 J Clin Aesthet Dermatol. 2021;14(11):38–40.
J Clin Aesthet Dermatol. 2021;14(11):38–40.
by Michael Roberts, DO; David B. Roy, DO, FAOCD, FAAD;
Marcus Goodman, DO, FAOCD, FAAD; and Gagandeep Grewal, MD
Drs. Roberts and Goodman are with the Philadelphia College of Osteopathic Medicine in Roswell, Georgia. Dr. Roy is with Pine Belt Dermatology and Skin Cancer Center in Petal, Mississippi. Dr. Grewal is with Merit Health Wesley in Hattiesburg, Mississippi.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
ABSTRACT: Background. Activated oxygen is an important chemical for disinfecting surfaces. In the last 10 years, it has become increasingly common in continuous positive airway pressure (CPAP) devices.
Objective. We sought to treat three cases of perioral dermatitis with concomitant use of CPAP devices.
Methods. Three patients presented to the clinic with the complaint of a burning and stinging skin irritation involving the bilateral malar cheeks. Physical exam revealed symmetric, scaling, well-demarcated, erythematous, and slightly indurated areas of skin involving the bilateral malar cheeks. Corticosteroids were prescribed and provided little relief. In all three cases, the CPAP masks were worn within one hour of completing the sanitizing cycle. Each patient was instructed to lengthen the time between completion of the sanitizing cycle and application of the mask to a minimum of four hours.
Results. All patients had resolution of their symptoms within two weeks of the modification, measured by subjective resolution and photodocumentation with resolution of erythema and scaling.
Conclusion. Ozone follows common gas laws such that its decay time can be considered in terms of half-life. Ozone requires approximately 1,524 minutes (25.4 hours) to decay one-half life when other factors are controlled. The activated oxygen containers are a fixed environment that could be causing increased ozone residue on the CPAP machines. The residual ozone reacts with the natural oils on the insdividual’s skin to cause perioral dermatitis.
Key words: Continuous positive airway pressure, sleep apnea, dermatitis, face mask, ozone
Continuous positive airway pressure (CPAP) machines are commonly used to treat obstructive sleep apnea (OSA), an occlusional disorder of the upper airway that occurs while sleeping, which causes intermittent reduction of oxygen saturation.1 OSA affects as many as 26 percent of the adult population in the United States.2 Since 1981, positive airway pressure has been the mainstay treatment for OSA.3 As of 2011, the use of activated oxygen disinfecting machines to sanitize CPAP machines has increased.4 These machines activate oxygen into ozone and use humidified oxygen to disinfect the CPAP mask and tubing. Moreover, ozone is currently used for a variety of disinfecting aplications, including food processing, prevention of dental caries, and chronic wounds.5–7
Ozone produces free radicals through two mechanisms. The first mechanism entails ozone and an electron donor. A well-studied example of this mechanism utilizes the electron donor glutathione (GSH), which produces the radical anion ozone and radical anion thiyl GS. The ozone radical ion then reacts with a proton to poduce a hydroxyl radical and dioxygen.8 The second mechanism is radical-dependent production of cytotoxic molecules. The peroxyl radical is formed from carbon and oxygen.8 Ozone is believed to play a part in both skin and lung diseases, potentially through free radical development.9,10
Ozone has an attractive value as a disinfectant, in part because ozone therapy is a strong antiseptic against microorganisms. One study found almost complete eradication of methicillin-resistant Staphylococcus aureus (MRSA) with oxygenated oil and water.11 The MRSA-infected areas of tissue that were treated with this therapy also exhibited minimal scarring.11 Ozone can also be used against viruses. One study recorded a significant decrease in the load of Norwalk virus in drinking water after five minutes of ozone treatment.12 In addition, ozone is currently used in dentistry to disinfect, clean wounds, and control bleeding.13 Ozone appears to be effective against bacteria, viruses, and fungi.14
Presented here is the first case series of a CPAP-related irritant contact dermatitis, utilizing non-latex fitted masks that were cleaned using activated oxygen. All three patients reported in this study presented to a local dermatology clinic. The patients presented at their regularly scheduled appointments, but all patients complained of a similar condition that appeared to be a form of contact dermatitis. All three patients used a CPAP machine that utilizes an industry-standard activated oxygen disinfector.
