aKerry Zang, DPM; bRobert Sullivan, BSc (Hons) Podiatry, MSc Pod Surgery, PgCAcup, FIChPA, MInstChP; cSteven Shanks
aArizona Institute of Footcare Physicians, Mesa, Arizona
bMidleton Foot Clinic Group, Midleton, County Cork, Ireland
cErchonia Corporation, Melbourne, Florida
Disclosure: Dr. Zang reports no relevant conflicts of interest. Mr. Shanks is employed by Erchonia Corporation. This study was sponsored by Erchonia Corporation.
Objective: The objective of this study was to assess the efficacy of non-thermal laser therapy for treating toenail onychomycosis. Design: This retrospective study analyzed the results of three nonrandomized, open-label studies. The device used was a 635nm/405nm dual-diode laser. Affected toenails were treated for 12 minutes weekly for 2 or 4 weeks. Setting: Treatments occurred in clinic and private office settings. Participants: Subjects with onychomycosis-infected toenails were enrolled. Measurements: Fifty great toenails were included in the analysis based on visually identifiable onychomycosis; thickened, discolored nail plate; and confirmed etiology of onychomycosis. Changes in the extent of clear nail bed was measured using multi-platform image manipulation software. The primary outcome measure was the percent of toenails attaining ?3mm of clear nail growth during the six-month post-treatment period. Overall study success was defined as ?60 percent of treated toenails meeting the individual success criteria. The secondary outcome measure was change in the length of clear nail bed. Results: Most treated toenails (67%) achieved individual treatment success. The extent of clear nail at baseline increased by a mean of 5.18 (4.76) mm after 6 months (p<0.0001). In addition, 89 percent of treated toenails demonstrated an increase in clear nail across the six-month study period. No adverse events were reported. Conclusion: Non-thermal laser therapy is safe and effective for increasing the extent of clear nail in onychomycosis-infected toenails following one weekly treatment for four weeks. ClinicalTrials.gov Identifier: NCT02588599. J Clin Aesthet Dermatol. 2017;10(5):24–30.
Onychomychosis is an infection of the finger- or toenails caused by dermatophytes, yeasts, and nondermatophyte fungi. In most cases, onychomycosis is caused by dermatophytes belonging to the genus Trichophyton, Microsporum, or Epidermophyton and most commonly T. rubrum (60%), T. mentagrophytes (20%), and E. floccosum (10%)1. Risk factors for developing onychomycosis include advancing age, male gender, diabetes, immunosuppression, and poor peripheral circulation.[1],[2] The prevalence of onychomycosis in North America is estimated to be about eight percent.[3] Procedures for the diagnosis of onychomycosis include direct microscopic examination of a potassium hydroxide (KOH) preparation, culture, or nail biopsy with periodic acid-Schiff staining.[1]
Although there are generally few serious medical outcomes associated with onychomycosis, the unsightly appearance of affected nails can have a significant negative impact on quality of life,[4-6] which is greater for women[7] and can result in patients being stigmatized by others.[8]
Current therapies include oral griseofulvin, itraconazole, and terbinafine9; topical amorolfine, ciclopirox, and terbinafine10; and the new topical antifungal agents efinaconazole and tavaborole.[11] Surgical treatment is usually reserved for drug-resistant infections.[9] Disadvantages to current therapies include clinical cure rates <100 percent despite months of treatment[12] and occasional drug interactions and toxicity from oral medications.[13] A meta-analysis of available data[14] found oral itraconazole 400mg pulse therapy was the most effective treatment with a mycological cure rate of 67 percent.[15]
In vitro studies have demonstrated the ability of laser light to inhibit the growth of several relevant pathogens. Light from a 1,064nm Q-switched Nd:YAG laser at 4 and 8J/cm2 and a 532nm Q-switched Nd:YAG laser at 8J/cm2 inhibited the growth of T. rubrum.[16] Q-Switched Nd:YAG 532nm at 8J/cm2 and 1,064nm at 4 and 8J/cm2 and a 595nm pulsed dye laser at 8 to 14J/cm2 inhibited the growth of T. rubrum.[17] A 980nm laser with a pulse duration of 6ms and a fluence of 27J/cm2 inhibited the growth of T. interdigitale and Candida guilliermondi.[18] Growth of T. rubrum colonies was significantly inhibited following irradiation by 694nm Q-switched and 1,064nm long-pulsed Nd:YAG lasers.[19]
Clinically, various laser devices using 1,064nm ND:YAG have been used for treating onychomycosis, either alone[20–22] or combined with topical therapies.[23–25] The fungicidal effect of these lasers is dependent on heating the affected area,[26] which may be associated with pain and burning sensations in the treated nail bed[20],[27] and darkening under the nail or over the nail plate.[22] Long-term studies demonstrate a role for 870nm and 930nm near-infrared light for the treatment of onychomycosis[28],[29] and photodynamic therapy using red light (630nm) and methyl aminolevulinate as a photosensitizing agent has also been used for treating onychomycosis30; however, reports of photodynamic therapy studies for treating onychomycosis are small, open-label studies that do not achieve mycological cure. Several energy-based devices are cleared for producing clear nails in patients with onychomycosis, but none are currently approved for treating onychomycosis.
