groups are as follows: 2.24 for PIH versus 0.74 for acne alone for feeling self-conscious, 1.44 for PIH versus 0.48 for acne alone for decrease in socialization, 0.65 for PIH versus 0 for acne alone for difficulties with partner, 0.92 for PIH versus 0.3 for acne alone for difficulties with friends, 1 for PIH versus 0.13 for acne alone for difficulties with family, 1.68 for PIH versus 0.14 for acne alone for feeling like an “outcast,” 1.4 for PIH versus 0.09 for acne alone for being “made fun of,” 1.36 for PIH versus 0.13 for acne alone for feeling rejected romantically, and 0.88 for PIH versus 0.13 for acne alone for feeling rejected by friends. As indicated, the greatest difference between groups was noted in questions 1 (self-conscious among others) and 6 (feeling like an “outcast”), while the least difference between groups was seen in questions 3 (difficulties with partner) and 4 (difficulties with friends) (Figure 1).
{kind=link}
Among all participants of the study, 60 percent of acne patients with PIH were “very markedly” affected in at least one of the realms of the AQOL scale, while no patients with only acne responded with “3” (“very markedly”) to any of the questions. Moreover, 100 percent of patients with both acne and PIH answered with “2” (“moderately”) or “3” (“very markedly”), while only four percent of patients with acne alone answered with “2” or “3.”
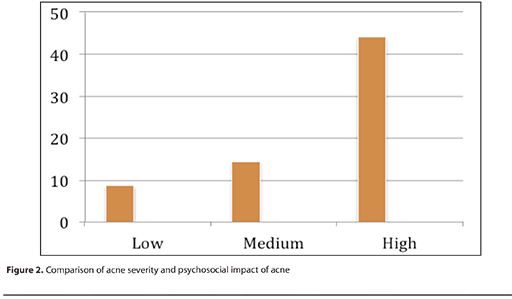
The authors’ findings show that greater severity of acne was associated with increased psychosocial impact of acne on patients. With a score of 100 signifying that the subject indicated a level of “3—very markedly” impact on his/her life from the questions on the AQOL scale, low acne severity had a value of 8.7, medium acne severity had a value of 14.4, and high acne severity had a value of 44 (Figure 2). Therefore, patients with high acne severity had the largest psychosocial impact, while those with low acne severity had the least psychosocial impact.
{kind=link}
Results did not show any relationship between provider-reported severity of post-acne hyperpigmentation and psychosocial impact. Also, data indicated no differences between male and female patients in overall psychosocial impact score.
DISCUSSION
Acne vulgaris is a common inflammatory skin disorder that is perpetuated by androgens and ligands in sebaceous gland follicles, resulting from keratinocyte proliferation, increased sebum production, comedones, and bacterial colonization by Propionibacterium acnes.[3–5] Acne lesions can manifest as a range of comedones, pustules, papules, nodules, and cysts, often leading to development of PIH and scarring.[3],[11] Skin appearance, especially of the face, can have a large impact on an individual’s self-esteem and relationships with others, thus contributing to overall quality of life. PIH is a common complication of acne and occurs more often in patients of darker skin color, frequently leaving a considerable negative psychosocial impact on these patients.[8],[9]
This is one of the few studies to report and quantitatively measure quality of life associated with acne-induced PIH. Several prior studies have evaluated quality of life associated with acne alone. As noted in prior studies, the authors found that acne itself is associated with increased psychological distress and a poorer quality of life.[6],[12],[13] Especially in adolescents, acne disrupts the development of self-identity, and often leads to anxiety, anger, depression, and decreased self-confidence.[1],[6],[7] Moreover, several affected individuals feel socially isolated due to their emotions of guilt and shame.[4] Acne can have a destructive impact on interpersonal relationships and communication with others and is also associated with decreased performance in work and school.[1],[7] In fact, approximately 5.6 percent of patients with acne experienced suicidal thoughts.[14] As a result of these findings and as shown in the authors’ study, patients suffering from acne often experience reduced quality of life.