Case presentations
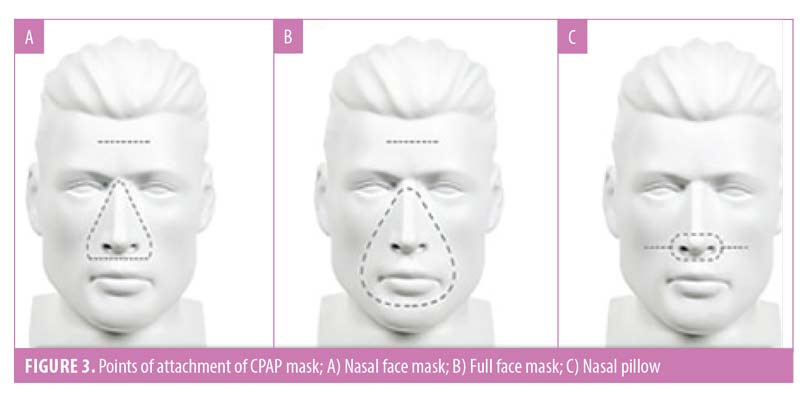
Three patients, including a 73-year-old woman, 55-year-old woman, and 51-year-old man, presented to the clinic for their regularly scheduled skin exam. Each patient reported an additional complaint of a burning and stinging skin irritation involving the bilateral malar cheeks (Figures 1 and 2). Two patients used the full face mask and one patient used the nasal mask (Figure 3).15 The duration of the irritation ranged from three months to one year. Interestingly, none of the patients reported pruritus. In each case, the history revealed the use of an activated oxygen disinfector that was temporally related to the onset of symptoms. The manufacturer of the disinfector was the same in all scenarios.
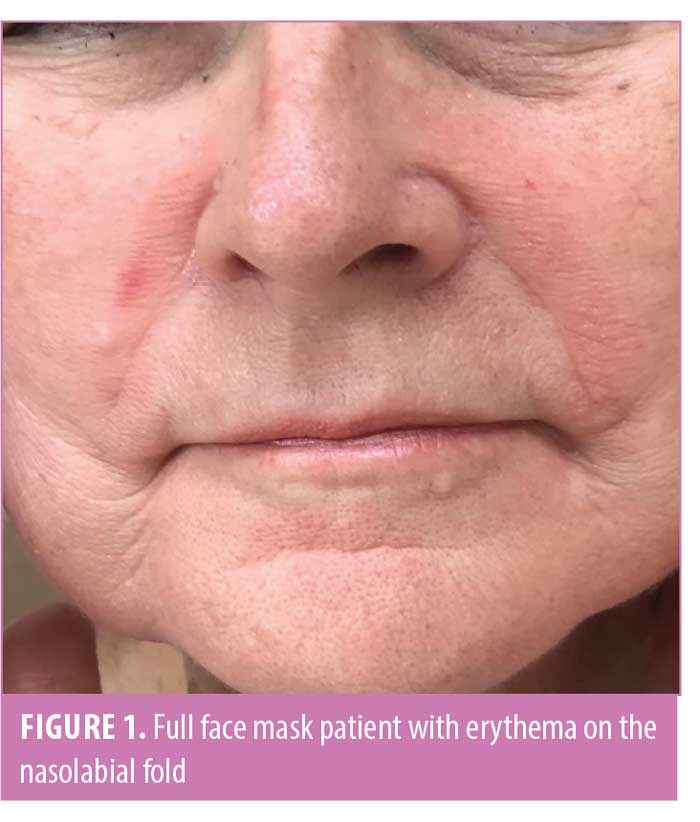
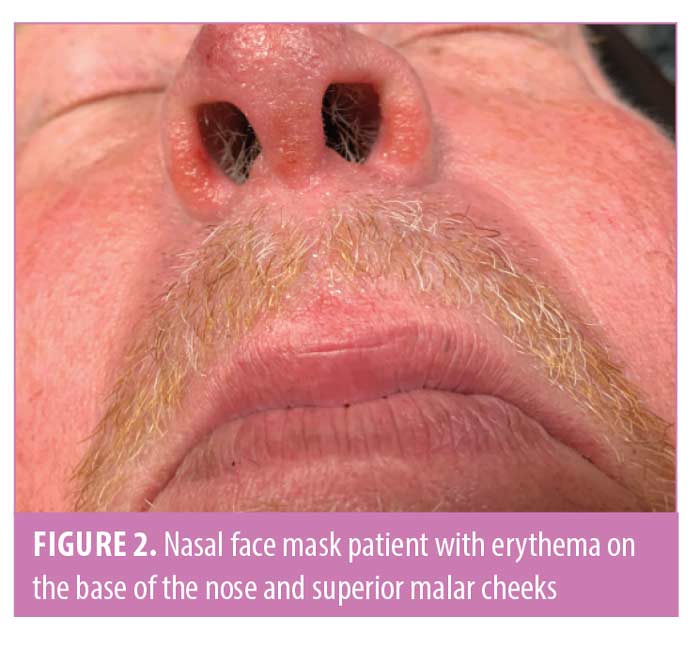
Physical examination revealed symmetric, scaling, well-demarcated, erythematous, and, in two cases, slightly indurated areas of skin involving the bilateral malar cheeks. The patient using the nasal mask also had irritation to the nostrils and columella. Tenderness to palpation was noted in a single case. No vesiculation, blistering, drainage, or sloughing was noted. The patients were all otherwise healthy and demonstrated no other similar skin changes.