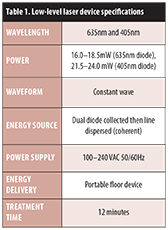
A device employing non-thermal lasers, also known as low-level lasers, has been developed for the treatment of toenail onychomycosis (Lunula Laser™, Erchonia Corporation, McKinney, Texas). The device is a dual-diode laser emitting 15.5 to 17.5mW of 635nm red laser light and 23.5 to 25.5mW of 405nm blue laser light (Table 1 ). The power reaching the surface of the skin is 1mW. When activated, laser light is directed at the affected nail at a distance of approximately four inches. Both wavelengths are simultaneously activated for a total treatment time of 12 minutes. There is no increase in the temperature of the exposed tissue.
{kind=link}
Three nonrandomized, open-label studies were performed during the development of this device to assess the efficacy of non-thermal laser therapy for the treatment of toenail onychomycosis. The objective of the following retrospective study was to analyze the results of these three studies to further establish the ability of non-thermal laser therapy to achieve clear nails in patients with toenail onychomycosis in support of a 510(k) submission to the United States Food and Drug Administration (FDA).
METHODS
This retrospective study evaluated a sample of study toenails drawn from three independent clinical trials. Each of these trials employed comparable clinical trial protocols, including the same inclusion criteria, treatment administration, baseline subject characteristics, and endpoint evaluations. The device used in each clinical trial was a dual-diode laser with wavelengths of 635nm and 405nm (Lunula Laser™, Erchonia Corporation), which is classified by the FDA/IEC as a Class 2 laser device. The technical specifications for the device are provided in Table 1 .
Enrolled subjects had not received prior treatment for onychomycosis. Treatment procedures were performed in the office or clinic of the investigators. During each treatment, the subject was seated with the non-thermal laser device on the floor in front of them. After being fitted with safety glasses, the subject placed the bare foot with the affected toenail to be treated on the treatment platform inside the non-thermal laser device. When the device was activated, the subject was simultaneously exposed to 405nm and 635nm laser light from a distance of approximately four inches. Subjects were treated for 12 minutes weekly for four weeks (Studies 1 and 3) or two weeks (Study 2). Safety glasses were worn by all subjects and investigators during treatment (Kentek Corporation; Pittsfield, New Hampshire).
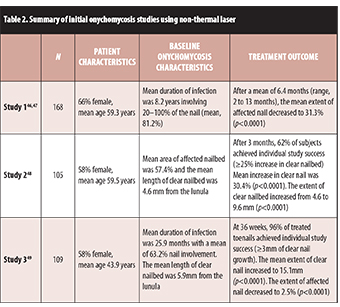
The baseline characteristics and outcomes of each study are summarized in Table 2 . Each subject had agreed to refrain from other non-study treatments for toenail onychomycosis including oral medications and nail lacquer, alternative therapies, such as acupuncture and home remedies, or to use any toenail cosmetics throughout the course of study participation. Subjects were queried about potential adverse events at the end of each trial.
{kind=link}
The clinical trials from which the data in this analysis were obtained conformed to the Good Clinical Practice guidelines of the International Conference on Harmonization.[31] Each protocol and all related documents were approved by a commercial institutional review board and/or ethics committee (Studies 1-3: Western Institutional Review Board®, Olympia, Washington and Saint Alphonsus IRB, Boise, Idaho; Study 1: Institute of Chiropodists and Podiatrists Ethics Board, Cork, Ireland). Each subject provided informed consent prior to participating in any study-related activities. ClinicalTrials.gov Identifier: NCT02588599.
