J Clin Aesthet Dermatol. 2025;18(11):12–15.
by Robert J. Vanaria, BS; Aysham Chaudry, DO; and Mark S. Nestor, MD, PhD
Mr. Vanaria is with the Center for Clinical and Cosmetic Research in Aventura, Florida and the Hackensack Meridian School of Medicine in Nutley, New Jersey. Dr. Chaudry is with the Center for Clinical and Cosmetic Research in Aventura, Florida. Dr. Nestor is with the Center for Clinical and Cosmetic Research in Aventura, Florida, the Department of Dermatology and Cutaneous Surgery at the University of Miami Miller School of Medicine in Miami, Florida, and the Department of Surgery, Division of Plastic Surgery, University of Miami Miller School of Medicine in Miami, Florida.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
Abstract: Objective. Ultraviolet (UV) radiation is a major cause of nonmelanoma skin cancer (NMSC), including basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). Due to its demographics and geographic location, Florida’s population is at increased risk of NMSC. While historical epidemiology suggests BCC has a significantly greater incidence than SCC, a 2012 study in South Florida reported a reverse in this ratio, with significantly higher SCC rates, warranting further investigation. Methods. A South Florida dermatology database was analyzed for confirmed NMSC biopsy results from 2024. Lesions were categorized into BCC (superficial and nonsuperficial subtypes) and SCC (in situ SCC [isSCC] and invasive subtypes). Results. Among 856 NMSC lesions, 247 (28.9%) were BCC and 609 (71.1%) were SCC. Subtypes included 54 superficial BCC (6.3%), 193 nonsuperficial BCC (22.5%), 268 isSCC (31.3%), and 341 invasive SCC (39.8%). Discussion. These results align with earlier findings, contradicting the belief that BCC is the most common NMSC. SCC subtypes represented more than 70% of cases, suggesting a shift in incidence patterns. This trend may be linked to the early use of UV-B protection-dominant sunscreens, which offer less protection against UV-A, a significant factor in the development of SCC. Additionally, treating SCC-suspicious lesions as actinic keratoses in favor of biopsy for BCC-suspicious lesions may have contributed to prior findings. Conclusion. Our findings challenge traditional epidemiologic teachings, showing a higher incidence of SCC than BCC. These trends may reflect historical photoprotection and/or changing biopsy practices. Keywords: Basal, epidemiology, incidence, nonmelanoma, photoprotection, squamous, sunscreen, ultraviolet
Introduction
Nonmelanoma skin cancer (NMSC) is the most prevalent form of cancer in the United States, with an estimated 5.4 million cases diagnosed annually.1 Ultraviolet (UV) radiation exposure is a well-established risk factor, associated with approximately 90% of NMSCs.2 Because of its location as one of the most southernmost states in the United States, Florida has one of the highest incidences of skin cancer in the world, ranking second in the nation for new cases.3 One study that analyzed lesions from 65 dermatology centers documented rates that suggest South Florida may have the highest incidence rate of NMSC globally.4 Traditionally, basal cell carcinoma (BCC) has been considered the most common form of NMSC by number of diagnoses, followed by squamous cell carcinoma (SCC), with an approximate ratio of 70:30.5 This long-held belief has shaped dermatologic education and clinical practice for decades. However, recent studies have begun to challenge this conventional representation, particularly in regions with high UV exposure like South Florida.