Low to mid-potency corticosteroids were prescribed for two of the three patients, yielding little to no relief. Two of the three patients discussed the issue with their sleep apnea specialists and various equipment changes yielded no improvement. Further questioning revealed a deviation from the manufacturer recommendations regarding the use of the sanitizing devices. In all three cases, the CPAP masks were worn within one hour of completing the sanitizing cycle. Manufacturer recommendations suggest a minimum of four hours between completing disinfection and applying the CPAP to the skin.
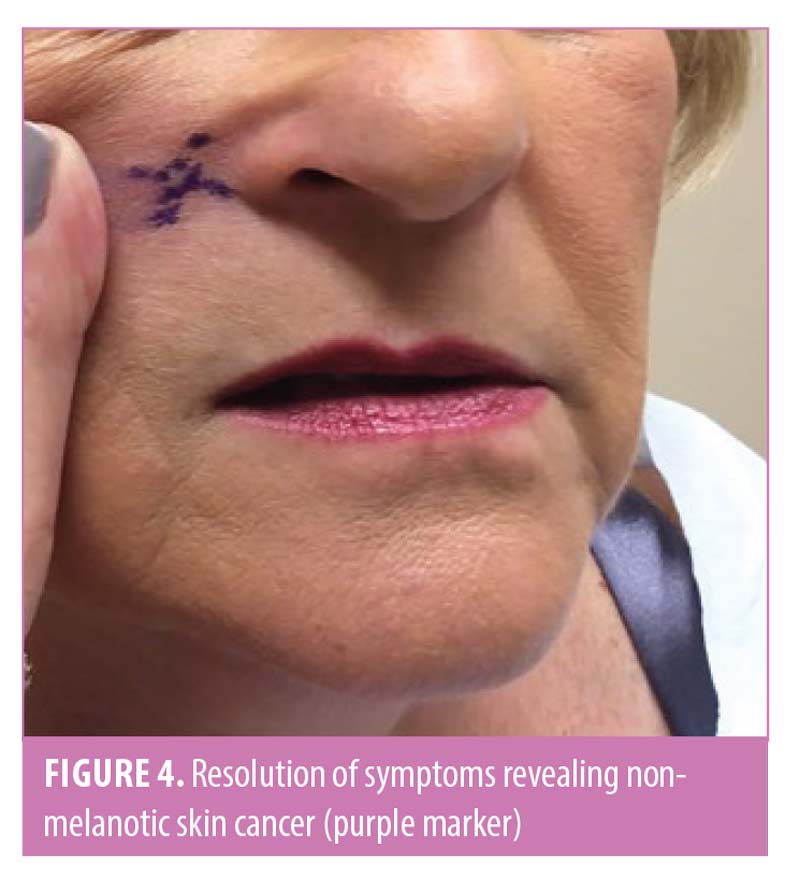
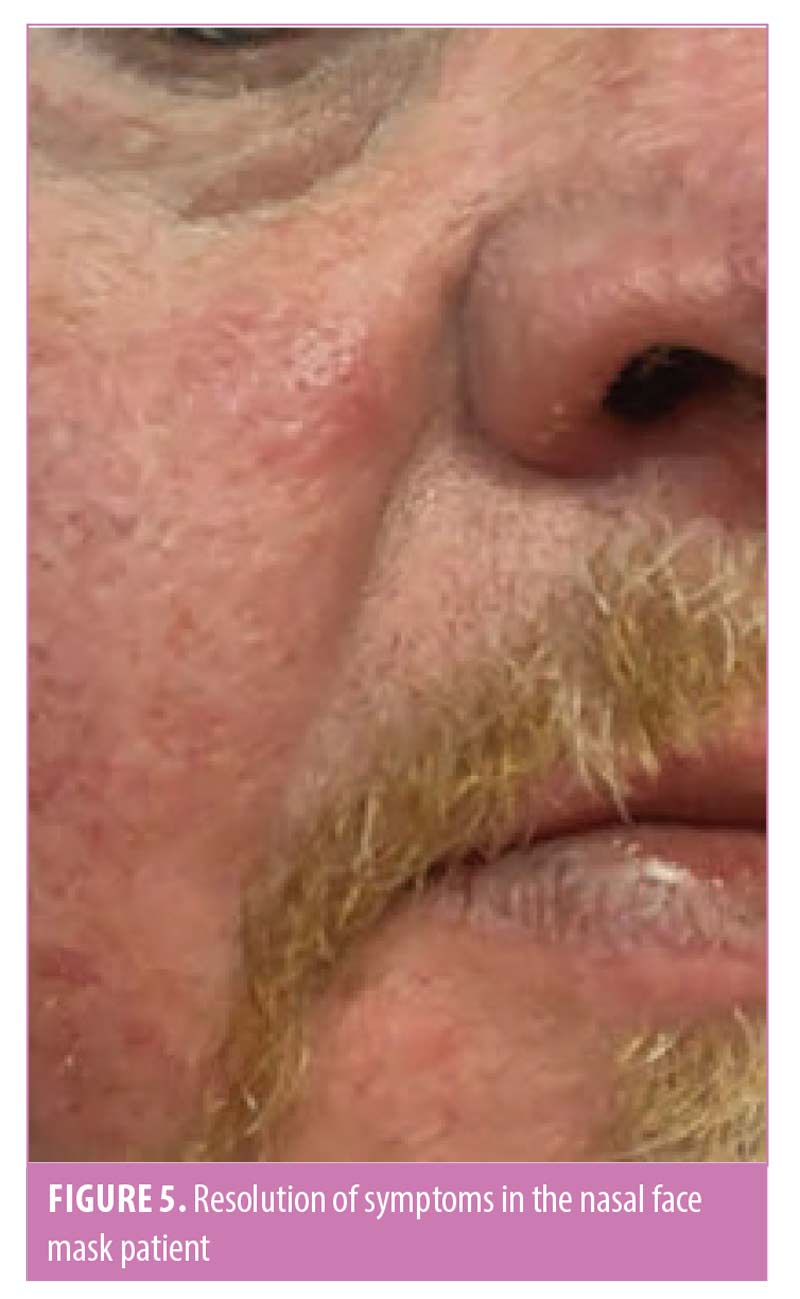
Each patient was instructed to lengthen the time between completion of the sanitizing cycle and application of the mask to a minimum of four hours. The patients continued using the same mask, straps, and sanitizing devices during this period of time. At follow-up, all three patients reported complete resolution of their symptoms within one to two weeks of the behavior modification (Figures 3 and 4). The only change made was in the amount of time before wear following the cleaning cycle, while the patients used their same mask, leading to the conclusion of irritant contact dermatitis secondary to a product from the activated oxygen devices.
Discussion
All three patients utilized similar activated oxygen devices to clean their CPAP machines. The patients sanitized their devices within one hour of sleep to clean the CPAP machines, allowing the device to remain in its container until the next use. The sealed container created an environment of minimal airflow. Ozone follows common gas laws such that its decay time can be considered in terms of its half-life. McClurken et al16 showed that, with minimal airflow, ozone requires approximately 1,524 minutes (25.4 hours) to decay one-half life when other factors are controlled. The half-life of ozone also decreases linearly with increasing temperature. The activated oxygen containers are a fixed environment that could be causing increased O3 residue on the CPAP machines. When a patient uses a CPAP machine daily, they may be replacing a mask that contains less than one half-life reduction of O3. The residual O3 can react with the natural oils on the individual’s skin to cause peri-oral dermatitis.17 Either increasing the temperature or opening the activated oxygen machines following use could remedy the above situation.