Retrospective analysis. Treated great toenails from the three clinical trials described above (N=54) were selected for inclusion in four categories of onychomycosis involvement (0–25%, 26–50%, 51–75%, 76–100%), representing mild-to-severe infections. Inclusion criteria were great toenails presenting with clear, visually identifiable, and photographically documentable onychomycosis; toenails having a somewhat thickened nail plate with a cloudy appearance and some discoloration (white to yellow to brown) on visual inspection; confirmed etiology of onychomycosis through positive fungal KOH testing. Reasons for exclusion from the analysis included already having met the quota for that category of onychomycosis involvement; spikes of disease extending to nail matrix in the great toenail; infection involving the lunula of the great toenail; great toenails with <2mm clear (unaffected) nail plate length beyond the proximal fold; dermatophytoma or “yellow spike/streak” (defined as thick masses of fungal hyphae and necrotic keratin between the nail plate and nail bed) on the great toenail; onychogryphosis; proximal subungual onychomycosis; or white superficial onychomycosis.
Data analysis. The multi-platform image/photo manipulation software GNU Image Manipulation Program 2.8 (GIMP) was used for measuring the extent of clear nail bed (The GIMP team, www.gimp.org). As the results of this study were intended to support a 510(k) submission, the FDA requested that the study sponsor conduct a study to validate the application of the GIMP software system and associated methodology for the linear measurement of clear nail from digital images[32]. The results of this validation study were accepted by the FDA. The data comprised digital images of 50 great toenails with varying degrees of onychomycosis disease involvement selected from among the existing pool of images obtained during the three prior studies. For each selected toenail, there was one baseline image obtained prior to treatment and one image obtained six months post-treatment. This sample size was specified by the FDA as being sufficient to demonstrate efficacy of the study treatment.
Study endpoints. The primary outcome measure was the percent of toenails attaining ?3mm of clear nail growth over a six-month post-treatment period. Overall study success criteria was defined as ?60 percent of treated toenails meeting the individual success criteria. The secondary outcome measure was the change in the length of clear nail bed over a six-month post-treat period. Statistical analysis. A t-test for paired samples was used to compare the mean change in study endpoints from baseline to six months post-procedure.
RESULTS
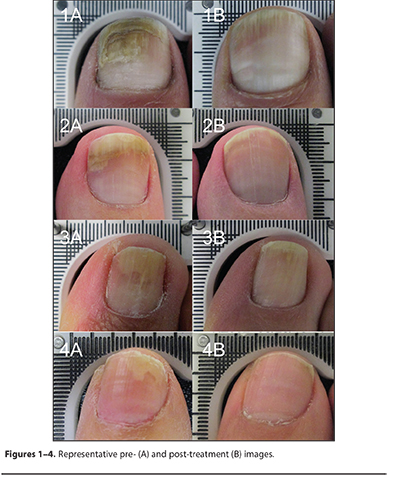
Most treated toenails (67%) achieved the criteria for individual treatment success (?3mm of clear nail growth), exceeding the pre-established overall study success goal of 60 percent. The extent of clear nail at baseline increased by a mean of 5.18 (4.76) mm, increasing from 7.64 (4.50) at baseline to 12.82mm (3.69) after six months and exceeding the pre-determined criteria of 3mm (p<0.0001). In addition, 89 percent of treated toenails demonstrated an increase in clear nail across the six-month study period. Only six (11%) treated toenails demonstrated a decrease in clear nail during the study. Representative pre- (A) and post-treatment (B) images are provided in Figures 1-4.
{kind=link}
No adverse events were reported or observed at any time during three clinical trials from which samples were obtained.