Two studies published in 2012, one specific to South Florida, reported extremely high overall rates of NMSC in addition to a reversed ratio of SCC to BCC, prompting a reevaluation of NMSC epidemiology, particularly in high-risk populations.4,6 This unexpected finding raises questions about potential shifts in NMSC incidence patterns and the factors driving such changes. Since BCC is associated with greater UV-B exposure and SCC with UV-A exposure, possible explanations for this trend include the historical use of UV-B protection-dominant sunscreens, which may, and likely do, offer less protection against UV-A radiation as well as evolving biopsy practices among dermatologists.7-9
Given Florida’s unique demographic composition, including a large elderly population, and its geographic location conducive to year-round sun exposure, understanding the current landscape of NMSC in this region is crucial for public health strategies and clinical practice.10 The aging population is particularly relevant, as the risk of developing skin cancer is directly related to and increases with age.11
This study aims to examine the current incidence patterns of NMSC, with a particular focus on the relative frequencies of BCC and SCC subtypes. By analyzing a comprehensive dermatology database from a South Florida dermatology practice in 2024, we seek to provide updated insights into the epidemiology of NMSC in a high-risk population. Our findings may have significant implications for skin cancer prevention, screening, and management strategies not just in South Florida, but also in similar high-risk regions worldwide and for those who frequent these locations.
Methods
This cross-sectional study analyzed data from a dermatology clinical practice database located in South Florida. The study period covered the full year of 2024 and included patients of all ages who underwent skin biopsies. We searched the electronic database associated with the practice to retrieve histologically confirmed NMSC biopsy results. Only biopsy-proven NMSC diagnoses were included in the analysis.