In the authors’ study, patients with acne and PIH had greater statistically significant impairments in all nine questions asked regarding quality of life compared to patients with only acne. The greatest difference in means between the two groups was noted for questions about “feeling self-conscious in the presence of others” and “feeling like an outcast.” This can be explained by anxiety and embarrassment experienced in a social setting due to hyperpigmentation from acne. The least difference in means was noted for questions about “difficulties with significant other” and “difficulties with friends.” This finding may be due to lessened apprehension about PIH experienced among loved ones due to higher comfort level and increased sense of belonging. Additionally, the authors’ study found no statistically significant difference in PIH incidence between male and female patients. Moreover, the authors found no statistically significant difference in quality of life between female and male patients, as also noted in a prior study.[13]
Although our study did not determine any difference in PIH occurrence and quality of life between ethnicities, previous literature shows that non-White/Caucasian women encounter more PIH than Caucasian women, supporting the fact that PIH occurs more often in darker skin types.[6] A prior study showed that in acne patients of dark skin color, 65.3 percent of African American (N=239), 52.7 percent of Hispanic (N=55), and 47.4 percent of Asian (N=19) patients suffered from PIH due to acne.[11] Moreover, acne itself was more disturbing to Caucasian patients than non-Caucasian patients, while acne PIH was more distressing to non-Caucasian patients than Caucasian patients.[6] By taking these perceptions into consideration, more effective therapy can be tailored to patients based on their individual goals and preferences.
As part of the authors’ study, dermatologists assessed acne PIH severity based on the Acne Global Assessment Severity Scale. The study was limited to two providers in an attempt to decrease variability. However, it is important to note that standardizing the clinical assessment acne PIH severity is difficult to achieve, even among experts in the field. A prior study shows that although most PIH cases were determined to be mild, there was variability in the clinical assessment of severe PIH cases. Some of this variability was due to active acne present with acne PIH, causing several raters to classify it as erythema rather than PIH, thus rating it as mild PIH.[15] Variability may exist among subjective assessment of acne PIH severity by different physicians during distinct clinic appointments.[8] This finding could apply to the authors’ study, highlighting the importance of implementing standardized criteria for assessing the severity of acne PIH.
The authors’ study did not find a relationship between acne PIH severity and quality of life. However, their results do show that increased acne severity was associated with a poorer quality of life. In support of this outcome, prior literature also shows a correlation between acne severity and worsened quality of life.[3] Another study illustrated that patients with moderate/severe acne endure poorer quality of life than patients with mild acne due to more extensive psychological, social, and emotional damage. Patients with increased acne severity were noted to have weakened self-esteem, perception of body image, and social relationships.[16] However, several other studies have shown this relationship.[1],[17],[18] Various factors besides acne itself have been proposed to impair quality of life, including but not limited to personality type, presence of scarring, alcohol use, and smoking.[17],[18] Discrepancy in correlation between acne severity and quality of life in patients can also depend on the sensitivity and specificity of the scale used to assess quality of life.[1]
Impaired quality of life has been improved with appropriate treatment of acne.[19] However, the effects of acne can be so drastic that this may not always be the case. Research has shown that clinical improvement in acne severity does not affect psychosocial impairment from acne.[20] A previous study also noted that, after treatment of acne, quality of life scores did not change significantly compared to the reduction in acne severity.[1]
The authors’ study highlights the substantial effect of acne on the daily struggles that patients encounter. Previous literature shows that patients with acne experience social, psychological, and emotional dilemmas comparable to those endured by patients with epilepsy, chronic disabling asthma, arthritis, diabetes, and back pain.[13] Another study also emphasizes that female acne may be under-recognized, as it is related to anxiety and depression, and negatively affects the way acne patients focus on work or school.[7]
These findings emphasize the importance of recognizing the severity of acne patients’ psychosocial impairment and providing useful health resources to help these patients overcome and/or improve upon these emotions. It is imperative to acknowledge PIH when evaluating acne in patients, and appropriate therapy should be provided to target acne hyperpigmentation along with acne itself. The authors’ study illustrates the necessity to provide teaching programs and lessons to the public about acne vulgaris and its complications. In addition, encouraging patients to seek prompt treatment for acne can help to reduce the PIH that takes place secondary to the skin disorder itself. Additionally, assessing quality of life in acne patients can also help to evaluate for depression in patients and allow for adherence with treatment.[21]
References
1. Zauli S, Caracciolo S, Borgh A, et al. Which factors influence quality of life in acne patients? J Eur Acad Dermatol Venereol. 2014;28(1):46–50.