DISCUSSION
The treated nails in this study represent patients with onychomycosis ranging from mild to severe. Nevertheless, 67 percent achieved ?3mm of clear nail growth and an overall mean increase of 5.18mm. These results are similar to those of others who demonstrated 65 percent of mildly, moderately, and severely infected toenails showed ?3mm of clear nail growth and 26 percent showed ?4mm of clear nail growth.[28]
Other studies have also demonstrated the antimicrobial effects of non-thermal laser therapy, such as the inhibitory effect on biofilms formed by Streptococcus mutans and Candida albicans,[33] C. albicans in cultures[34] and infected mice,[35] and in humans with oral C. albicans infections.[36] Non-thermal laser therapy has also been shown to be active against the fungus Paracoccidioides brasiliensis in vitro and in infected mice.[37]
The antifungal mechanism of non-thermal laser therapy is not known with certainty, but is based on the principles of photomodulation. Following exposure of tissue to light from a non-thermal laser, the target chromophore appears to be the iron- and copper-containing enzyme cytochrome C oxidase in the mitochondrial respiratory chain.[38],[39] Consequently, there is an increase in the production of mitochondrial products, such as ATP, NADH, and RNA, and increased cellular respiration.[38–40] Consistent with these effects, neutrophils from non-thermal laser-treated mice are more metabolically active and have higher fungicidal activity.[37] When stimulated with non-thermal laser light in vitro, human neutrophils show greater production of reactive oxygen species, such as hydroxyl radicals and hypochlorite anions, and increased fungicidal capacity against C. albicans.[41]
An advantage of the non-thermal laser is that its antimicrobial effects are not dependent on heat. In contrast, the mean peak temperatures associated with a 808nm laser was 74.1 to 112.4°C and that of a 980nm laser was 45.8 to 53.5°C.42 Not surprisingly, the use of thermal lasers may be associated with pain or burning sensations,[20],[27],[43] described in one study as a mean score of 5 on a 10-point pain rating scale.[44] To date, no adverse events have been associated with the use of the non-thermal laser described in this paper.
A limitation of this study is the retrospective nature. More convincing results might have been achieved using a prospective, controlled study design and better balance between male and female subjects. A study of longer duration might determine the durability of treatment response.
Based on the safety and efficacy demonstrated in this retrospective study, this non-thermal laser device received FDA 510(k) market clearance for the temporary increase of clear nail in patients with onychomycosis caused by dermatophytes (e.g., Trichophyton rubrum and T. mentagrophytes) and/or yeasts (e.g., Candida albicans).[45]
CONCLUSION
Non-thermal laser therapy is a safe and effective tool for significantly increasing the extent of clear nail in onychomycosis-infected toenails after six months following one weekly treatment for four weeks. Based on these results, this device became the first non-thermal laser to receive FDA 510(k) market clearance for increasing the extent of clear nail in patients with onychomycosis.
ACKNOWLEDGMENTS
The authors acknowledge the careful manuscript review by Stephanie Shanks, the editorial assistance of Dr. Carl Hornfeldt, Apothekon, Inc., and the statistical support of Elvira Walls, Regulatory Insight, Inc. This study was sponsored by Erchonia Corporation, Melbourne, Florida.
REFERENCES
1. Welsh O, Vera-Cabrera L, Welsh E. Onychomycosis. Clin Dermatol. 2010;28:151–159.
2. Ghannoum M, Isham N. Fungal nail infections (onychomycosis): a never-ending story? PLoS Pathog. 2014;10:e1004105.
3. Gupta AK, Jain HC, Lynde CW, et al. Prevalence and epidemiology of onychomycosis in patients visiting physicians’ offices: a multicenter canadian survey of 15,000 patients. J Am Acad Dermatol. 2000;43:244–248.
4. Reich A, Szepietowski JC. Health-related quality of life in patients with nail disorders. Am J Clin Dermatol. 2011;12:313–320.
5. Milobratovi? D, Jankovi? S, Vuki?evi? J, et al. Quality of life in patients with toenail onychomycosis. Mycoses. 2013;56:543–551.
6. Tosti A, Elewski BE. Treatment of onychomycosis with efinaconazole 10% topical solution and quality of life. J Clin Aesthet Dermatol. 2014;7:25–30.
7. Belyayeva E, Gregoriou S, Chalikias J, et al. The impact of nail disorders on quality of life. Eur J Dermatol. 2013;23:366–71.
8. Chan HH, Wong ET, Yeung CK. Psychosocial perception of adults with onychomycosis: a blinded, controlled comparison of 1,017 adult Hong Kong residents with or without onychomycosis. Biopsychosoc Med. 2014;8:15.
9. Elewski B, Tavakkol A. Safety and tolerability of oral antifungal agents in the treatment of fungal nail disease: a proven reality. Ther Clin Risk Manag. 2005;1:299–306.