Ozone dermatitis has been observed in other commercial products. For example, one case series reported two patients who reacted to ozonated olive oil. Both patients had similar reactions to those reported for the patients considered in this study; in other words, they presented with well-demarcated irritant contact dermatitis. Both patients were patch tested, with one patient having a positive reaction to her oxygenated oil.18 The other patient had neither a reaction to oxygenated oil or plain olive oil. A control group of 20 people showed a 40-percent reaction rate to oxygenated olive oil. Squalene has been implicated as reacting with O3 on the epidermis to create periodical damage.17 Moreover, there is some evidence that O3 oils can suppress Th2-dominant cytokines and increase the suppression of interleukin-10. This process has been considered beneficial in inflammatory reactions, such as atopic dermatitis.19
Conclusion
Additional research should be carried out regarding the use of ozone. Currently, these devices are not approved by the United States Food and Drug Administration (FDA).20 The FDA has received 11 reports of cough, nasal irritation, headaches, and asthma attacks following use of CPAP disinfectors.20 It is possible that the above patients are not using their activated oxygen cleaning devices properly. A follow-up study determining the amount of ozone that remains after cleaning could be useful in determining how long patients should wait before using their masks. If the containers create an environment that prolongs the residence of the ozone residue, then an integrated flow system in the disinfecting machines could decrease the amount of ozone that remains on the mask and tubing. There is minimal research on the benefits that activated oxygen machines afford patients. These machines might be causing more harm than good when patients are not instructed on the proper use.