Lesions were categorized into two main types: BCC and SCC. These were further divided into the following subtypes: superficial BCC, nonsuperficial BCC (including nodular, morpheaform, and others), in situ SCC (isSCC), and invasive SCC (including superficially invasive SCC, invasive SCC, and SCC keratoacanthoma type). The retrieved biopsy results were then sorted and counted according to their classification. Descriptive statistics were used to summarize the frequency and percentage of each NMSC type and subtype. The relative proportions of BCC and SCC were compared to assess the predominant type of NMSC in the study population.
Results
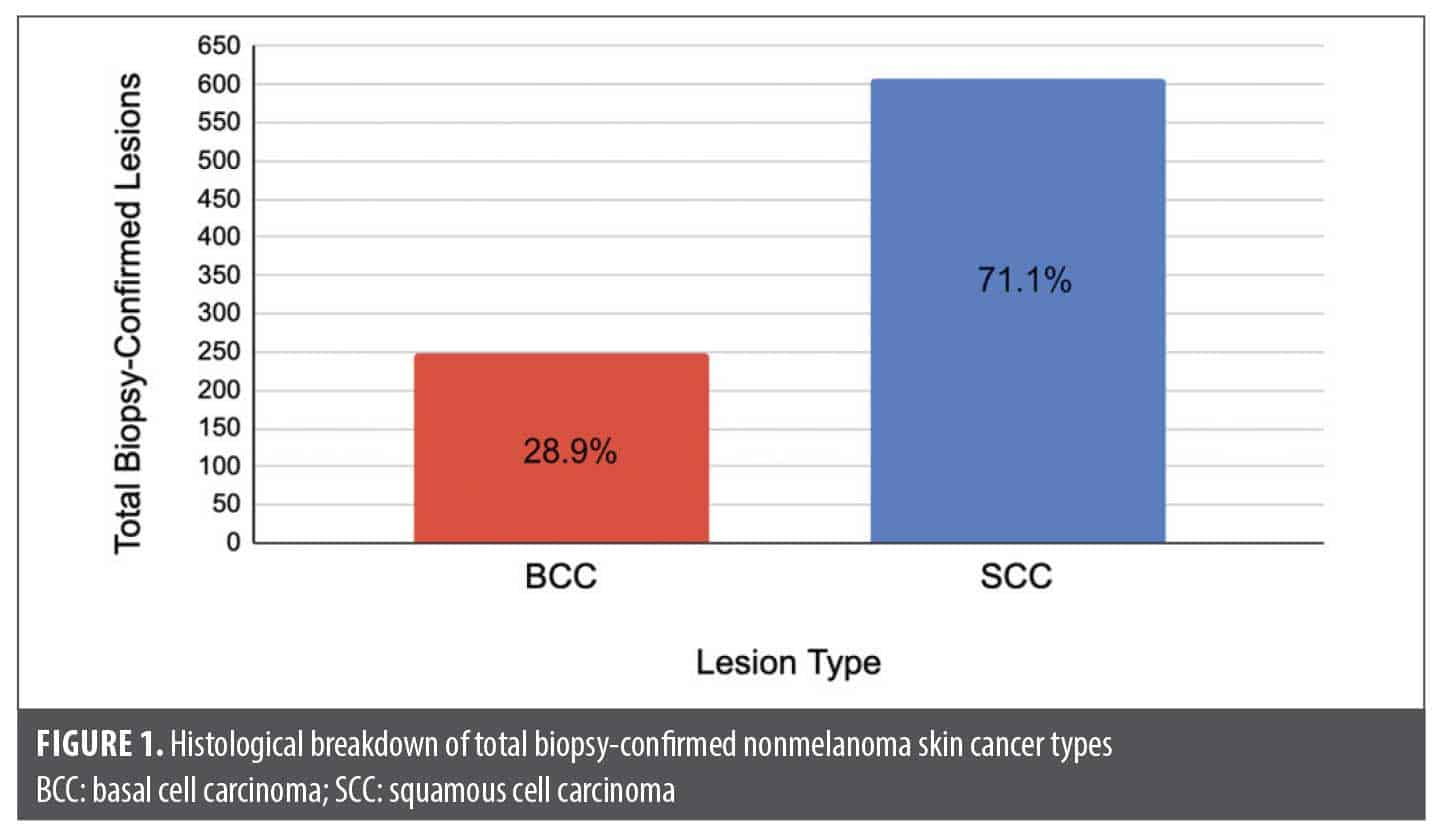
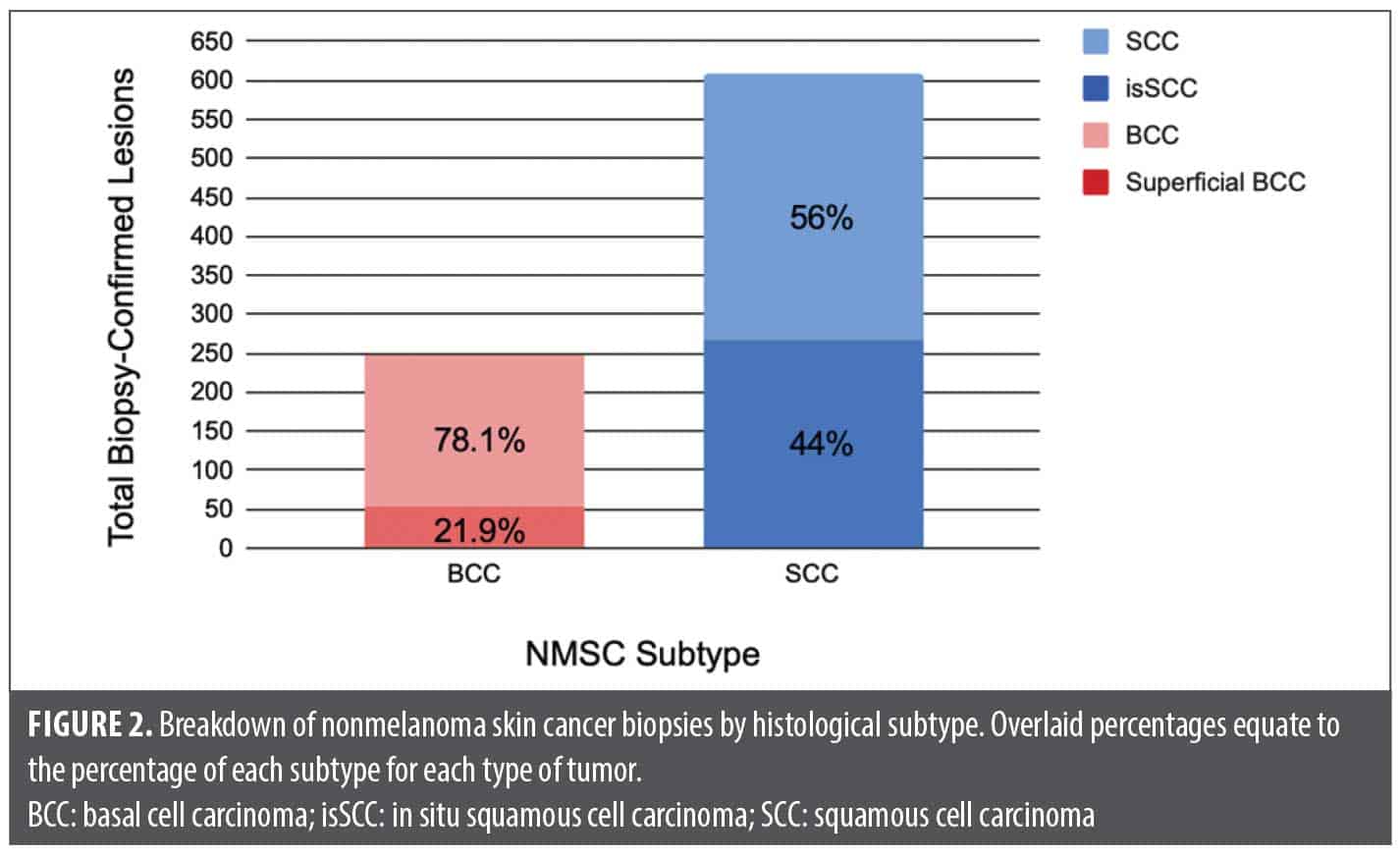
A total of 856 biopsy-proven NMSC lesions were identified and analyzed from the database. The distribution of NMSC types and subtypes is shown in Figures 1 and 2.
These results demonstrate a significantly high proportion of SCC compared with BCC in the study population (Figure 1). SCC subtypes represented more than 70% of all biopsy-confirmed cutaneous cancers, with invasive SCC being the most common subtype overall. Within the BCC category, invasive types (including nodular, morpheaform, and others; n=193) were more prevalent than superficial BCC (n=54), accounting for 78.1% of BCC lesions. For SCC, invasive lesions slightly outnumbered isSCC (n=268), representing 56.0% of all SCC cases (n=341). The high proportion of isSCC (44.0% of SCC cases) is noteworthy and may reflect early detection practices (Figure 2).
Discussion