10. Tabara K, Szewczyk AE, Bienias W, et al. Amorolfine vs. ciclopirox—lacquers for the treatment of onychomycosis. Postepy Dermatol Alergol. 2015;32:40–45.
11. Poulakos M, Grace Y, Machin JD, et al. Efinaconazole and tavaborole: emerging antifungal alternatives for the topical treatment of onychomycosis. J Pharm Pract. 2016 Feb 11 [Epub ahead of print].
12. Ferrari J. Fungal toenail infections. BMJ Clin Evid. 2011;2011:1715.
13. Elewski BE, Tosti A. Tavaborole for the treatment of onychomycosis. Expert Opin Pharmacother. 2014;15:1439–1448.
14. Gupta AK, Daigle D, Foley KA. Network meta-analysis of onychomycosis treatments. Skin Appendage Disord. 2015;1:74–81.
15. Havu V, Brandt H, Heikkilä H, et al. A double-blind, randomized study comparing itraconazole pulse therapy with continuous dosing for the treatment of toe-nail onychomycosis. Br J Dermatol. 1997;136:230–234.
16. Vural E, Winfield HL, Shingleton AW, et al. The effects of laser irradiation on Trichophyton rubrum growth. Lasers Med Sci. 2008;23:349–353.
17. Ghavam SA, Aref S, Mohajerani E, et al. Laser irradiation on growth of trichophyton rubrum: an in vitro study. J Lasers Med Sci. 2015;6:10–16.
18. Paasch U, Mock A, Grunewald S, et al. Antifungal efficacy of lasers against dermatophytes and yeasts in vitro. Int J Hyperthermia. 2013;29:544–550.
19. Xu ZL, Xu J, Zhuo FL, et al. Effects of laser irradiation on Trichophyton rubrum growth and ultrastructure. Chin Med J (Engl). 2012;125:3697–700.
20. Helou J, Maatouk I, Hajjar MA, et al. Evaluation of Nd:YAG laser device efficacy on onychomycosis: a case series of 30 patients. Mycoses. 2016;59:7–11.
21. Kim MS, Jung JY, Cho EB, et al. The effectiveness of 1,064-nm long-pulsed Nd:YAG laser in the treatment of severe onychomycosis. J Cosmet Laser Ther. 2016;22:1–6.
22. Lu S, Zhang J, Liang Y, et al. The efficacy and prognostic factors for long pulse neodymium: yttrium-aluminum-garnet laser treatment on onychomycosis: a pilot study. Ann Dermatol. 2016;28:406–408.
23. Bhatta AK, Keyal U, Huang X, et al. Fractional carbon-dioxide (CO2) laser-assisted topical therapy for the treatment of onychomycosis. J Am Acad Dermatol. 2016;74:916–23.
24. Kim TI, Shin MK, Jeong KH, et al. A randomised comparative study of 1064 nm Neodymium-doped yttrium aluminium garnet (Nd:YAG) laser and topical antifungal treatment of onychomycosis. Mycoses. 2016 Jul 12 [Epub ahead of print].
25. Zhang J, Lu S, Huang H, et al. Combination therapy for onychomycosis using a fractional 2940-nm Er:YAG laser and 5% amorolfine lacquer. Lasers Med Sci. 2016 Jun 23 [Epub ahead of print].
26. Carney C, Cantrell W, Warner J, et al. Treatment of onychomycosis using a submillisecond 1064-nm neodymium:yttrium-aluminum-garnet laser. J Am Acad Dermatol. 2013;69:578–582.
27. Kalokasidis K, Onder M, Trakatelli MG, et al. The effect of Q-switched Nd:YAG 1064?nm/532?nm laser in the treatment of onychomycosis in vivo. Dermatol Res Pract. 2013;2013:379725.
28. Landsman AS, Robbins AH, Angelini PF, et al. Treatment of mild, moderate, and severe onychomycosis using 870- and 930-nm light exposure. J Am Podiatr Med Assoc. 2010;100:166–177.
29. Landsman AS, Robbins AH. Treatment of mild, moderate, and severe onychomycosis using 870- and 930-nm light exposure: some follow-up observations at 270 days. J Am Podiatr Med Assoc. 2012;102:169–171.