References
- Donovan LM, Boeder S, Malhotra A, Patel SR. New developments in the use of positive airway pressure for obstructive sleep apnea. J Thorac Dis. 2015;7(8):1323–1342.
- Patil SP, Ayappa IA, Caples SM, et al. Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE Assessment. J Clin Sleep Med. 2019;15(2):301–334.
- Sullivan C, Berthon-Jones M, Issa F, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;317(8225):862–865.
- D’Ambrosio D. Healthcare Startup Grows 2,805 Percent In 7 Years With CPAP Sanitizer. Available at: https://www.forbes.com/sites/danieldambrosio/2018/12/21/healthcare-startup-grows-2805-percent-in-7-years-with-cpap-sanitizer/#67d32fc05cfb. Accessed November 21, 2019.
- Marino M, Maifreni M, Baggio A, Innocente N. Inactivation of foodborne bacteria biofilms by aqueous and gaseous ozone. Front Microbiol. 2018;9:2024.
- Almaz ME, Sönmez IS. Ozone therapy in the management and prevention of caries. J Formos Med Assoc. 2015;114(1):3–11.
- Izadi M, Bozorgi M, Hosseine MS, Khalili N, Jonaidi-Jafari N. Health-related quality of life in patients with chronic wounds before and after treatment with medical ozone. Medicine (Baltimore). 2018;97(48):e12505.
- Pryor WA. Mechanisms of radical formation from reactions of ozone with target molecules in the lung. Free Radic Biol Med. 1994;17(5):451–465.
- Bonamonte D, Filoni A, Vestita M, et al. The role of the environmental risk factors in the pathogenesis and clinical outcome of atopic dermatitis. Biomed Res Int. 2019;2019:2450605.
- Di Mauro R, Cantarella G, Bernardini R, et al. The biochemical and pharmacological properties of ozone: the smell of protection in acute and chronic diseases. Int J Mol Sci. 2019;20(3):634.
- Song M, Zeng Q, Xiang Y, et al. The antibacterial effect of topical ozone on the treatment of MRSA skin infection. Mol Med Rep. 2018;17(2):2449–2455.
- Shin GA, Sobsey MD. Reduction of Norwalk virus, poliovirus 1, and bacteriophage MS2 by ozone disinfection of water. Appl Environ Microbiol. 2003;69(7):3975–3978.
- Gupta G, Mansi B. Ozone therapy in periodontics. J Med Life. 2012;5(1):59–67.
- Dyas A, Boughton BJ, Das BC. Ozone killing action against bacterial and fungal species; microbiological testing of a domestic ozone generator. J Clin Pathol. 1983;36(10):1102–1104.
- CPAPguide.net. Types of CPAP masks. Available at: https://cpapguide.net/types-of-cpap-masks/. Accessed November 21, 2019.
- Mcclurkin JD, Maier DE, Ileleji KE. Half-life time of ozone as a function of air movement and conditions in a sealed container. J Stored Prod Res. 2013;55:41–47.
- Wisthaler A, Weschler CJ. Reactions of ozone with human skin lipids: sources of carbonyls, dicarbonyls, and hydroxycarbonyls in indoor air. Proc Natl Acad Sci U S A. 2010;107(15):6568–6575.
- Aerts O, Leysen J, Horst N, Lambert J, Goossens A. Contact dermatitis caused by pharmaceutical ointments containing ‘ozonated’ olive oil. Contact Dermatitis. 2016;75(2):123–126.
- Lu J, Chen M, Gao L, et al. A preliminary study on topical ozonated oil in the therapeutic management of atopic dermatitis in murine. J Dermatolog Treat. 2018;29(7):676–681.
- Commissioner, O. (n.d.). FDA Reminds Patients that Devices Claiming to Clean, Disinfect or Sanitize CPAP Machines Using Ozone Gas or UV Light Have Not Been FDA Authorized. Available at: https://www.fda.gov/news-events/press-announcements/fda-reminds-patients-devices-claiming-clean-disinfect-or-sanitize-cpap-machines-using-ozone-gas-or. Accessed October 17, 2020.