Our findings challenge the traditional understanding of NMSC epidemiology, which has long held that BCC is the most common form of skin cancer by incidence rate. In our population, SCC subtypes were found to be more than twice as common as BCC subtypes. These findings align with the two previously mentioned studies, both of which reported higher rates of SCC compared with BCC.4,6 This consistent pattern suggests a potential shift in NMSC incidence in high-risk populations, particularly in regions—in this case South Florida—with intense UV exposure.
We hypothesize that several factors may contribute to this observed trend. First, the shift in incidence rate could be due to increased exposure to UV-A as a result of the historical use of UV-B-dominant sunscreens. It is well documented that UV-A is more strongly associated with SCC development while UV-B is more strongly associated with BCC development.12-15 Specific patient populations, such as those who have received transplants or psoralen–UV-A (PUVA) therapy, have been known to have a high incidence of SCC. PUVA involves a high dose of UV-A, and multiple studies, including a meta-analysis, have demonstrated a significantly higher incidence of SCC specifically in patients who received any dose of PUVA than any other cutaneous neoplasms.13 Further, due to their medication-induced chronic immunosuppression, patients who have received transplants with a history of significant sun exposure are at an increased risk of SCC.16-19 This can also accelerate the timeline for SCC development, as typical immune surveillance is hindered, demonstrating the importance of biopsy and histologic confirmation of SCC early in its development. Furthermore, since actinic keratoses (AK) have a very high incidence in this patient population and are known precursors to SCC, the increase in AKs can be a driving factor for the relative increase in SCC appearance.4 This factor also makes the case for aggressive treatment and field therapy for AKs.