30. Robres P, Aspiroz C, Rezusta A, et al. Usefulness of photodynamic therapy in the management of onychomycosis. Actas Dermosifiliogr. 2015;106:795–805.
31. International Conference on Harmonisation. Guidance for Industry E6 Good Clinical Practice: Consolidated Guidance. April, 1996. http://www.fda.gov/ downloads/Drugs/Guidances/ucm073122.pdf. Accessed on July 19, 2016.
32. Data on file. A validation protocol for application of the GNU Image Manipulation Program (GIMP 2.8) to the measurement of mm of clear nail on toenails; Version 2.0, April 24, 2015. Erchonia Corporation, McKinney, Texas; 2015.
33. Basso FG, Oliveira CF, Fontana A, et al. In vitro effect of low-level laser therapy on typical oral microbial biofilms. Braz Dent J. 2011;22:502–510.
34. Maver-Biscanin M, Mravak-Stipetic M, Jerolimov V. Effect of low-level laser therapy on Candida albicans growth in patients with denture stomatitis. Photomed Laser Surg. 2005;23:328–332.
35. Seyedmousavi S, Hashemi SJ, Rezaie S, et al. Effects of low-level laser irradiation on the pathogenicity of Candida albicans: in vitro and in vivo study. Photomed Laser Surg. 2014;32:322–329.
36. Scwingel AR, Barcessat AR, Núñez SC, et al. Antimicrobial photodynamic therapy in the treatment of oral candidiasis in HIV-infected patients. Photomed Laser Surg. 2012;30:429–432.
37. Burger E, Mendes AC, Bani GM, et al. Low-level laser therapy to the mouse femur enhances the fungicidal response of neutrophils against Paracoccidioides brasiliensis. PLoS Negl Trop Dis. 2015;9:e0003541.
38. Avci P, Gupta A, Sadasivam M, et al. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Semin Cutan Med Surg. 2013;32:41–52.
39. Chung H, Dai T, Sharma SK, et al. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40:516–533.
40. Wang L, Hu L, Grygorczyk R, et al. Modulation of extracellular ATP content of mast cells and DRG neurons by irradiation: studies on underlying mechanism of low-level-laser therapy. Mediators Inflamm. 2015;2015:630361.
41. Cerdeira CD, Lima Brigagão MR, Carli ML, et al. Low-level laser therapy stimulates the oxidative burst in human neutrophils and increases their fungicidal capacity. J Biophotonics. 2016 May 31 [Epub ahead of print].
42. Paasch U, Nenoff P, Seitz AT, et al. Heat profiles of laser-irradiated nails. J Biomed Opt. 2014;19:18001.
43. Moon SH, Hur H, Oh YJ, et al. Treatment of onychomycosis with a 1,064-nm long-pulsed Nd:YAG laser. J Cosmet Laser Ther. 2014;16:165–170.
44. Noguchi H, Miyata K, Sugita T, et al. Treatment of onychomycosis using a 1064nm Nd:YAG laser. Med Mycol J. 2013;54:333–339.
45. Press Release. Erchonia Corporation, McKinney Texas, July 5, 2016. http://www.prnewswire.com/ news-releases/nail-fungus-sufferers-find-relief-in-new-laser-treatment-300293487.html. Accessed on July 19, 2016.
46. Data on file. Evaluation of the effect of the Erchonia Lunula Laser™ on the temporary increase of clear nail in patients with toenail onychomycosis. Institute of Chiropodists and Podiatrists (Ireland) Ethics Board Approval # LLNS/RS0312. Erchonia Corporation, McKinney, Texas; 2010.
47. Sullivan R, O’Flynn D. Erchonia laser therapy in the treatment of onychomycosis. A preliminary report on an ongoing clinical trial. Podiatr Rev. 2014;71:6–9.
48. Data on file. An evaluation of the effect of the Erchonia FX-405™ on treating toenail onychomycosis. Clinical StudyClinicalTrials.gov Identifier: NCT01534689. https://clinicaltrials.gov/ct2/show/results/NCT01534689. Erchonia Corporation, McKinney, Texas; 2012.
49. Data on file. An evaluation of the effect of the Erchonia LUNULA on treating toenail onychomycosis. ClinicalTrials.gov Identifier: NCT02242019. https://clinicaltrials.gov/ct2/show/NCT02242019. Erchonia Corporation, McKinney, Texas; 2014.