2. Fabbrocini G, Annunziata MC, D’Arco V, et al. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. Oct 2010;2010:893080.
3. Vilar GN, Santos LA, Sobral Filho JF. Quality of life, self-esteem and psychosocial factors in adolescents with acne vulgaris. An Bras Dermatol. 2015;90(5):622–629.
4. Zouboulis CC. Acne vulgaris. Hautarzt. 2014;65(8):733–747.
5. Williams HC, Dellavalle RP, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361–372.
6. Callender VD, Alexis AF, Daniels SR, et al. Racial differences in clinical characteristics, perceptions and behaviors, and psychosocial impact of adult female acne. J Clin Aesthet Dermatol. 2014;7(7):19–31.
7. Tanghetti EA, Kawata AK, Daniels SR, et al. Understanding the burden of adult female acne. J Clin Aesthet Dermatol. 2014;7(2):22–30.
8. Davis EC, Callender VD. Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 2010;3(7):20–31.
9. Taylor S, Grimes P, Lim J, et al. Postinflammatory hyperpigmentation. J Cutan Med Surg. 2009;13(4):183–191.
10. Gupta MA, Johnson AM, Gupta AK. The development of an Acne Quality of Life scale: reliability, validity, and relation to subjective acne severity in mild to moderate acne vulgaris. Acta Derm Venereol. 1998;78(6):451–456.
11. Hongcharu W, Taylor CR, Chang Y, et al. Topical ALA-photodynamic therapy for the treatment of acne vulgaris. J Invest Dermatol. 2000;115(2):183–192.
12. Thomas DR. Psychosocial effects of acne. J Cutan Med Surg. 2004;8(Suppl 4):3–5.
13. Mallon E, Newton JN, Klassen A, et al. The quality of life in acne: a comparison with general medical conditions using generic questionnaires. Br J Dermatol. 1999;140(4):672–676.
14. Gupta MA, Gupta AK. Depression and suicidal ideation in dermatology patients with acne, alopecia areata, atopic dermatitis and psoriasis. Br J Dermatol. 1998;139:846–50.
15. Goh CL, Abad-Casintahan F, Chow S. Evaluating acne-related post-inflammatory hyperpigmentation is a challenge even amongst experts. Japanese Dermatol Association. 2014;41:1106–1108.
16. Tasoula E, Gregoriou S, Chalikias J, et al. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An Bras Dermatol. 2012;87(6):862–869.
17. Kokandi A. Evaluation of acne quality of life and clinical severity in acne female adults. Dermatol Res Pract. 2010; Article ID 410809.
18. Gupta A, Sharma YK, Dash KN, et al. Quality of life in acne vulgaris: relationship to clinical severity and demographic data. Indian J Dermatol Venereol Leprol. 2016;82(3):292–297.
19. Gieler U, Gieler T, Kupfer JP. Acne and quality of life—impact and management. J Eur Acad Dermatol Venereol. 2015;29(Suppl 4):12–14.
20. Mulder MMS, Sigurdsson V, vanZuuren EJ, et al. Psychosocial impact of acne vulgaris. Evaluation of the relation between a change in clinical acne severity and psychosocial state. Dermatology. 2001;203.2:124–130.
21. Dreno B. Assessing quality of life in patients with acne vulgaris. Am J Clin Dermatol. 2006;7(2):99–106.