In the past, UV-B-dominant sunscreens were more common than broad-spectrum sunscreens, potentially leaving patients more vulnerable to UV-A exposure and therefore increased risk for SCC development.20 This effect was compounded by the prevention of sunburn by selectively blocking UV-B, allowing patients to stay out in the sun longer and be exposed to a greater dose of UV-A radiation. Presently, data still suggest sunscreens, including those labeled as “broad-spectrum,” may not do an adequate job of protecting against UV-A radiation.9,21
The timeline of historical UV-B-dominant sunscreen use is paramount, as the development of SCC, although nonlinear and dependent on a multitude of patient-specific factors, takes years following UV exposure.22 The importance of broad-spectrum protection has become increasingly recognized in recent years. Current recommendations emphasize the use of sunscreens that protect against both UV-A and UV-B radiation.23,24 However, the long-term effects of historical UV-B-specific sunscreen use may still be reflected in our current NMSC incidence patterns.
Another factor that could contribute to the discrepancy between epidemiologic teachings and our findings is biopsy practices. Under the current NMSC epidemiology teachings, dermatologists are trained to anticipate more BCC-suspicious lesions and fewer SCC-suspicious lesions, resulting in fewer biopsies of SCC in favor of BCC, especially for superficial or in situ lesions that may not clinically differ from hypertrophic AKs. When dermatologists encounter hyperkeratotic suspicious lesions, many are presumed to be hypertrophic AKs and treated with liquid nitrogen freezing rather than biopsy. This bias in biopsy practices could also contribute to prior misconceptions about the relative frequencies of BCC and SCC.
It is important to note that while our study focused on a South Florida population, the implications of our results are relevant to other high-risk regions. Florida has the second highest incidence of melanoma in the United States, suggesting a generally elevated risk for all types of skin cancer in this geographic location and similar areas.25 Our findings underscore the need for effective broad-spectrum sun protection that guards against both UV-A and UV-B radiation, and they also highlight the importance of reconsidering current approaches to skin cancer screening and biopsy practices to ensure accurate representation as well as appropriate treatment of NMSC subtypes.
Future research should focus on validating these findings across multiple centers as well as investigating the long-term impact of different sunscreen formulations on NMSC incidence patterns. Additionally, efforts to improve public awareness about the importance of comprehensive UV protection as well as treatment of precancerous AKs are crucial in light of these results.
Conclusion
Our findings confirm previous studies and challenge traditional epidemiologic teachings by demonstrating a higher incidence of SCC subtypes compared with BCC subtypes. This trend contradicts the long-held belief that BCC is the most common form of skin cancer by incidence rate. Several factors may contribute to this shift, including historical patterns in the use of UV-B-specific photoprotection, increased incidence of precancerous AKs, and biopsy practices. Dermatologists should be aware of this trend and maintain a higher vigilance when screening for SCC, particularly in high-risk populations.
References
- Basal & squamous cell skin cancer statistics. American Cancer Society. October 31, 2023. Accessed February 18, 2025. https://www.cancer.org/cancer/types/basal-and-squamous-cell-skin-cancer/about/key-statistics.html
- Narayanan DL, Saladi RN, Fox JL. Ultraviolet radiation and skin cancer. Int J Dermatol. 2010;49(9):978-986.
- Guy GP Jr, Thomas CC, Thompson T, Watson M, Massetti GM, Richardson LC. Vital signs: melanoma incidence and mortality trends and projections – United States, 1982-2030. MMWR Morb Mortal Wkly Rep. 2015;64(21):591-596.
- Nestor MS, Zarraga MB. The incidence of nonmelanoma skin cancers and actinic keratoses in South Florida. J Clin Aesthet Dermatol. 2012;5(4):20-24.
- Leiter U, Keim U, Garbe C. Epidemiology of skin cancer: update 2019. Adv Exp Med Biol. 2020;1268:123-139.
- Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. population, 2012. JAMA Dermatol. 2015;151(10):1081-1086.
- Seité S, Fourtanier A, Moyal D, Young AR. Photodamage to human skin by suberythemal exposure to solar ultraviolet radiation can be attenuated by sunscreens: a review. Br J Dermatol. 2010;163(5):903-914.
- Weinstock MA, Lott JP, Wang Q, et al. Skin biopsy utilization and melanoma incidence among Medicare beneficiaries. Br J Dermatol. 2017;176(4):949-954.
- Andrews DQ, Rauhe K, Burns C, et al. Laboratory testing of sunscreens on the US market finds lower in vitro SPF values than on labels and even less UVA protection. Photodermatol Photoimmunol Photomed. 2022;38(3):224-232.
- Schmitt J, Seidler A, Diepgen TL, Bauer A. Occupational ultraviolet light exposure increases the risk for the development of cutaneous squamous cell carcinoma: a systematic review and meta-analysis. Br J Dermatol. 2011;164(2):291-307.
- Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7(2):1-6.
- Armstrong BK, Kricker A. The epidemiology of UV induced skin cancer. J Photochem Photobiol B. 2001;63(1-3):8-18.
- Stern RS; PUVA Follow-Up Study. The risk of squamous cell and basal cell cancer associated with psoralen and ultraviolet A therapy: a 30-year prospective study. J Am Acad Dermatol. 2012;66(4):553-562.
- Man I, Crombie IK, Dawe RS, Ibbotson SH, Ferguson J. The photocarcinogenic risk of narrowband UVB (TL-01) phototherapy: early follow-up data. Br J Dermatol. 2005;152(4):755-757.
- Sun, UV rays and cancer. World Cancer Research Fund. Accessed February 19, 2025. https://www.wcrf.org/preventing-cancer/topics/sun-uv-rays-and-cancer/
- Krynitz B, Edgren G, Lindelöf B, et al. Risk of skin cancer and other malignancies in kidney, liver, heart and lung transplant recipients 1970 to 2008—a Swedish population-based study. Int J Cancer. 2013;132(6):1429-1438.
- Rangwala S, Tsai KY. Roles of the immune system in skin cancer. Br J Dermatol. 2011;165(5):953-965.
- Harwood CA, Toland AE, Proby CM, et al; KeraCon Consortium. The pathogenesis of cutaneous squamous cell carcinoma in organ transplant recipients. Br J Dermatol. 2017;177(5):1217-1224.
- Euvrard S, Kanitakis J, Claudy A. Skin cancers after organ transplantation. N Engl J Med. 2003;348(17):1681-1691.
- Garland CF, Garland FC, Gorham ED. Rising trends in melanoma. An hypothesis concerning sunscreen effectiveness. Ann Epidemiol. 1993;3(1):103-110.
- Coelho SG, Rua D, Miller SA, Agrawal A. Suboptimal UVA attenuation by broad spectrum sunscreens under outdoor solar conditions contributes to lifetime UVA burden. Photodermatol Photoimmunol Photomed. 2020;36(1):42-52.
- Squamous cell carcinoma risk factors. Skin Cancer Foundation. January 2025. Accessed February 19, 2025. https://www.skincancer.org/skin-cancer-information/squamous-cell-carcinoma/scc-causes-and-risk-factors/
- Wang SQ, Xu H, Stanfield JW, Osterwalder U, Herzog B. Comparison of ultraviolet A light protection standards in the United States and European Union through in vitro measurements of commercially available sunscreens. J Am Acad Dermatol. 2017;77(1):42-47.
- Demehri S. Preventing skin damage from UVA and UVB rays. Mass General Brigham. September 22, 2023. Accessed February 19, 2025. https://www.massgeneralbrigham.org/en/about/newsroom/articles/uva-and-uvb-ray-differences
- Melanoma by the state: Florida. AIM at Melanoma Foundation. March 6, 2018. Accessed February 19, 2025. https://www.aimatmelanoma.org/melanoma-state-florida/